Accepted on 28 Dec 2020
Submitted on 01 Dec 2020


Hydatidosis is a condition characterized by the presence of cysts produced by Echinococcus granulosus. It is common in places where cattle and swine are practiced, and in Mediterranean countries, South America, New Zealand and the Middle East. It is estimated that one million people are infected around the world [1] and the incidence is 2/100,000 [2]. The most common site of localization is the liver in 70 percent, in the right lobe; In order of frequency, the thorax is found in up to 20 percent of cases, and simultaneously in 5–13 percent of cases; less common locations are spleen (6%), bones/muscles (4%), kidney (2%), heart (2%), brain (1%), and others (2%) [3]. It has been reported that between 7.4% [4] and 10.5% of intrathoracic hydatid cysts are extrapulmonary; locations can be the pleura, mediastinum, pericardium, and diaphragm, with the pleural cavity being the most commonly involved site, with 57% of cases [5]. For a long time Dévé et al and other authorities on hydatidosis considered that primary pleural hydatidosis was only the result of cysts that migrate or rupture through the diaphragm from the liver or bronchi into the pleura, in 2 percent and 8 percent, respectively; likewise, it was suggested that the only form of hydatid cysts in the pleural cavity was forming part of a compound of heterotopic disease that simultaneously affected 2 different organs, however, the cases presented by Finocchietto demonstrated the presence of primary pleural hydatidosis [6].
Primary pleural hydatidosis occurs in 1.4%–3.4% of all cases of echinococcal infection, making it extremely rare, even in countries where it is considered an endemic infection [7]. The location of the pleural cysts can be on the pulmonary fissures in 54.6% or properly immersed in the pleural space in 13.3%, they are more commonly found on the right side (41%) [8]. Before considering that it is a primary pleural hydatidosis, it is necessary to rule out the simultaneous location of hydatid cysts in another site, for example, the liver or the lung. Primary pleural hydatidosis most commonly affects men between the third and fifth decades of life. The clinical presentation is widely variable, from asymptomatic patients to unusual presentations such as pyoneumothorax [9] or simulating a phantom tumor [10]. The diagnosis of the hydatid cyst can be an imaging finding. Given its low incidence, hydatidosis is not usually considered within the differential diagnoses of pleural disease, therefore cases of intrathoracic hydatid cysts, especially extrapulmonary intrapleural cysts, represent a diagnostic challenge, because their rupture sometimes brings life-threatening complications. as anaphylactic shock. Treatment is based on aspiration of the contents and surgical resection of the intact cyst or residual membranes, with washing of the cavity and treatment with antiparasitics. Finally, patients may need to be followed up to detect recurrences early.
A 26-year-old Mexican woman, non-smoker, with no significant medical or surgical history began with a one-day-old fever, with no other accompanying symptoms. She was taken to the emergency room where she works. During the physical examination, no abnormality was detected. She denies a history of trauma, or a previous presentation of fever. Due to the current situation, tests were performed to rule out the diagnosis of SARS-CoV-2 infection, a nasal swab for RT-PCR was performed, with a negative result; and the taking of a chest computed tomography, which showed in an axial cut a lesion with lobulated edges in its anterior portion and smooth in its posterior part, presenting intimate contact with the 5th and 6th right vertebral bodies, respecting the cortical axes with larger than 42 mm × 16 mm (Figure 1.A). The application of intravenous contrast medium did not present reinforcement compared to the simple phase (Figure 1.B). The remaining studies performed were normal. Informed consent was obtained before starting treatment. The biopsy was scheduled for analysis of the lesion. The procedure begins, with the patient in the prone position, with an 18 g × 20 cm coaxial cutting needle with which 5 unsuccessful tissue samples are taken. It is aspirated through the coaxial of the previously placed needle and in the post-aspiration control a collapse of 90% of the lesion is observed. The volume of material obtained was 10 ml of very viscous consistency, 5 ml of liquid mixed with absolute alcohol were sent for cytological study and 5 ml for culture (Figure 1.C). Four smears were made that were stained with H&E for cytological study. Post-fixation, friable yellow-white material is obtained that is included in two capsules for histological study. In the histological sections of the cell blocks, abundant concentric sheets of amorphous proteinaceous material are observed that correspond to the cuticle, which in different areas alternates with calcareous corpuscles (Figure 2.A) and hooks (Figure 2.B). In the smears, few mature lymphocytes and macrophages of foamy cytoplasm are observed. Lung parenchyma, other pathogens, or morphological data of malignancy were not identified. The diagnosis was hydatid cyst. The patient was discharged with treatment for Echinococcus granulosus, subsequent medical appointments were established. Currently the patient is asymptomatic with a satisfactory evolution.
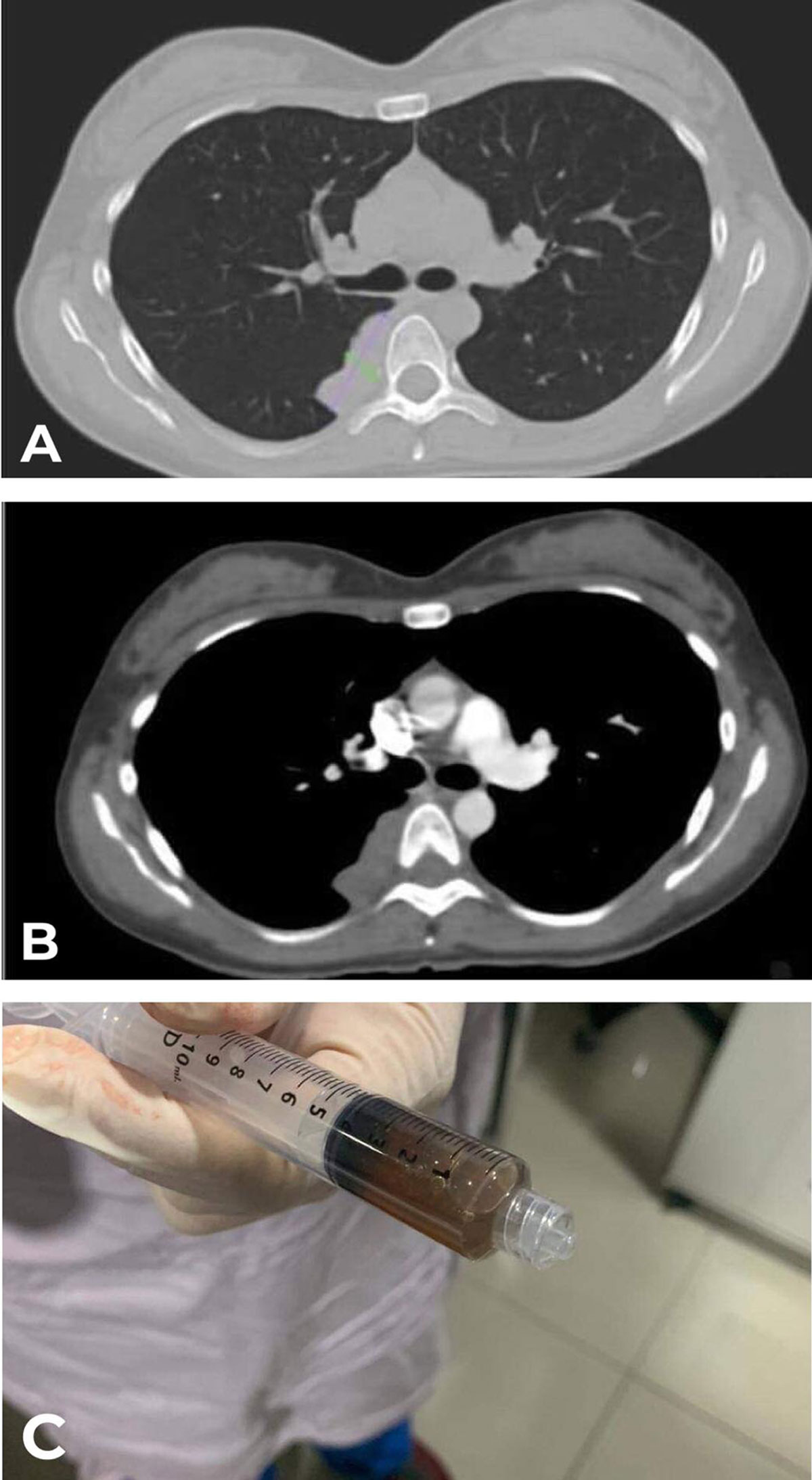
A) TC Anterior lobulated and posterior smooth lesion, adjacent to the 5th and 6th right vertebral bodies, respecting the cortical axes with larger than 42 mm × 16 mm. B) The application of intravenous contrast medium did not present reinforcement compared to the simple pase. C) Material obtained was 10 ml of very viscous consistency. Photo: Jorge Guerrero- Ixtlahuác. Reproduced with permission of the photographer.
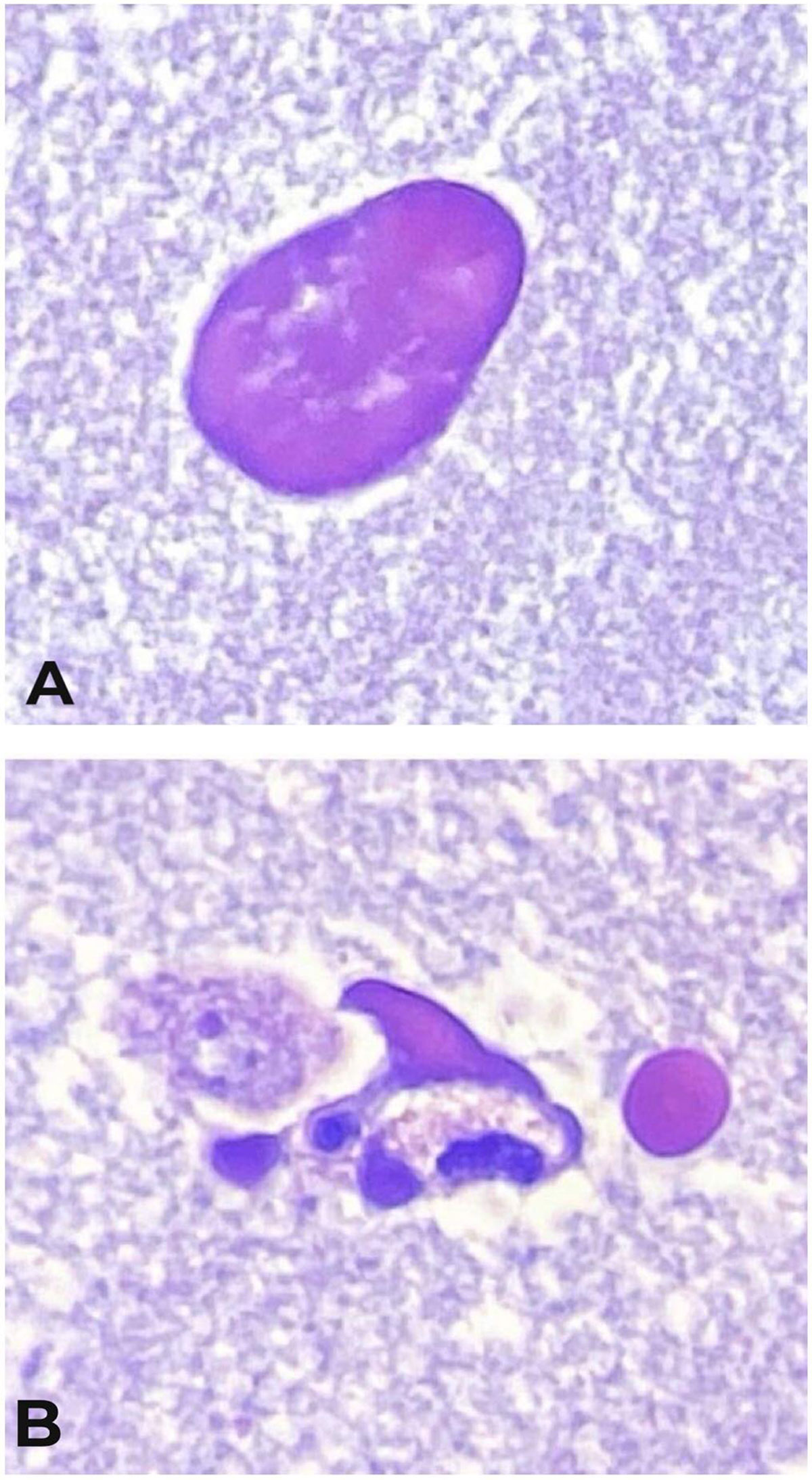
A) Echinococcus granulosus: concentric sheets of amorphous proteinaceous material that correspond to the cuticle, in different areas alternates with calcareous corpuscles. B) Hooks of E. granulosus. Photo: Fredy Chablé-Montero. Reproduced with permission of the photographer.
Primary pleural hydatidosis is a rare pathological entity even in endemic countries for infection by Echinococcus granulosus [11], it is produced by the ingestion of parasite eggs in food or water contaminated with dog faeces or from sheep breeding sites. which are the main host, the human, is just an accidental reservoir. Once ingested they can migrate to the intrathoracic vessels [10]. The hexacanth embryo crosses the duodenal wall towards the portal circulation or the perigastric and periduodenal lymphatic vessels, which connect with the thoracic lymphatic duct, through which it affects the thoracic cavity. The reason why the embryo evades the liver parenchyma through its passage in the portal vein remains unknown, however, it is estimated that 15–20% of embryos [12] are capable of passing into the pulmonary circulation, which it constitutes the second barrier before reaching the aorta and being able to spread to any organ through the systemic circulation, even to the small and multiple capillaries that supply the pleural tissue. Knowledge of this form of dissemination makes it possible to consider that the pleura may be affected without secondary pleural hydatidosis due to rupture or contiguity. These cysts are considered primary when they are produced directly by the migration and fixation of the embryo directly released from the egg ingested by the host in a specific organ, in this case the pleura. Secondary cysts are formed by migration of daughter vesicles, scolexes, or other fertile perennial hydatid elements that migrate after the primary cyst rupture to other organs [13].
Once the embryo is fixed, it has the ability to form the vesicle, which is first unique and then can be multiple, they grow 2 to 3 cm per year, can take a long time from infection until symptoms appear, it can even be only an imaging finding when a patient is routinely evaluated for other comorbidities [14], or simulating an infectious respiratory disease with mild and nonspecific symptoms of short evolution, as in the present case. Symptomatic patients with intrathoracic hydatid cysts can do so through a wide variability of clinical data, including cough (54%), chest pain (36%), dyspnea (25%), hemoptysis (19%)), fever and chills (10%), hydatidemesis (10%), pleurisy (5%), and spontaneous pneumothorax [15]. Symptoms can be more commonly located on the right side because most extrapulmonary intrathoracic hydatid cysts are anchored to a pedicle from the wall, are more common on that side, are rarely bilateral, and up to 30% may be asymptomatic [2].
Given the rarity of primary pleural cysts, it has been difficult to establish a clinical characterization, especially because the manifestations that have been described in the reported cases do not allow accurate identification of whether it is a primary pleural cyst due to hydatidosis, including some of they, like pleural effusion, can simulate the rupture of a primary one elsewhere within the pleural space. In the case presented here, the patient only had a short-term fever, which did not lead to a specific diagnosis, due to the current global situation of the SARS-CoV-2 pandemic and her occupational exposure, the approach began ruling out this infection. with a swab that gave a negative result, as well as a chest X-ray without alterations, for which a tomography was requested where the lesion was evidenced.
There are several case reports that show the individual importance of the diagnosis of primary pleural hydatidosis. We conducted an analysis of the literature (ScienceDirect, Medline, Pubmed, SCOPUS) from 1920 to 2020 using the key words: “pleural hydatidosis; primary hydatid cyst AND pleura; primary pleural echinococcosis; case report” (Table 1), to try to identify the clinical presentations most associated with the presence of primary pleural hydatid cysts. The wide variability of the presentation in the case reports increases the level of difficulty in the diagnostic suspicion, however, the constant presence of symptoms that affect the respiratory system and sometimes the fever remains.
Table 1
Case reports of primary pleural hydatidosis. Literature review of 100 years.
| AUTOR | YEAR | CASES | SEX | AGE | CLINICAL PRESENTATION | LOCALIZATION | COUNTRY |
|---|---|---|---|---|---|---|---|
| Hashimi et al [16] | 2019 | 1 | Man | 10 years old | Severe chest pain, high-grade fever, dyspnea and shortness of breath for 3 months, dry cough and anorexia | Multiple cysts occupying the entire intrapleural space on the right side | Pakistan |
| Oncel et al [17] | 2018 | 1 | Man | 20 years old | Dyspnea | Effusion plus opacity floating in pleural space | Turkey |
| Mrabet et al [18] | 2018 | 2 | Woman | 17 years old | Right chest pain and tightness for 3 months, mMRC stage III dyspnea, some episodes of low-volume hemoptisis | Garbhi type II right pleural cyst | Morocco |
| Man | 28 years old | Asymptomatic | Left mediastinal pleura | Morocco | |||
| Kalra et al [1] | 2018 | 1 | Man | 31 years old | Shortness of breath, cough and significant weight loss for six months and fever for three months | Loculated left massive pleural effusion | India |
| Amini et al [19] | 2018 | 1 | Man | 79 years old | Dyspnea, non-productive cough, fatigue, and weight los | Left massive pleural effusion with cystic inclusions | Iran |
| Mardani et al [20] | 2017 | 1 | Woman | 33 years old | Dyspnea, cough, chills | Right, multiple | Iran |
| Badji et al [21] | 2017 | 2 | Woman | 13 years old | Fever, thoracic deformity with right basytoracic wound in midclavicular line due to anterior effusion and right pleural effusion syndrome | Right mediastinal pleura and multiple cystic formations in a minor fissure. Extension of lesions to the diaphragm and adjacent soft tissues | Senegal |
| Man | 14 years old | Asymptomatic, fistulized mass on the right flank, leaving a whitish fluid with streaks of blood. | Right mediastinal pleura and minor fissure, multiple cystic formations. Extension of lesions to the diaphragm and adjacent soft tissues | Senegal | |||
| Kumar et al [11] | 2016 | 1 | Man | 24 years old | Left pain, dry cough and dyspnea 2 months | Pneumothorax and multiple left pleural cysts | India |
| Alakhras et al [22] | 2016 | 1 | Woman | 36 years old | Chronic productive cough in the morning, chest pain, dyspnea NYHA ll. | Parietal pleura posterior superior segments of the right lung. | Syria |
| Akkas et al [23] | 2015 | 1 | Man | 24 years old | Asymptomatic | 6th right rib attached to the pleura | Turkey |
| Erkoc et al [24] | 2014 | 1 | Man | 73 years old | Sudden shortness of breath, incisor pain in the left chest with decreased breath sounds | Left pleural effusion | Turkey |
| Ekinci et al [25] | 2013 | 1 | Man | 32 years old | Left pleuritic pain and sweating for 15 days. Exuding pleural effusion | Left costodiaphragmatic groove | Turkey |
| Vaidesswar et al [26] | 2012 | 1 | Man | 20 years old | Left chest pain, 15 days ago, cough, fever. Massive left pleural effusion | Left, multiloculate | India |
| Jana et al [9] | 2012 | 1 | Woman | 35 years old | Pioneumothorax, respiratory distress, intermittent fever, mild right chest pain for 3 months, dry cough for 2 years, empyema | Right hydropneumothorax, ruptured hydatid cyst as a sign of air bubble, double wall together with multiple daughter cysts. | India |
| Kim et al [14] | 2011 | 1 | Man | 50 years old | Asymptomatic | Lateral arch of the 7th and 8th right ribs with internal fat density | Korea |
| Singh et al [27] | 2010 | 1 | Woman | 37 years old | Persistent dry cough and recurrent pleural effusion, developed empyema after 10 months of antituberculous treatment | Multiple liquid collections and septa in the left pleural cavity, extending along the costal, mediastinal, and diaphragmatic pleura | India |
| Canpolat et al [10] | 2010 | 1 | Woman | 26 years old | Pain in the right pectoral, stabbing and increasing with movement, dyspnea on exertion and productive cough. | Collection of cystic fluid located in the right major fissure, compatible with a phantom tumor | Turkey |
| Tewari et al [28] | 2009 | 1 | Woman | 28 years old | Six-month left non-painful lump at the level of the 7th–8th rib | Lower part of the left lung that lines the left dome of the diaphragm | India |
| Harzalla et al [13] | 2007 | 1 | Man | 43 years old | Right basal chest pain for 3 months | Homogeneous and well limited right axillary opacity with peripheral calcification | Morocco |
| Mbatchou et al [29] | 2004 | 1 | Woman | 16 years old | Dry cough, dyspnea, polypnea, right chest pain for 3 months | Right apical opacity excavated at the air-fluid level. | Senegal |
| Antona et al [30] | 1979 | 1 | – | – | Continuous pain in the right hemithorax, decreased mobility of the hemithorax, dull to percussion and abolished transmission of sounds, chills, fever and vomiting. | Giant opacity in the right hemithorax | Spain |
| Jesiotr et al [6] | 1972 | 1 | Man | 21 years old | Fever, cough, pain in right chest, marked shortness of breath, mildly productive cough, vomiting. Right hydropneumothorax. | Right costodiaphragmatic sinus | Israel |
The importance of performing imaging studies in the approach of a patient with respiratory symptoms is essential to try to determine if the cause is, for example, an infectious or neoplastic process. In the case of hydatidosis, multiple techniques have been used to describe the characteristics of the cysts, however, there are still difficulties for identification. The chest x-ray can only show the presence of calcified cysts.
Ultrasound is the most sensitive technique to identify hydatid membranes, septa and sand inside the cyst; it is seen as a rounded, smooth anechoic cyst [15]. Due to their characteristics, they can be classified based on the WHO or Gharbi criteria, classifications with which treatment can be guided [31, 32]. A homogeneous round or oval density can be seen on computed tomography, demonstrating calcification of the cyst wall. Magnetic resonance imaging shows the characteristic hypointense T2-weighted ring. Some injuries may not even be identified until direct visualization during the surgical procedure.
A complicated issue of the name of primary pleural hydatid cyst is to guarantee objectively through imaging, mainly, the absence of cysts in other locations that could suggest that the presence of hydatid cysts in the pleural space is rather due to a secondary or heterotopic dissemination, in the literature there are some reported cases where we can find pleural hydatid cysts without evidence of cyst in another organ but with a history of hydatid cyst intervened several years ago [33, 34, 35]; on other occasions, the presence of an apparently primary pleural cyst is accompanied by cysts in other intrathoracic locations, even with evidence that the pleural cyst is not produced by the rupture of a pulmonary cyst, forming the entity recognized as heterotopic pleuropulmonary hydatidosis [13].
Abnormalities in biochemical tests have been reported in patients with intrathoracic hydatid cyst, there may be nonspecific leukopenia or thrombocytopenia, mild eosinophilia, is only present in 15%, or alterations in liver function tests, which are not conclusive. The patient of the case that we present did not have any alteration in the paraclinical tests, in addition to the other case reports where hardly any of the patients showed alterations in the studies, which reinforces the current that it is not necessary that there be eosinophilia to consider the diagnosis of a parasitosis.
The serological diagnosis of Echinococcus granulosus combines at least 3 methods, initially indirect hemagglutination or ELISA, and to confirm immunoelectrophoresis or by Western Blot), the serum determination of specific IgE that occurs only in case of serological dissociation. In the absence of a positive serological test, aspiration of the cyst content may be required for histopathological identification of hydatid elements (hooks, or membranes). In the case presented, the serology determination was not carried out because the diagnosis was obtained by direct visualization of elements of E. granulosos with histopathology.
The importance of early diagnosis of an intrathoracic hydatid cyst in the pleural cavity is that, although the majority of cases present with respiratory clinical data that may not affect quality of life, they can also manifest as a result of rupture of cyst with pneumothorax, pleural effusion, empyema and allergic or anaphylactic reaction, which requires immediate and accurate therapeutic intervention.
Hydatid cyst management options include medical treatment, percutaneous puncture, surgical resection, or observation. The curative goal is achieved with surgical resection; the technique of choice is cystectomy and capitonage that may require adjuvant therapy with protocolicidal agents such as albendazole and close follow-up to detect recurrences early [36]. The recurrence rate has been estimated to be 0–2.7% [37], and overall morbidity and mortality rates after surgical treatment of pulmonary hydatid cyst are 1.4%–19.1% and 0.6%–4.2%, respectively [38].
Patients at high surgical risk or who do not agree to undergo an intervention, should receive long-term therapy with albendazole. When the cyst has ruptured within the pleural cavity, drainage and a thoracotomy are necessary to eliminate all traces of hydatid disease and prevent or treat anaphylaxis, which is a latent risk, as well as seeding in other intra- or extra-thoracic locations. In general, treatment can be chosen based on the type of hydatid cyst and its characteristics according to the WHO ultrasonographic classification. The recommended dose of albendazole is 10 to 15 mg/kg per day divided into 2 doses, or 400 mg 2 times a day in adults, the duration of treatment is variable; for one month after surgical resection, and the duration for those patients who cannot undergo surgery is 10 to 15 mg/kg/day for 4 weeks, at least three cycles separated by 2 weeks [39]. This work has been reported in line with the SCARE criteria [40].
In conclusion, this article exemplifies the importance of considering primary pleural hydatidosis in young patients, especially from endemic countries, within a differential diagnosis of thoracic cystic lesions, in order to offer adequate treatment and follow-up based on the characteristics of the cyst.
The additional file for this article can be found as follows:
Supplemental MaterialSCARE 2020 Checklist. DOI: https://doi.org/10.29337/amscr.3.s1
Ethical approval has been waived by the institution, as it is not considered risky research for the patient or researchers.
Informed consent was obtained from the patient for the publication of this case report. A copy of the written consent is available for review by the editor-in-chief of this journal upon request.
“Currently, I’m satisfied with my treatment, I hope to continue improving as I have been doing it so far.”
The authors have no competing interests to declare.
Medina-Franco Heriberto.
This is a non-commissioned paper that has undergone external peer review according to journal policy.
Kalra S, Gogia P, Rakheja N. Primary pleuropulmonary echinococcosis – Varied manifestations. J Curr Med Res Pract. 2018; 8(3): 109–112. DOI: https://doi.org/10.1016/j.cmrp.2018.04.003
Qian ZX. Thoracic hydatid cysts: a report of 842 cases treated over a thirty-year period. Ann Thorac Surg. 1988; 46(3): 342–346. DOI: https://doi.org/10.1016/S0003-4975(10)65941-3
McManus DP, Zhang W, Li J, Bartley PB. Echinococcosis. Lancet. 2003; 362(9392): 1295–1304. DOI: https://doi.org/10.1016/S0140-6736(03)14573-4
Oğuzkaya F, Akçali Y, Kahraman C, Emiroğullari N, Bilgin M, Sahin A. Unusually located hydatid cysts: intrathoracic but extrapulmonary. Ann Thorac Surg. 1997; 64(2): 334–337. DOI: https://doi.org/10.1016/S0003-4975(97)00521-3
Ulkü R, Eren N, Cakir O, Balci A, Onat S. Extrapulmonary intrathoracic hydatid cysts. Can J Surg. 2004; 47(2): 95–98.
Jesiotr M, Romanoff H. Pneumothorax following rupture of a primary pleural hydatid cyst. A case report. J Thorac Cardiovasc Surg. 1972; 63(4): 594–598. DOI: https://doi.org/10.1016/S0022-5223(19)41875-8
Emlik D, Kiresi D, Sunam GS, Kivrak AS, Ceran S, Odev K. Intrathoracic extrapulmonary hydatid disease: radiologic manifestations. Can Assoc Radiol J. 2010; 61(3): 170–176. DOI: https://doi.org/10.1016/j.carj.2009.12.002
Oğuzkaya F, Akçali Y, Kahraman C, Emiroğullari N, Bilgin M, Sahin A. Unusually located hydatid cysts: intrathoracic but extrapulmonary. Ann Thorac Surg. 1997; 64(2): 334–337. DOI: https://doi.org/10.1016/S0003-4975(97)00521-3
Jana P, Daekincis I, Bairagya T, Dhali S, Mitra S, Kundu S, Dutta S. Pleural Hydatid Cyst Causing Pyopneumothorax, an Unusual Presentation. Int Med J. 2012; 19: 309–311.
Canpolat U, Sunman H, Taher A, Yorgun H, Dural M, Tokgozoglu L, et al. Fissural hydatid cyst in a young woman mimicking phantom tumor. Int. J. Cardiol. 2010; 140: S61. DOI: https://doi.org/10.1016/S0167-5273(10)70211-4
Kumar A, Yadav P, Pahuja S, Chaudhri S. Hydatid Disease of Pleura: A Rare Cause of Recurrent Pneumothorax. Case Report JCR. 2016; 6(2): 273–276. DOI: https://doi.org/10.17659/01.2016.0067
Rakower J, Milwidsk H. Hydatid pleural disease. Am Rev Respir Dis. 1964; 90: 623–31.
Harzallah L, Bacha M, Garrouche A, et al. Kyste hydatique pleural primitif: a propos d’une observation [Primitive pleural hydatid cyst: case report]. Rev Med Liege. 2007; 62(7–8): 506–508.
Kim S, Jung K, Jo W, Kim Y, Shin C, Kim J. A Case of Pleural Hydatid Cyst Mimicking Malignancy in a Non-Endemic Country. Tuberc Respir Dis. 2011; 70: 338–341. DOI: https://doi.org/10.4046/trd.2011.70.4.338
Darwish B. Clinical and radiological manifestations of 206 patients with pulmonary hydatidosis over a ten-year period. Prim Care Respir J. 2006; 15(4): 246–251. DOI: https://doi.org/10.1016/j.pcrj.2006.05.006
Hashmi M, Ullah M, Sarwar M, Sultan A, Aleem A, Khan I. Extrapulmonary Intrapleural Hydatid Disease- A Case Report. MedPharmRes. 2019; 3(1): 12–16. DOI: https://doi.org/10.32895/UMP.MPR.3.1.12
Oncel M, Yildiran H, Sunam GS. What Is Floating in the Pleural Space? Ann Thorac Surg. 2018; 106(5): e263. DOI: https://doi.org/10.1016/j.athoracsur.2018.04.020
Mrabet FZ, Achrane J, Sabri Y, El Hassani FE, Hammi S, Bourkadi JE. Contribution of Imaging in Diagnosis of Primitive Cyst Hydatid in Unusual Localization: Pleura-A Report of Two Cases. Case Rep Radiol. 2018; 2018: 6242379. DOI: https://doi.org/10.1155/2018/6242379
Amini S, Kahramfar Z, Rahimi B. A case of Extrapulmonary intrathoracic hydatidosis with pseudochylothorax. Clin Case Rep. 2018; 6: 1507–1509. Published 2018 Jun 19. DOI: https://doi.org/10.1002/ccr3.1628
Mardani P, Karami MY, Jamshidi K, Zadebagheri N, Niakan H. A Primary Pleural Hydatid Cyst in an Unusual Location. Tanaffos. 2017; 16(2): 166–169.
Badji NF, NDong B, Akpo G, Dème H, Touré MH, Niang El H. Apport De L’Imagerie Dans Le Diagnostic De Kyste Hydatique Pleural Primitif: à Propos De Deux Cas [Contribution Of Imaging In Diagnosis Of Pleural Cyst Hydatid Primitive: Two Cases Reports]. Mali Med. 2017; 32(4): 33–36.
Alakhras F. A rare case of primary hydatidosis; a primary parietal pleural hydatid cyst. Acta Healthmedica. 2016; 1(4): 93–97. DOI: https://doi.org/10.19082/ah93
Akkas Y, Kaplan T, Peri NG, Kocer B. Do the Hydatid Cysts Have Unusual Localization and Dissemination Ways in the Chest Cavity? Case Rep Surg. 2016; 2016: 7092494. DOI: https://doi.org/10.1155/2016/7092494
Erkoç MF, Öztoprak B, Alkan S, Okur A. A rare cause of pleural effusion: ruptured primary pleural hydatid cyst. BMJ Case Rep. 2014; 2014: bcr2013202959. DOI: https://doi.org/10.1136/bcr-2013-202959
Ekinci G, Haciomeroglu O, Ongel E, Kavas M, Yilmaz A. Primary Pleural Hydatid Disease. Respir Case Rep. 2013; 2(3): 147–149. DOI: https://doi.org/10.5505/respircase.2013.70288
Vaideeswar P, Agnihotri MA, Hira P. Unusual manifestations of pleuro-pulmonary hydatidosis. Indian J Pathol Microbiol. 2012; 55: 111–112. DOI: https://doi.org/10.4103/0377-4929.94878
Singh J, Rana SS, Singh H, Sharma R, Sharma V. Multiple intrathoracic hydatids. Asian Cardiovasc Thorac Ann. 2010; 18: 88–9. DOI: https://doi.org/10.1177/0218492309355197
Tewari M, Kumar V, Shukla HS. Primary pleural hydatid cyst. Indian J Surg. 2009; 71(2): 106. DOI: https://doi.org/10.1007/s12262-009-0029-0
Mbatchou N, Badiane N, Diarra O, Kane Y, Diatta A, Sah A, et al. Pneumothorax compressif compliquant: Une hydatidose pleurale. Rev. Pneumol. Trop. 2004; 1: 5–6.
Antona Gómez JM, García-Vinuesa G, Fuentes Otero F, Checa Pinilla JM, Pérez Miranda M. Giant primitive pleural hydatid cyst. Chest. 1979; 76(5): 614. DOI: https://doi.org/10.1378/chest.76.5.614
WHO Informal Working Group. International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop. 2003; 85: 253. DOI: https://doi.org/10.1016/S0001-706X(02)00223-1
Gharbi HA, Hassine W, Brauner MW, Dupuch K. Ultrasound examination of the hydatic liver. Radiology. 1981; 139: 459. DOI: https://doi.org/10.1148/radiology.139.2.7220891
Sebit S, Tunc H, Gorur R, Isitmangil T, Yildizhan A, US MH, Pocan S, Balkanli K, Ozturk OY. The evaluation of 13 patients with intrathoracic extrapulmonary hydatidosis. J Int Med Res. 2005; 33: 215–221. DOI: https://doi.org/10.1177/147323000503300209
Zarzosa MP, Orduña Domingo A, Gutiérrez P, et al. Evaluation of six serological tests in diagnosis and postoperative control of pulmonary hydatid disease patients. Diagn Microbiol Infect Dis. 1999; 35: 255. DOI: https://doi.org/10.1016/S0732-8893(99)00079-6
Ortona E, Riganò R, Buttari B, et al. An update on immunodiagnosis of cystic echinococcosis. Acta Trop. 2003; 85: 165. DOI: https://doi.org/10.1016/S0001-706X(02)00225-5
Halezeroglu S, Okur E, Tanyü MO. Surgical management for hydatid disease. Thorac Surg Clin. 2012; 22(3): 375–385. DOI: https://doi.org/10.1016/j.thorsurg.2012.04.004
Pejhan S, Zadeh M, Javaherzadeh M, et al. Surgical Treatment of Complicated Pulmonary Hydatid Cyst. Tanaffos. 2007; 6(1): 19–22.
Sahin E, Enon S, Cangir AK, Kutlay H, Akay H, et al. Single-stage transthoracic approach for right lung and liver hydatid disease. J Thorac Cardiovasc Surg. 2003; 126: 769–73. DOI: https://doi.org/10.1016/S0022-5223(03)00366-0
Brunetti E, Kern P, Vuitton DA, Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010; 114(1): 1. DOI: https://doi.org/10.1016/j.actatropica.2009.11.001
Agha RA, Franchi T, Sohrabi C, Mathew G, for the SCARE Group. The SCARE 2020 Guideline: Updating Consensus Surgical CAse REport (SCARE) Guidelines. International Journal of Surgery. 2020; 84: 226–230.