|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 2 | Page : 43-48 |
|
Prevalence of malaria and typhoid coinfection among patients in some hospitals in Samaru, Zaria
Christian E Mbah, Blessing Agu
Department of Biological Sciences, Ahmadu Bello University, Zaria, Nigeria
| Date of Web Publication | 23-Mar-2015 |
Correspondence Address:
Christian E Mbah
Department of Biological Sciences, Ahmadu Bello University, Zaria
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.153813

Background: A large number of staff and students live off-campus (cannot be accommodated on campus) because of limited space. Most of them live in houses where there are no clean, safe drinking water and poor or no drainage system. The investigation was carried out by screening blood samples of patients who attended the Ahmadu Bello University Clinic (Sickbay) and Jama'a hospital in Samaru, Zaria to determine the occurrence of malaria and typhoid parasites in the area. Materials and Methods: Blood samples were collected with new disposable syringes from 264 patients during the period of study of 3 months. Blood films were stained with Giemsa stain, air- dried, treated with immersion oil, and examined under high-power objective of the microscope. Malaria parasites were identified based on their ring forms. The Widal test was used to detect the presence of Salmonella antibodies in the patient's serum. Result: Majority of the people screened 143 (84.1%) adults were not infected while 27 (15.9%) had malaria parasites in their blood stream. Only 20 (21.3%) of the children screened were positive for malaria parasites. Two Plasmodium parasites, Plasmodium falciparum and P. vivax were detected in the blood samples. Plasmodium falciparum was found to be significantly higher than P. vivax. More adults from age 19 and older had typhoid pathogens (57.0%) in their blood samples than children who were 18 years and younger (21.2%). A small but significant proportion (15.2%) of those screened were co-infected with malaria and typhoid. Conclusion: Malaria and typhoid are diseases of poverty that are still endemic in developing countries. It requires the combined effort of the government at all levels, the scientific community and co-operation of every member of the society to conquer these re-emerging diseases. Keywords: Coinfection, malaria, typhoid, Zaria
How to cite this article:
Mbah CE, Agu B. Prevalence of malaria and typhoid coinfection among patients in some hospitals in Samaru, Zaria. Ann Bioanthropol 2014;2:43-8 |
| Introduction | |  |
The first historical evidence of malaria parasites was found in mosquitoes preserved in amber from the Palaeogene period about 30 million years ago. [1] Human malaria is believed to have originated from Africa and coevolved with its hosts, mosquitoes and non-primates. [2] Human beings probably first became infected by mosquitoes which fed on gorillas and transmitted Plasmodium falciparum with their bites. [3] Plasmodium vivax may have been transmitted from chimpanzees and gorillas. [4] Plasmodium knowlesi has its origin in Asian macaque monkeys while Plasmodium malariae is highly specific to humans with some evidence of asymptomatic infection among wild chimpanzees. [5]
Malaria parasites are transmitted by the bites of an infected female Anopheles mosquito. The African continent is the most severely affected by malaria. For this reason, April 25 th of every year has been declared African Malaria Day and the Roll Back Malaria (RBM) campaign has Africa as its main focus. [6]
The Anopheles gambiae species A of the An. gambiae complex is widespread in nearly all African countries south of the Sahara and it is probably the world's most efficient malaria vector. [7] It consists of morphologically similar species separated by banding patterns of their polytene chromosomes and certain aspects of their biology and behavior. They include: An. arabiensis, An. quadriannulatus, An. melas, An. merus, An. funestus, An. nilli, An. mucheti, An. hargreavesi, and An. Hanocki. [8]
Typhoid is a common worldwide bacterial disease, transmitted by the ingestion of food or water contaminated with the feces of an infected person, which contains the bacterium Salmonella typhi enteric serovar. The pathogen is a Gram-negative short bacillus that is motile due to its peritrichous flagella. [9]
There are about 33 million cases of typhoid annually resulting in 216,000 deaths in endemic areas. The World Health Organization (WHO) identifies typhoid as a serious public health problem with high incidence on children and young adults. [9] Typhoid fever also has a very high social and economic impact because of the hospitalization of patients with acute disease and the complications and loss of income during the duration of the clinical illness. [10]
In April 2000, the government of Nigeria hosted the African Summit on RBM in Abuja, demonstrating political commitment at higher levels. In African countries, there has been an increase in NGO (non-governmental organization), private sector, and non-health sector involvement (e.g., collaboration with Ministries of Education, Communication, Finance, Agriculture, Environment) and non-traditional partners have become involved, e.g., UNESCO in Sudan. Joint actions on malaria between neighboring countries have also taken shape, e.g., the health for peace initiative in West Africa. [11]
The Global Malaria Action Plan (GLAP) with guidelines of its implementation was laid down in 1993-2000. The basic technical elements of the strategy is to provide early diagnosis and prompt treatment, plan and implement selective and sustainable preventive measures including vector control, to detect an early stage or epidemic, to strengthen local capacities. [12]
Typhoid is spread by the fecal-oral route and closely associated with poor hygiene; lack of clean, safe drinking water; and poor sanitation. The disease is exclusively transmitted through food and water contaminated by the urine and feces of patients and carriers. Polluted water is the most common source of typhoid transmission. In addition, shellfish taken from sewage contaminated beds, unwashed vegetables fertilized with night-soil and eaten raw, contaminated milk and milk products have been shown to be a ready source of infection. [9]
Taxonomy within the genus Salmonella has been receiving attention. Recent classification based on DNA sequencing has left only two species, S. enteric and S. bongori, further subdivided into subspecies and serovars. Salmonella enterica serovar Typhi continues to be referred to as S. typhi.
The study was carried out in Ahmadu Bello University, Main Campus, Zaria and Samaru Village located opposite the Main Campus. The University Campus is well-planned with layouts of academic areas, student hostels and staff quarters; the contrary is the case in Samaru Village where houses were built indiscriminately with utter disregard to town planning regulations and most areas are without access roads and basic amenities, such as clean and safe drinking water and observance of environmental sanitation.
The university cannot provide accommodation for all of its students and staff. The majority of the students, staff and their families live off campus in Samaru Village. Among the patients (staff and students) who attend the university clinic, their major complaints are usually connected with typhoid fever and malaria. This is what prompted this investigation to unravel the probable causes of these problems and proffer lasting solutions.
| Materials and methods | | |
Blood samples were collected with new disposable syringe from 264 patients who attended Ahmadu Bello University Health Center and Jama'a Hospital during the period of study of 3 months.
Blood films were made by using the end of a pipette to apply a large drop of blood on the slide to produce a thick smear. An area of about 15 mm × 15 mm was covered by the film. The blood films were air-dried and the slide placed on a horizontal position. [13]
Giemsa stain, buffered water or saline of pH 7.1-7.2 was used for staining. Giemsa stain was diluted with 10% solution for 10 min staining. The slides were placed face downwards on a slide rack. Immersion oil was added by the edge and it spread to cover an area of about that is equivalent to the diameter of the film. Blood films were examined under ×40 and ×100 objectives and malaria parasites recorded. The parasites were identified based on their ring forms.
Widal test
The Widal test is a serological technique used to detect the presence of Salmonella antibodies in the patient's serum. [13] Serum was obtained from 5 ml of the patient's venous blood. [14] One drop of positive control was placed on a reaction circle of a glass slide. A 50 μl of physiological saline was placed on the next reaction circle of the glass slide. One drop of the patient's serum was placed to be tested on each of the reaction circles. A drop of the appropriate Widal antigen suspension was added to the reaction circles containing positive control and physiological saline. One drop of appropriate widal antigen suspension was also added to the reaction circles containing the patient's serum. The content of each circle is uniformly mixed over the entire circle with separate mixing sticks. The slides were gently rocked back and forth, and observed for agglutination for one minute. Agglutination is a positive test result which indicates the presence of the corresponding antibody in the patient's serum. [14]
| Result | | |
A total of 264 blood samples was collected from Sickbay and Jama'a Hospital in Samaru, Zaria and analyzed. Four parameters were used to compare the occurrence of malaria and typhoid: age, sex, Plasmodium species, and Salmonella typhi type.
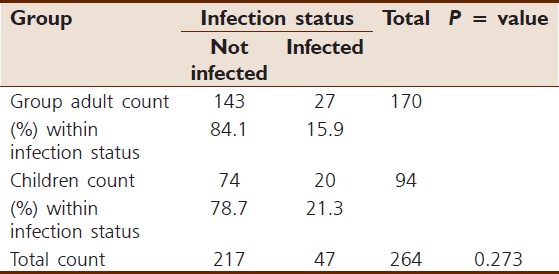
The majority of the people screened, 143 (84.1%) adults, were not infected while 27 (15.9%) had malaria parasites in their bloodstream. Twenty (21.3%) children screened were positive for malaria parasites [Table 1]. There was no significant association between infection status and age.
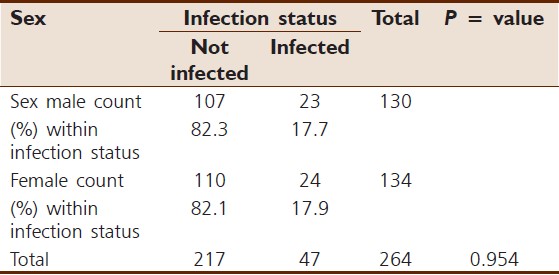
The number of males infected with malaria parasites, 23 (17.7%), was slightly lower than the number of infected females, 26 (17.9%) [Table 2]. Association between malaria infection and sex was therefore not significantly different.
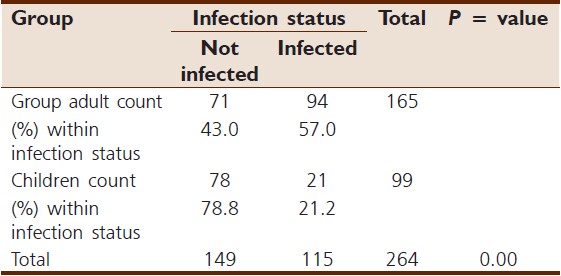
Two Plasmodium parasites, plasmodium falciparum and plasmodium vivax were detected in the blood samples. Plasmodium falciparum was found to be significantly higher than P. vivax in the samples [Table 3]. More adults aged 19 years and older had typhoid pathogens (57.0%) in their blood samples than children ages 18 years and younger (21.2%). The proportion of infected adults was significantly higher than children with typhoid [Table 4].
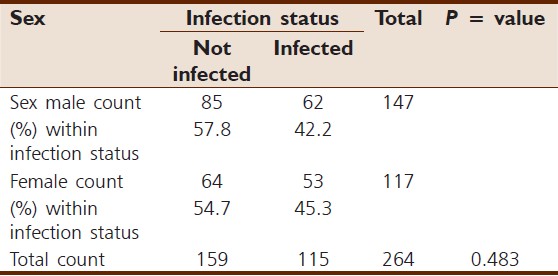
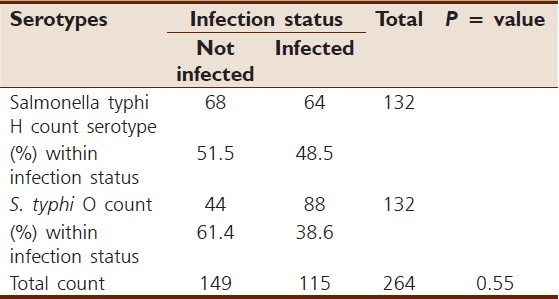
Females had slightly higher prevalence of S. typhi (45.3%) than males (42.2%) [Table 5]. Association between S. typhi infection and sex did not differ significantly. The prevalence of Salmonella typhi infection was slightly higher (48.5%) with H antigen than the infections for O antigen (38.6%) [Table 6]. The association with Salmonella typhi H antigen was not significant. It was discovered that out of the 264 blood samples screened, 47 (17.8%) patients were infected with malaria parasites, 115 (43.7%) patients with typhoid, while 40 (15.2%) were infected with malaria and typhoid at the same time. Parasites of malaria and typhoid were not detected from the remaining 62 patients representing 23.5% of all those screened [Table 7].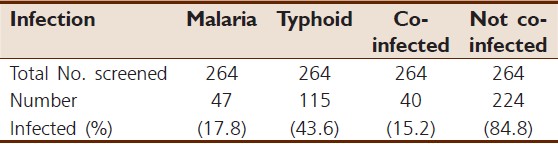 | Table 7: Prevalence of infected, co-infected and not co-infected patients
Click here to view |
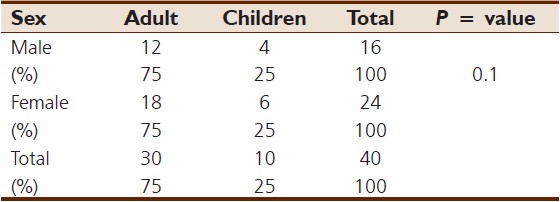
Of those who were coinfected, 30 (75%) were adults, while 10 (25%) were children. More females 24 (60%) were coinfected with malaria and typhoid than males 16 (40%) [Table 8].
| Discussion | | |
The vast majority of estimated cases (80%) and deaths (91%) caused by malaria occur in sub-Saharan Africa and most of them are in children under five years of age. Patients suffering from malaria represent about 60% of clinic visits annually. [15]
One out of every 6 adults screened were predisposed to malaria infection compared to one out every 5 children screened. This is probably because children require repeated infections before they could develop resistance, while adults must have developed resistance before reaching their present age. The majority of malaria cases occur in children and pregnant women who are also known to be vulnerable. Children who suffer first and second bouts of malaria are believed not to have developed appropriate immunity against the parasite. This is probably responsible for more malaria cases observed in children. [15]
Both male and female patients were equally predisposed to malaria infection because any part of the body that is exposed to mosquito bite is an avenue for parasite innoculation and transmission irrespective of gender.
The major malaria parasite incriminated in this study was Plasmodium falciparum. It is the main species found in hotter parts of the world including tropical Africa, part of South America, Bangladesh, Nepal, India, the Middle East, and the eastern Mediterranean. This pathogen has wider distribution in tropical and sub-tropical regions of the world including Nigeria. Plasmodium vivax develops in mosquitoes at lower temperatures. Although it is found in tropical countries P. vivax is the main pathogen in South America occurring as far as south of northern Argentina, Mexico, and the Middle East. It is possible that the pool of P. vivax in tropical countries of the world is maintained by a stream of travellers who import them from temperate regions where they are endemic. [5],[12]
Several people opt for self-medication when they suspect that they are suffering from malaria. Some use herbs and concoctions, which they believe cure malaria. However, the high cost of drugs and medical treatment also limits its accessibility. Malaria is strongly associated with poverty. [15]
The drug of choice endorsed by the WHO for children and adults is Coartem, artemether 20 mg/lumefantrine 120 mg. It is an antimalarial agent manufactured by Novartis Pharmaceutics Corporation, Suffern, New York, USA. Another recommended drug similar to Coartem is Gvitherplus, artemether 80 mg/lumefantrine 480 mg. It is used for treatment of malaria including multidrug resistant strains of P. falciparum. It is manufactured by Bliss Pharma Ltd. Maharashtra, India with NAFDAC No. A4-6730. Artemisnin derivatives like artemether are the fastest-acting schizonticides, which clears the parasites rapidly.
Prevention of malaria can be accomplished by use of insecticide treated bednets, administration of prophylactic drugs through a licensed medical practitioner, and mosquito eradication. The plan to produce vaccines that will destroy all stages of the parasite and possible mutations is still a thing of the future. Research towards replacement of current population of mosquitoes with genetically engineered population has produced the first Plasmodium resistant species announced by a team of researchers at Case Western Reserve University in Ohio in 2002. [15] A researcher from Liverpool, School of Tropical Medicine Gareth Lyceth, told BBC that "it is another step on the journey towards malaria control through genetically-modified mosquito release." [15] In addition, the Biology and Control of Vectors (BCV) group has sponsored groundbreaking research into the genetic manipulation of Anopheles gambiae. There is ongoing global genomics research effort to create a transgenic mosquito. This will open up the prospect of modifying mosquitoes so that they become unable to transmit malaria parasites. [16]
Some symptoms of malaria such as fever, headache, and shivering are similar to that of typhoid. More adults were infected with Salmonella typhi than children probably because of occupational hazards such as eating food or raw vegetables in the farms without proper washing, eating, and drinking satchet water of questionable hygienic quality especially on a journey could expose them to infection. Children who contract typhoid may still be learning about hygiene, or even lack basic amenities such as clean, safe drinking water.
Typhoid infection did not exhibit preference for either of the sexes, likely because patients who were screened live and work in the same environment and obtained their food and water basically from the same source.
Although typhoid fever has practically disappeared from industrialized countries [17],[18] it remains a serious public health problem in several Asian, African and South American regions of the world.
The rediscovery of Oral Rehydration Therapy (ORT) provided a simple way to prevent many of the deaths of diarrheal diseases including typhoid. Where resistance is uncommon, the treatment of choice is a fluoroquinolone such as ciprofloxacin, otherwise, a third generation cephalosporin such as ceftriaxone or cefataxime is preferred. Cefixime is a suitable oral alternative.
Typhoid in most cases is not fatal. Antibiotics such as ampicillin, chloroamphenicol, trimethoprin - sulfamethoxazole, amoxicillin, and ciprofloxacin have been commonly used to treat typhoid in developed countries. [9]
The fact that more individuals were infected with typhoid than malaria indicates a poor level of personal and general hygiene among the patients screened within the communities where they reside.
A small but significant proportion (15.2%) of those screened were coinfected with malaria and typhoid. Where such people embark on self-treatment without proper laboratory tests and Doctor's prescription, malaria is usually treated while typhoid is masked. The danger is that they are healthy carriers like Mary Mallon, known as "Typhoid Mary," who was the first known case of a healthy carrier in the United States. [19] She was incriminated in the contamination of at least 120, including five dead. [19] By the time it would be realized that there was coinfection the victims' intestines would have been perforated leading to complications and avoidable deaths.
When untreated, typhoid fever persists for 3-4 weeks and death occurs in some 10 to 30% of such cases. [9]
Two vaccines have been licensed for use for the prevention of typhoid: The live, oral Ty21 a vaccine marketed as Vivotif Berna and the injectable typhoid polysaccharide vaccine sold as Typhim Vi by Sanofi Pasteur and Typherix by GlaxoSmithKline. They are protective and are recommended for travelers to areas where typhoid is endemic.
The introduction of typhoid vaccines in routine vaccination programs will greatly reduce the disease burden and cost of illness to governments and individuals. Only China and Vietnam have incorporated typhoid vaccination into their immunization programs. [15],[16],[17]
| Conclusion | | |
Malaria and typhoid have been vanquished from developed countries, but they remain a life-threatening health problem in Africa and other developing third-world nations. Only combined effort by individuals, governments, and NGOs through the provision of basic social amenities can turn the tide in favor of millions who are effected. Malaria and typhoid infections cut across all strata of the society, irrespective of sex and age. Control strategies should be tailored to cater for all segments of the community including unborn babies who in some cases are unwilling victims.
Recommendations
Distribution of insecticide treated nets should cover every hamlet, free of charge, under the RBM Program. Applied research into drugs for the treatment of resistant malaria and typhoid pathogens should be intensified while all hands must be on deck to teach children the rudiments of personal hygiene and everyone should imbibe the good habit of washing hands before and after eating with clean water.
| References | | |
| 1. | Poinar, G Jr. Plasmodium dominicana n. sp. (Plasmodidae: Hamospororida) from tertiary Dominican amber. Syst Parasitol 2005;61:47-52.  |
| 2. | Joy, DA, Feng X, Mu J, Furuya T, Chotivanich K, Krettli AU, et al. Early origin and recent expansion of Plasmodium falciparum. Science 2003;300:318-21. |
| 3. | Liu W, Li Y, Learn GH, Rudicell RS, Robertson JD, Keele BF, et al. Origin of the human malaria parasite Plaasmodium falciparum in gorillas. Nature 2010;467:420-5. |
| 4. | Liu W, Li Y, Shaw KS, Learn GH, Plenderleith LJ, Malenke JA, et al. African origin of the malaria parasite Plasmodium vivax. Nat Commun 2014;5:3346. |
| 5. | Lee KS, Divis PC, Zakaria SK, Matusop A, Julin RA, Conway DJ, et al. Plasmodium knowlesi: Reservoir hosts and tracking the emergence in humans and macaques. PLoS Pathog 2011;7:e1002015. |
| 6. | Ridley R, Mocumbi P. Combating Malaria. World Malaria Day - 25 th April: Research in Developing Countries Must be Supported. TDR News No. 83. Geneva, Switzerland. World Health Organization; 2009. p. 18. |
| 7. | Service MW. A Guide to Medical Entomology. London: The Macmillan Press Ltd.; 1980. p. 3-47. |
| 8. | Lane RP, Crosskey RW. Medical Insects and Arachnids. British Museum (Natural History). London: Chapman and Hall; 1995. p. 120-240. |
| 9. | Anonymous. Background Document: The Diagnosis, Treatment and Prevention of Typhoid Fever. Communicable Disease Surveillance and Response. Vaccines and Biologicals. Geneva, Switzerland. World Health Organisation, WHO/V&B/03.07; 2003. p. 7-26. |
| 10. | Punjabi NH. Cost evaluation of typhoid fever in Indonesia. Med J Ind 1998;7(Suppl 5-6):90-3. |
| 11. | Anonymous. Reducing infant deaths due to malaria. TDR News No. 77, p.12, February 2007. Special Programme for Research and Training in Tropical Diseases sponsored by UNICEF/UNDP/WORLD BANK/WHO. Geneva, Switzerland. World Health Organization 2007; p. 12. |
| 12. | Mbah CE, Yashim YE, Iliyasu IM. A Survey of adult mosquito species found in selected mosques in Samaru Zaria. J Ed Res Dev 2012;7:45-51. |
| 13. | Cheesbrough M. District Laboratory Practice in Tropical Countries. Cambridge low price edition. Part 1 and 2, Tropical Health Technology. St. Albans, Herts, United Kingdom. For Cheesbrough 2000: Cambridge; 2000. p. 176-253. |
| 14. | Cruickshank R. Medical Microbiology. 12 th ed. Churchill Livingstone 1975. 587 pages. Michigan. For Cruickshank R. 1975: Lab-Care Diagnostics Pvt. Ltd.; 1982. p. 403. |
| 15. | Anonymous. World Health Organization Global Malaria Report. Geneva: WHO; 2012. |
| 16. | Anonymous. Mosquito genomes secrets. TDR News No. 79. Geneva, Switzerland. World Health Organization; 2007. p. 28-9. |
| 17. | Anonymous. New vaccine development: Establishing priorities. Vol. 11. Diseases of Importance in Developing Countries, Appendix D14. Washington DC: National Academy Press; 1986. p. 1-10. |
| 18. | Ivanoff BN, Levine MM, Lambert PH. Vaccination against typhoid fever: Present status. Bull World Health Organ 1994;72:957-71. |
| 19. | Soper GA. The curious career of typhoid mary. Bull N Y Acad Med 1939;15:698-712. |
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7], [Table 8]
|








 Search Pubmed for
Search Pubmed for