|
 
 |
| CASE REPORT |
|
| Year : 2017 | Volume
: 5
| Issue : 1 | Page : 40-42 |
|
Anomalous renal vasculature
Chike Ikechukwu Patrick Anibeze, Christian Chiemeka Ozor, Ogugua Augustine Egwu, Jude Ikechukwu Nnaji, Bright Ozuroke Enyinda, Blessing Amara Iwunze
Department of Anatomy, Faculty of Basic Medical Sciences, College of Medicine, Enugu State University of Science and Technology, Parklane, GRA, Enugu, Nigeria
| Date of Web Publication | 11-Jul-2017 |
Correspondence Address:
Christian Chiemeka Ozor
Department of Anatomy, Faculty of Basic Medical Sciences, College of Medicine, Enugu State University of Science and Technology, Parklane, GRA, Enugu
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.210255

Presence of anomalous structures has been continually observed in human body specimens. Such variations have been observed in renal vasculature. During routine dissection of a young adult male cadaver at the Dissection Hall of the Anatomy Department of Enugu State University of Science and Technology, College of Medicine, Parklane, GRA, Enugu, Nigeria, we found multiple renal vasculatures. There were four separate renal arteries arising directly from abdominal aorta on the left. On the right, one major artery gives an early branch and three branches close to the hilum before separately entering the renal parenchyma. The venous vasculature also displays an obvious variation of a bifurcated vein on the right and a normal single vein on the left. These may predispose to easy factors of partial occlusion or compression of renal vasculature resulting in varicocele or hypertension. Similarly, blood circulation through the renal arteries, in case of multiple branching pattern, may result in altered hemodynamics. The knowledge of these anomalous vasculatures is significant since it is known that microvascular techniques for renal transplantation surgeries require a thorough anatomical knowledge of accessory or multiple vasculatures for better outcomes. Keywords: Anomalies, cadaver, kidney, renal artery, renal vein
How to cite this article:
Anibeze CI, Ozor CC, Egwu OA, Nnaji JI, Enyinda BO, Iwunze BA. Anomalous renal vasculature. Ann Bioanthropol 2017;5:40-2 |
| Introduction | |  |
The anomalies in structure of the human body have been noted by many radiologists and surgeons, and these have often served as useful tools and aids both in the study of human anatomy and clinical practice. Many of such occurrences in the different structures of the human body have been reported over the years.[1] The awareness of these anomalies has been helpful in providing answers to some complications observed in clinical practice and applied anatomy. The renal arteries on each side normally arise from the abdominal aorta below the origin of the superior mesenteric artery.[2] Near the hilum of the kidney, each renal artery divides into anterior and posterior branches, which in turn divides into a number of segmental arteries supplying the different renal vascular segments. The presence of anomalous branching pattern of the renal artery is not uncommon, and in 70% of the cases, there is a single renal artery supplying each kidney.[3] The renal veins normally show bilateral variations in the pattern of venous return to the inferior vena cava (IVC). In the present study, we report anomalous patterns of renal vasculature in a young adult male cadaver. The uniqueness of this case report is the multiplicity of the renal arteries and veins in one specimen.
| Case Report | | |
During the routine dissection by a team of undergraduate medical students, with postgraduate supervisions, in the Anatomy Department of Enugu State University of Science and Technology, College of Medicine, we observed some anomalous variations in the renal vasculature of an embalmed male cadaver. Based on the mode of cadaver procurement, it was impossible to put the exact age. However, visual observations on the gross anatomy suggest the age of the cadaver to be between 20 and 30 years. The anomalous situations were studied in detail and the specimens were photographed. We noticed variations in the number of renal arteries bilaterally, but that of the renal veins on the right.
On the left, one main renal artery (MRA) and three accessory renal arteries (ARA) supply the kidney. All the four renal arteries are direct branches of the abdominal aorta. The MRA and the three ARAs enter the substance of the kidney without prior branching into segmental arteries. Of the four renal arteries, the MRA enters the hilum. The three ARAs are aberrant arteries which enter the renal parenchyma through the surface of the kidney. The first ARA (FARA) penetrates the substance of the kidney superior to the hilum having passed posterior to the left ureter. The second ARA (SARA) enters the kidney inferior but close to the hilum of the kidney, while the third ARA enters the kidney farther inferior to the hilum. The left kidney however presents only one renal vein that exits through its hilum to join the IVC.
The right kidney presents only one MRA that originates from the lateral aspect of the abdominal aorta and then trifurcates into three presegmental arteries (PSA). The first PSA is given off by the renal artery close to its origin from the abdominal aorta. The right renal artery then enters the hilum of the kidney as a terminal second PSA after given off a third PSA, which enters the kidney just inferior to the hilum. Unlike the left kidney, the right kidney drains by two renal veins ( first renal vein and second renal vein), which exit the substance of the kidney to join the IVC.
| Discussion | | |
Renal artery variations
Conventionally, each kidney is supplied by a single renal artery and drained by a single renal vein, originating from the abdominal aorta and draining into the IVC, respectively.[1] The paired renal arteries take about 20% of the cardiac output to supply the kidneys that represent <one-hundredth of the total body weight.[4] In addition to the paired renal arteries, ARAs can also exist, and a thorough knowledge of the embryological development of the kidneys and renal vessels is necessary for one to comprehend the possibilities of the existence of the multiple renal vasculatures.[2] The kidneys begin their development in the pelvic cavity and then subsequently ascend to the lumbar region. During the development and ascent of the kidneys, their blood supply shifts from common iliac artery when the organ lies in the pelvic cavity to abdominal aorta when it ascends to the lumbar region.[5] However, the kidneys may receive multiple vasculatures as accessory vessels. ARAs are found frequently – more often on the left side and occurring in as high as 30–35% of cases in some series. These arteries usually enter the upper or lower poles of the kidney.[6] The main clinical significance of such arteries entering the lower pole is that they may obstruct the ureter and lead to hydronephrosis.[6] Mir et al. suggested that ARAs are common in 20–30% of individuals, usually arising from the abdominal aorta either above or below the MRA.[5] This is typical of our specimen. On the left; the FARA took origin from the abdominal aorta superior to the origin of the MRA, while the SARA and third ARA were given off by the abdominal aorta inferior to the origin of the MRA [Figure 1]. In a study by Ozkan et al., of the total number of patients examined, the variations in renal vasculature included bilateral multiple renal arteries in 5% and early renal artery furcation in 8% of the cases.[7] In our specimen, four unilateral renal arteries were however observed on the left, with early trifurcation of the renal artery on the right, which in turn penetrate the substance of the right kidney [Figure 2] and [Figure 3]. | Figure 1: The anterior surfaces of the right and left kidneys as they lie in the paravertebral gutters. Two renal veins emerge from the hilum of the right kidney to enter the inferior vena cava. One renal vein emerges from the hilum of the left kidney and passes anterior to the abdominal aorta to enter the inferior vena cava (A: Right kidney; B: Left kidney; C: Inferior vena cava; D: Abdominal aorta; E and F: Right renal veins; G: Left renal vein; H and I: Right and left ureters, respectively)
Click here to view |
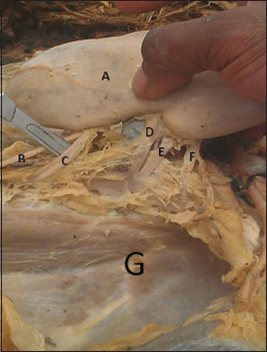 | Figure 2: The posterior surface of the left kidney as it is pulled away from the paravertebral gutter, together with the structures entering and leaving the substance of the kidney (A: Left kidney; B: Left ureter; C: First accessory renal artery; D: Main renal artery; E: Second accessory renal artery; F: Third accessory renal artery; G: Left paravertebral gutter)
Click here to view |
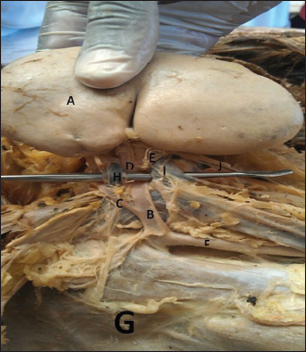 | Figure 3: The posterior surface of the right kidney as it is reflected medially away from the right paravertebral gutter together with the structures entering and exiting the substance of the kidney (A: Right kidney; B: Main renal artery; C: First presegmental artery; D: Second presegmental artery; E: Third presegmental artery; F: Abdominal aorta; G: Right paravertebral gutter; H and I: First and second renal veins, respectively; J: Right ureter)
Click here to view |
Renal vein variations
Classically, each kidney is drained by a single renal vein. However, there have been anatomic variations where more than one renal vein exit the hilum of one or both kidneys to join the IVC. The most common renal venous anomaly is the occurrence of dual renal veins, accounting for 15–30%, frequently on the right side.[8],[9],[10],[11] This is typical of the case in the index specimen of discussion. The right kidney is drained by two renal veins, which are clearly seen in [Figure 3] as they exit the hilum of the kidney. Dhar reported a case with segmental branches of right renal artery being sandwiched between two right renal veins and the emergence of two renal veins at the hilum of the right kidney, which drained separately into IVC.[12] This case had similarity with the right-sided variation of our case in which a single right renal artery is sandwiched between two right renal veins [Figure 3]. Researches have shown that in cases of dual or multiple renal veins, the smaller tributary can often be ligated without significant consequences whereas the larger vein should be preserved to maintain better venous drainage.[13] However, a close examination of both the right and left kidneys in our specimen [Figure 1] reveals that the left kidney with a single venous drainage appeared paler in color compared to the right kidney which had a dual venous drainage. Although we cannot categorically state the reasons for this discrepancy in color, we assert, tentatively, that this is indicative that the right kidney was better drained via its two renal veins than the left kidney. Anomalous veins are likely to be dilated and tortuous predisposing injury to occur during surgical dissection.[14]
| Conclusion | | |
Variations in renal vasculature occur frequently and can be masked all through life, thus allowing the individual to live a complete healthy life. However, a sound knowledge of possible variations in renal vasculature is essentially remarkable to avoid accompanying serious complications such as hydronephrosis where the ureter(s) may become obstructed by one or more of the accessory renal vessels which, in turn, are likely to be dilated and tortuous, hence predisposing to injury during surgical procedures. Hence, awareness of the presence of renal vascular variations is of extreme importance in surgical, medical, and radiological practices.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Aristotle S, Pandian S, Felicia C. Anatomical study of variations in the blood supply of kidneys. J Clin Diagn Res 2013;7:1555-7.  |
| 2. | Thakuria S, Roy RD, Baruah PD, Das TK. Multiple renal arteries: A case report. Int J Anat Var 2013;6:155-7. |
| 3. | Das S. Anomalous renal arteries and its clinical implications. Bratisl Med J 2008;109:182-4. |
| 4. | Rao TR. Aberrant renal arteries and its clinical significance: A case report. Int J Anat Var 2011;4:37-9. |
| 5. | Mir NS, Hassan AU, Rangrez R, Hamid S, Tabish SA, Rasool Z, et al. Bilateral duplication of renal vessels: Anatomical, medical and surgical perspective. Int J Health Sci 2008;2:179-85. |
| 6. | Singh G, Ng YK, Bay BH. Bilateral accessory renal arteries associated with some anomalies of the ovarian arteries: A case study. Clin Anat 1998;11:417-20. [ PUBMED] |
| 7. | Ozkan U, Oguzkurt L, Tercan F, Kizilkiliç O, Koç Z, Koca N. Renal artery origins and variations: Angiographic evaluation of 855 consecutive patients. Diagn Interv Radiol 2006;12:183-6. |
| 8. | Pozniak MA, Balison DJ, Lee FT Jr., Tambeaux RH, Uehling DT, Moon TD. CT angiography of potential renal transplant donors. Radiographics 1998;18:565-87. |
| 9. | Namasivayam S, Kalra MK, Waldrop SM, Mittal PK, Small WC. Multidetector row CT angiography of living related renal donors: Is there a need for venous phase imaging? Eur J Radiol 2006;59:442-52. [ PUBMED] |
| 10. | Holden A, Smith A, Dukes P, Pilmore H, Yasutomi M. Assessment of 100 live potential renal donors for laparoscopic nephrectomy with multi-detector row helical CT. Radiology 2005;237:973-80. [ PUBMED] |
| 11. | Smith PA, Ratner LE, Lynch FC, Corl FM, Fishman EK. Role of CT angiography in the preoperative evaluation for laparoscopic nephrectomy. Radiographics 1998;18:589-601. [ PUBMED] |
| 12. | Dhar P. An additional renal vein. Clin Anat 2002;15:64-6. [ PUBMED] |
| 13. | Disick GI, Shapiro ME, Miles RA, Munver R. Critical analysis of laparoscopic donor nephrectomy in the setting of complex renal vasculature: Initial experience and intermediate outcomes. J Endourol 2009;23:451-5. [ PUBMED] |
| 14. | Downey RS, Sicard GA, Anderson CB. Major retroperitoneal venous anomalies: Surgical considerations. Surgery 1990;107:359-65. [ PUBMED] |
[Figure 1], [Figure 2], [Figure 3]
|








 Search Pubmed for
Search Pubmed for