|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 1
| Issue : 1 | Page : 21-26 |
|
To study the prevalence of complete edentulousness among rural and urban population of Udaipur district of Rajasthan in relation to age and gender
Laxman singh kaira1, Reeta Jain2, Harpreet kukreja3, Esha Dabral4, HR Dayakara5, Vipul Asopa1
1 Department of Dentistry, Veer Chandra Singh Garhwali Medical Science and Research Institute, Srinagar Garhwal, Uttarakhand, India
2 Department of Prosthodontics, Eklavya Dental College, Jaipur, Rajasthan, India
3 Department of Prosthodontics, R. R. Dental College, Udaipur, Rajasthan, India
4 Private Practionner, Srinagar Garhwal, Uttrakhand, India
5 Department of Prosthodontics, Bapuji Dental College, Davangere, Karnataka, India
| Date of Web Publication | 16-Aug-2013 |
Correspondence Address:
Laxman singh kaira
Faculty Residence Type 2 House No. 4, Veer Chandra Singh Garhwali Medical Science and Research Institute, Srinagar, Garhwal, Uttarakhand
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.116596

Background: The objectives of this study were to evaluate the frequency of complete edentulism among rural and urban population of Udaipur district of Rajasthan who visited at a department of prosthesis at a university for the 1 st time. Materials and Methods: A cross-sectional study using the systematic cluster sampling method was used to select the study sample of 524 elderly men and women. Data were collected using questionnaires and oral examination. Data were statistically analyzed using a Chi-square test. Results: Nearly 52.3% and 47.8% of the rural and urban females were completely edentulous in the age group of 30-50 years and 51-70 years. 55.1% and 53.8% of urban and rural males were completely edentulous in 51-70 years of age groups. Conclusions: It is essential to identify feasible strategies to provide primary dental health education and treatment to all rural and urban elderly in the future. We suggest community dental health services as a general health need of the elderly rather than a special health need of the community. Keywords: Complete edentulousness, India, tooth loss
How to cite this article:
kaira Ls, Jain R, kukreja H, Dabral E, Dayakara H R, Asopa V. To study the prevalence of complete edentulousness among rural and urban population of Udaipur district of Rajasthan in relation to age and gender. Eur J Prosthodont 2013;1:21-6 |
How to cite this URL:
kaira Ls, Jain R, kukreja H, Dabral E, Dayakara H R, Asopa V. To study the prevalence of complete edentulousness among rural and urban population of Udaipur district of Rajasthan in relation to age and gender. Eur J Prosthodont [serial online] 2013 [cited 2018 Jul 12];1:21-6. Available from: http://www.eurjprosthodont.org/text.asp?2013/1/1/21/116596 |
| Introduction | |  |
Edentulousness and a small number of remaining teeth are associated with low education level and family income. [1] Edentulism is defined as the loss of all permanent teeth and is the treatment outcome of a multifactorial process involving biologic process (dental caries, periodontal disease, trauma and others), as well as non-biologic factors related to dental procedures (access to care, patient preferences). [2] The prevalence and patterns of tooth loss have been studied to a certain extent in western countries and a few such studies have been carried out in India. [1],[2],[3],[4],[5],[6],[7],[8] Dental caries and periodontitis are caused by microorganisms, but age, gender, oral hygiene and life-style (dietary habits, tobacco smoking, alcohol intake) may modify the progression of these disorders. The influence of socio-economic and the socio-demographic factors on edentulousness have been well-documented. [1],[2],[3],[4],[5],[6],[7],[8],[9]
World health organization databanks indicate that dental caries is prevalent in the majority of countries internationally with some reporting 100% incidence in their populations severe periodontal disease is estimated to affect 5-20% of the population and the incidence of complete edentulism has been estimated between 7% and 69% internationally. [1] Several cross-sectional studies on the prevalence of edentulousness show consistently that edentulousness is associated with age, gender and living areas in most countries. [1],[2],[4],[9]
Edentulism rates among the elderly have been reported as relatively high in number of European countries such as England (74-79%), Scotland (85%), Ireland (72%), Northern Ireland (69%), The Netherlands (83%), Denmark (68%), Finland (67%), and Norway (57%). In Australia, 68% of people aged 65 or more were edentulous. Edentulism is consistently shown to increase with age, with females having higher rates of edentulism than do males. [4]
We do not have the statistics of either the cause of edentulism, proportion of loss of teeth or percentage of the population of India who are completely edentulous, so this study was carried out in both rural and urban population of Udaipur district of Rajasthan.
| Aims and Objectives | | |
The present study was conducted with the following aims and objectives.
- To evaluate the percentage, duration and reasons of complete edentulousness in relation to age and gender.
| Materials and Methods | | |
The city of Udaipur is located in Rajasthan, a state in the Northern part of India. In the language of geography, Udaipur runs from latitude 24.58° in the north to longitude 73.68° in the east. The city covers an area of 37 sq.km and lies at an altitude of 598 m above sea level. It is located 403 km (250 mi) southwest of the state capital, Jaipur, 248 km (154 mi) west of Kota and 250 km (155 mi) southwest of the state capital, Jaipur, 248 km (154 mi) west of Kota and 250 km (155 mi) northwest from Ahmedabad. According to census 2011, the population of Udaipur is 3,067,549. Male population of Udaipur is 1,566,781. Female population of Udaipur is 1,500,768. Gender ratio is 958 females/1000 males. Urban population of Udaipur according to census 2011 is 608,891. District Udaipur's rural population according to census 2011 is 2,458,658. An analytical, cross-sectional, descriptive, epidemiological study to determine the prevalence of complete edentulous patients in relation to age and gender reporting to the dental colleges in Udaipur for the first time was conducted. Initially, a pilot study was carried out with 20 patients recruited in the same manner as in the main study to check the feasibility of the study and the questions were modified accordingly.
Following the successful pilot study in which the questionnaire was validated, potential subjects were approached to carry out the main study. A total of 602 completely edentulous subjects, who reported for a complete denture treatment, to the Department of Prosthodontics, Darshan Dental College and Hospital, Udaipur, were selected over a period of 1 year (September 2009 to September 2010). Subjects were selected on the basis of clinical oral examination only not by radiographic examination. Hence, a total of 78 subjects who did not complete the questionnaire and were uncooperative were excluded from the study, yielding a sample of 524 individuals Ethical clearance was obtained prior to the survey from the Ethical Committee of Darshan Dental College and Hospital. The informed consent of each patient was taken prior to recording oral health.
Subject's age was divided into following groups:
- Group I - 30-50 years
- Group II - 51-70 years
- Group III - 71 years and above.
Questionnaire proforma
A self-prepared questionnaire, which sought inquiries related to socio-demographic factors, which included name, age, sex, occupation, reasons of edentulousness (trauma, dental caries, periodontal disease, tobacco smoking, alcohol intake, diabetes, hypertension, heart failure) was prepared, but for the convenience we only included dental caries, trauma, periodontitis and other factors. Next part of the questionnaire elicited information regarding duration of edentulousness and reasons of edentulousness.
Procedure for collection of data
The questionnaire was completed personally for each patient who agreed to participate in the study, in the form of an interview, which appeared like normal conversation to allow for introduction and exploration of ideas and probe more deeply. Following the completion of the interview, the patients signed at the end of the questionnaire to mark their consent.
| Results | | |
For the present study, 524 completely edentulous subjects who reported for the first time for a complete denture treatment, to the Department of Prosthodontics, Darshan Dental College and Hospital, Udaipur, were selected over a period of 1 year.
Statistical analysis
The collected data were entered on a PC and analyzed using a standard SPSS statistical program version 11, software (SPSS Inc. Chicago ,Illinois ,USA). Descriptive statistics were applied and pearson chi -square test was used to test variables. The collected data was analyzed statistically using the chi- square test at the significance level of P<0.05.
Chi square test
It's a non parametric test, used when data were expressed in frequency or proportion or percentages. Chi square test is used to evaluate the statistical significance of differences in frequencies between subgroups. Chi square checks the difference between observed and expected values. The formula used for chi square test is:
Where,
∑ = Denotes summation
O = Observed frequency
E = Expected frequency
P value denotes level of significance:
P >0.05 Non significant
P <0.05 Significant
P <0.01 Highly Significant (Significant at 99% confidence level)
P <0.001 Very highly Significant (Significant at 99.9% confidence level)
Results
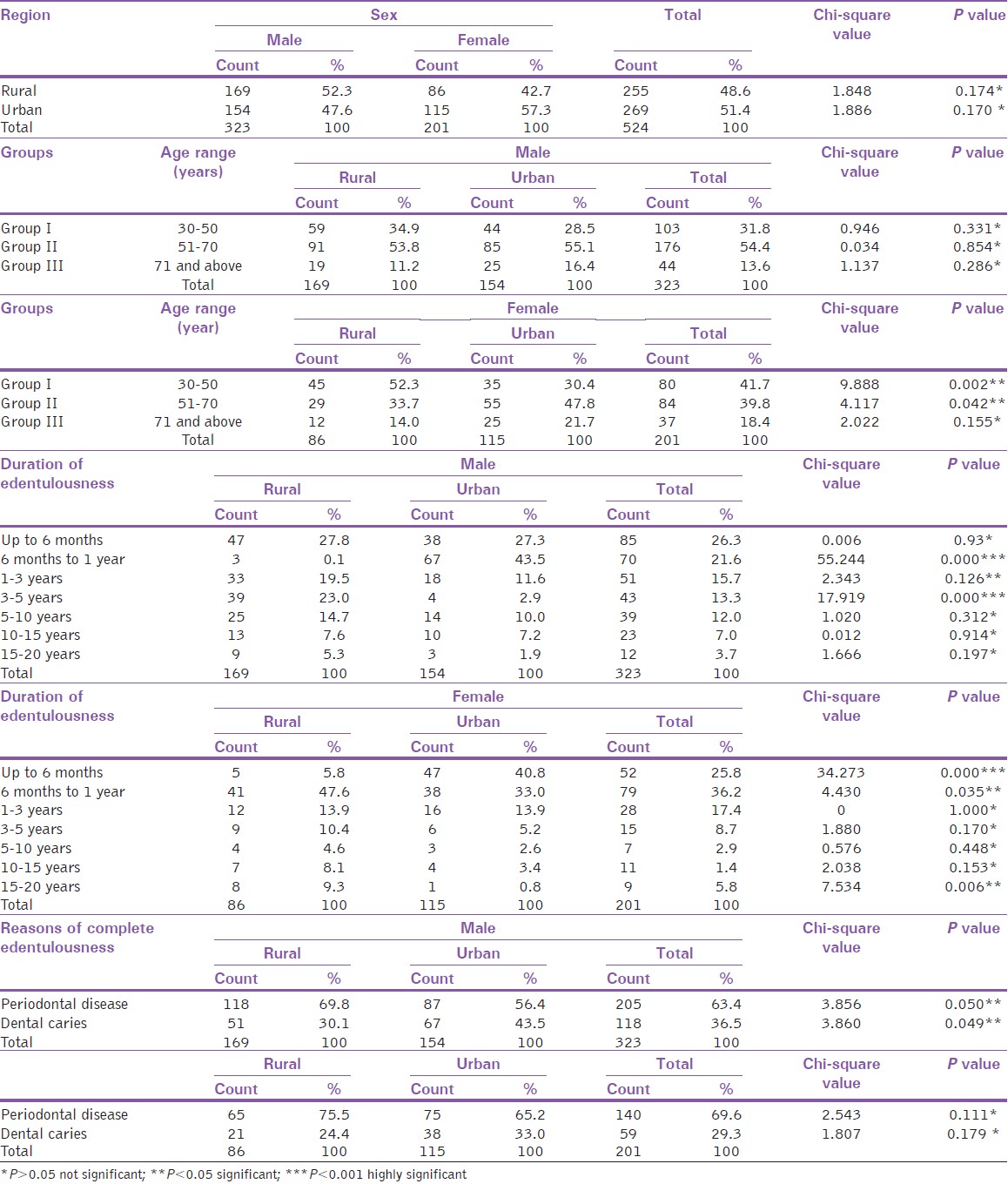
Out of 524 completely edentulous subjects, 255 (48.6%) were from rural region and 269 (51.4%) were from urban region. Out of 323 male subjects, 169 (52.3%) were from rural and 154 (47.6%) were from urban region. Out of 201 female subjects, 86 (42.7%) were from rural and 115 (57.3%) were from urban region. The P value was non-significant for both rural and urban region. In the rural region, a maximum number of subjects were in Group II and minimum were in Group III. Out of 154 subjects of the urban region, a maximum number of subjects were in Group II and minimum were in Group III. For all age groups of rural and urban region, the P value was non-significant. In the rural region, out of 86 subjects, a maximum number of subjects were in Group I and minimum were in Group III. Out of 115 subjects of the urban region, a maximum number of subjects were in Group II and minimum were in Group III. For age Group III, the P value was non-significant. The P value was significant for both Group I and II. In the rural region, out of 169 subjects, a maximum numbers of subjects were in a category of age group up to 6 months and minimum were in 6 months to 1 year. In the urban region, out of 154 subjects, a maximum numbers of male subjects were in 6 months to 1 year and minimum were in a category of up to 6 months. The P value was highly significant for age group 6 months to 1 year and 3-5 years. The P value was non-significant for other age groups. In the rural region, out of 86 subjects, 5 (5.8%), 41 (47.6%), 12 (13.9%), 9 (10.4%), 4 (4.6%), 7 (8.1%), 8 (9.3%) were found edentulous in a category of up to 6 months, 6 months to 1 year, 1-3 years, 3-5 years, 5-10 years, 10-15 years and 15-20 years respectively. Maximum numbers of female subjects were in the age group of 6 months to 1 year and minimum were between 5 and10 years. In the urban region, out of 115 subjects, a maximum number of female subjects were in 6 months to 1 year age group and minimum were between 5 and10 years. The P value was highly significant for up to 6-month age group. The P value was non-significant for age groups 1-3 years, 3-5 years, 5-10 years and 10-15 years. The P value was significant for age group 6 months to 1 year and 15-20 years. In the rural region, out of 169 subjects, 118 (69.8%) were edentulous due to periodontal disease. 51 (30.1%) were edentulous due to dental caries. In the urban region, out of 154 subjects, 87 (56.4%) were edentulous due to periodontal disease. 67 (43.5%) were edentulous due to dental caries. Trauma was not causative factor for edentulism in both rural and urban region. The P value was significant for both periodontal disease and dental caries. In the rural region, out of 86 subjects, 65 (75.5%) were edentulous due to periodontal disease. 21 (24.4%) were edentulous due to dental caries. In an urban region, out of 115 subjects, 75 (65.2%) were edentulous due to periodontal disease. 38 (33%), 2 (2.3%) were edentulous due to trauma. The P value was non-significant for periodontal disease, dental caries and trauma [Table 1].
| Discussion | | |
This study is the first that has evaluated the relationship between age, tooth loss and the frequency of edentulism at a Department of Prosthodontics at a University in India. There are many variables affecting the quality-of-life out of which tooth loss is one of the premier factors. The loss of one or more teeth can have profound effects on an individual oral health and quality-of-life. [5] One concept that has received particular attention when setting health targets is that of a minimum threshold for the number of teeth below, which oral function and health diminish rapidly. Such concepts originally arose with the works of Agerberg and Carisser [6] and Käyser [10] two decades ago. Besides the foremost factor age and tooth loss both have their variable effects on different age groups affecting the quality-of-life. For an example, in case of infants and small children, tooth loss hampers speech and sucking while in teenagers aesthetics is of major concern, which affects the quality-of-life while performing day-to-day tasks. In addition, along with teeth, several other factors affect the oral health related quality-of-life, the most important among which is personal habit, which includes tobacco usage both in smoking and nonsmoking forms and also alcohol consumption.
The rate of edentulism is estimated at 30% for African Americans, American Indians or Alaska Natives for this age group, 26% for Caucasians and 24% for Hispanics. [7] While the women have been reported to lose all their teeth at a higher rate (3% higher in the USA) than men, this trend appears to be country specific. [7]
According to gender, 323 subjects were male and 201 subjects were female. This tendency for more number of male than female subjects is consistent with some studies, [11] but not with others. [1],[2],[7],[8] Suominen-Taipale et al. concluded that in 1978 edentulism was found to be more in females than males, but in 1997, the difference between sexes had almost disappeared. [2] The reason can be attributed to the fact that females were dependent upon the male members of the family to take them for treatment. [8] Males were not dependent upon any one and they can easily come for treatment.
According to the region, out of 323 male subjects, 169 subjects were from the rural region and 154 subjects were from the urban region. The reasons could be attributed to the fact that there is no health care system in rural areas with the dentist population ratio of about 1:200,000. Only 25% community health centers are having posting of dental surgeons, but have inadequate instruments, equipments and dental materials so they were dependent upon nearby dental colleges for complete denture treatment.
According to the region, out of 201 female subjects, 86 subjects were from the rural region and 115 subjects were from the urban region. This could be because women in the urban region had a better health seeking behavior and were more conscious of their appearance. [8] Ronald Ettinger and Annette found that people living in urban population (52%) were least likely to be edentulous than rural population (48%). [12],[13]
According to age-wise distribution of subjects, highest percentage of complete edentulousness in female subjects was found in the age group of 30-50 years and 51-70 years in rural (52.3%) and urban region (47.8%), respectively. This showed that females were becoming edentulous at an early age than males. [1],[3],[13],[14],[15],[16],[17] This could be because rural females had a lower level of education and they could not have afforded treatment procedures that would have save their tooth in question and therefore opted for extraction. [8],[15],[18],[19] This observation that edentulousness increases with age is in agreement with the finding of other studies. [20],[21],[22],[23],[24] In the urban region, females were more concern about their oral hygiene and they preferred conservative treatment rather than extraction. [25] Highest percentage of male subjects was found in the age group of 51-70 years in both rural (53.8%) and urban (55.1%) regions. Majority of dental colleges and teaching institutions were located in urban areas so they had a better access to treatment. In females edentulousness was increased between age groups of 30-44, 45-59, 60-64 and then decreased. According to duration of complete edentulousness, maximum percentage of males was found in the category of up to 6 months (27.8%) in the rural region. This observation can be associated with the fact that dental surgeons are not posted at the level of primary health center in most rural areas of India. Provision of dental care in rural areas should not be limited to treatment alone, but should focus on empowering the community through dental health education to increase acceptability of services leading to greater utilization of curative care. [26],[27],[28] The rural subjects were economically poor and generally employed in urban areas. This saves their time and expenditure so they reported within 6 months. Maximum percentage of male subjects were in 6 months to 1 year (43.5%) in the urban region the reason was that they wait for at least 6 months because they were aware that bone required time for proper healing. Maximum percentage of female subjects were found in the category of 6 months to 1 year (47.6%) and up to 6 months (40.8%) in rural and urban region, respectively; the reason was that the females in the rural region were busy all day doing house hold works and there was a lack of awareness among them. [8],[29],[30] Females in the urban region were educated and they can come alone that's why they reported within 6 months.
In Sweden, the introduction of a general dental health insurance system has during the last few decades probably improved the attitudes toward saving teeth instead of extracting them. [9] This study showed that periodontal disease was the major cause for edentulousness and then dental caries and lastly trauma. Some other studies have also shown similar significant findings, [2],[3],[9],[31] but not others. [2],[9],[12] However, it is documented in the literature that dental caries was the most prevalent reason rendering the patients edentulousness. [2]
Periodontal disease and dental caries have been considered as main determinants for the high occurrence of tooth loss and consequently for the high percentage of edentulism. [2],[3],[21] Identifying failure to visit the dentist regularly was also found to be a major reason. [6] Age was strongly associated with edentulism, [3],[4],[13],[25],[32],[33],[34] This finding was not surprising because the cumulative effects of dental caries and periodontal diseases as well as treatment decisions associated with these two main reasons, increase with age. [1],[2],[3] Differential treatment choice across the socio-economic conditions, like endodontic versus tooth extraction, also may play the role in the overall tooth loss phenomenon. [9],[11],[12],[17],[19],[31]
The consequences of complete edentulism on the oral and facial structures are well-known criteria for predicting the long-term effects of tooth removal on any individual patient are currently lacking. A greater awareness regarding proper dental hygiene and timely replacement of the missing teeth needs to be stressed among the general public. [35]
| Conclusion | | |
Age, gender, and tooth loss are associated with each other, but they have independent effects on the oral health-related quality-of-life. Tooth loss, which is associated with the increase of age, is associated with more negative impacts while the increase of age independently results in fewer. It is essential to identify feasible strategies to provide primary dental health education and treatment to all rural and urban elderly in the future. We suggest community dental health services as a general health need of the elderly rather than a special health need of the community. Incorporating primary, as well as rehabilitative dental care services under the existing rural health infrastructure may be an effective method to improve access to oral health-care for the elderly in developing countries.
| Acknowledgment | | |
I would like to thank the trustees of Darshan Dental College Mr. B R Agarwal, my HOD Dr. Suresh S for helping me in completing my thesis work.
| References | | |
| 1. | Xie Q, Ainamo A. Association of edentulousness with systemic factors in elderly people living at home. Community Dent Oral Epidemiol 1999;27:202-9. 
[PUBMED] |
| 2. | Suominen-Taipale AL, Alanen P, Helenius H, Nordblad A, Uutela A. Edentulism among Finnish adults of working age, 1978-1997. Community Dent Oral Epidemiol 1999;27:353-65.
[PUBMED] |
| 3. | Takala L, Utriainen P, Alanen P. Incidence of edentulousness, reasons for full clearance, and health status of teeth before extractions in rural Finland. Community Dent Oral Epidemiol 1994;22:254-7.
[PUBMED] |
| 4. | Hunt RJ, Beck JD, Lemke JH, Kohout FJ, Wallace RB. Edentulism and oral health problems among elderly rural Iowans: The Iowa 65+rural health study. Am J Public Health 1985;75:1177-81.
[PUBMED] |
| 5. | Slade GD, Spencer AJ. Social impact of oral conditions among older adults. Aust Dent J 1994;39:358-64.
[PUBMED] |
| 6. | Agerberg G, Carisser GE. Chewing ability in relation to dental and general health. Analysis of data obtained from a questionnaire. Acta Odontol Scand 1981;39:147-53.
|
| 7. | Felton DA. Edentulism and comorbid factors. J Prosthodont 2009;18:88-96.
[PUBMED] |
| 8. | Prabhu N, Kumar S, D'Souza M, Hedge V. Partial edentulousness in rural population based on Kennedy's classification: An epidemiological study. J Indian Prosthodont Soc 2009;9:18-23.
 |
| 9. | Fure S, Zickert I. Prevalence of root surface caries in 55, 65, and 75-year-old Swedish individuals. Community Dent Oral Epidemiol 1990;18:100-5.
[PUBMED] |
| 10. | Käyser AF. Shortened dental arches and oral function. J Oral Rehabil 1981;8:457-62.
|
| 11. | Sakki TK, Knuuttila ML, Vimpari SS, Hartikainen MS. Association of lifestyle with periodontal health. Community Dent Oral Epidemiol 1995;23:155-8.
[PUBMED] |
| 12. | Bouma J, Schaub RM, van de Poel F. Periodontal status and total tooth extraction in a medium-sized city in the Netherlands. Community Dent Oral Epidemiol 1985;13:323-7.
[PUBMED] |
| 13. | Ettinger RL, Beck JD, Jakobsen J. Removable prosthodontic treatment needs: A survey. J Prosthet Dent 1984;51:419-27.
[PUBMED] |
| 14. | Shah N. Gender issues and oral health in elderly Indians. Int Dent J 2003;53:475-84.
[PUBMED] |
| 15. | Shah N, Parkash H, Sunderam KR. Edentulousness, denture wear and denture needs of Indian elderly: A community-based study. J Oral Rehabil 2004;31:467-76.
[PUBMED] |
| 16. | Ahlqwist M, Bengtsson C, Gröndahl HG, Halling A. Tooth mortality in women in a 12-year follow-up of a population sample in Gothenburg, Sweden. Community Dent Oral Epidemiol 1986;14:358-61.
|
| 17. | Chauncey HH, Baric JM, Alman JE, Feldman RS. Longitudinal study of tooth loss and caries prevalence in healthy male adults. Gerodontics 1987;3:38-42.
[PUBMED] |
| 18. | Hand JS, Kohout FJ, Cunningham MA. Incidence of edentulism in a non-institutionalized elderly population. Gerodontics 1988;4:13-7.
[PUBMED] |
| 19. | Ahlqwist M, Bengtsson C, Gröndahl HG, Lapidus L. Social factors and tooth loss in a 12-year follow-up study of women in Gothenburg, Sweden. Community Dent Oral Epidemiol 1991;19:141-6.
|
| 20. | Shetty P, Bhargava K, Goel P, Saha R. Edentulousness and prosthetic needs of a rural population in Southern India. J Indian Prosthodont Soc 2001;1:20-5.
|
| 21. | Angelillo IF, Sagliocco G, Hendricks SJ, Villari P. Tooth loss and dental caries in institutionalized elderly in Italy. Community Dent Oral Epidemiol 1990;18:216-8.
[PUBMED] |
| 22. | Nuttall NM, Nugent ZJ. Indicators of dental extractions and full mouth clearances: A longitudinal analysis. Community Dent Oral Epidemiol 1997;25:181-3.
[PUBMED] |
| 23. | Krall EA, Garvey AJ, Garcia RI. Alveolar bone loss and tooth loss in male cigar and pipe smokers. J Am Dent Assoc 1999;130:57-64.
[PUBMED] |
| 24. | McCord JF, Grant AA. Complete dentures: An introduction. Br Dent J 2000;188:373-4.
[PUBMED] |
| 25. | Douglass C, Gillings D, Sollecito W, Gammon M. The potential for increase in the periodontal diseases of the aged population. J Periodontol 1983;54:721-30.
[PUBMED] |
| 26. | Goel P, Singh K, Kaur A, Verma M. Oral healthcare for elderly: Identifying the needs and feasible strategies for service provision. Indian J Dent Res 2006;17:11-2.
[PUBMED] |
| 27. | Medina-Solís CE, Pérez-Núñez R, Maupomé G, Casanova-Rosado JF. Edentulism among Mexican adults aged 35 years and older and associated factors. Am J Public Health 2006;96:1578-81.
|
| 28. | Kozma A, Marti GP, Mats T. Ageing in disguise: Age, period and cohort effects in mobility and edentulousness over three decades. Eur J Ageing 2007;4:83-91.
|
| 29. | Rihs LB, da Silva DD, de Sousa Mda L. Dental caries in an elderly population in Brazil. J Appl Oral Sci 2009;17:8-12.
[PUBMED] |
| 30. | Idowu OE, Al-Shanrani SM. Pattern of tooth loss in a selected population at King Saud University College of Dentistry. Saudi Dent J 2009;3:6.
|
| 31. | Marcus PA, Joshi A, Jones JA, Morgano SM. Complete edentulism and denture use for elders in New England. J Prosthet Dent 1996;76:260-6.
[PUBMED] |
| 32. | Brauer L, Bessermann M, Frijs-Madsen B, Brauer E. Oral health status and needs for dental treatment in geriatric patients in a Danish District Hospital. Community Dent Oral Epidemiol 1986;14:132-5.
[PUBMED] |
| 33. | Nicholls. A study of periodontal disease and tooth loss over 12 years. Br Dent J 2000;188:98-9.
|
| 34. | Lopez R, Baelum V. Classifying periodontitis among adolescents: Implications for epidemiological research. Community Dent Oral Epidemiol 2003;31:136-43.
[PUBMED] |
| 35. | Axelsson G, Helgadóttir S. Edentulousness in Iceland in 1990. A national questionnaire survey. Acta Odontol Scand 1995;53:279-82.
|
[Table 1]
|









 Search Pubmed for
Search Pubmed for