|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 33-36 |
|
Prosthetic management of ocular defects: A case series
Laxman Singh Kaira1, Rahul Bhayana2, Vipul Asopa3, Achyut N Pandey3, Esha Dabral4
1 Department of Dentistry, Veer Chandra Singh Garhwali Government Medical Sciences and Research Institute, Srinagar, Pauri Garhwal, Uttrakhand, India
2 Department of Prosthodontics, Mahatma Gandhi Dental College and Hospital, Sitapura, Jaipur, Rajasthan, India
3 Department of Prosthodontics, Darshan Dental College and Hospital, Udaipur, Rajasthan, India
4 Department of Opthalmology, Veer Chandra Singh Garhwali Government Medical Sciences and Research Institute, Srinagar, Private practionner, Srinagar Garhwal, Uttrakhand, India
| Date of Web Publication | 12-Dec-2013 |
Correspondence Address:
Laxman Singh Kaira
Department of Dentistry, Veer Chandra Singh Garhwali Government Medical Sciences and Research Institute, Type 2, House No. 4, Block no. 2, Faculty Residence, VCSGGMSRI Campus, Srinagar, Pauri Garhwal, Uttrakhand
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.122992

An ocular prosthesis is a simulation of a perfectly normal healthy eye and surrounding tissues. The primary purpose of an ocular prosthesis is to maintain the volume of eye socket and create the illusion of a healthy eye and surrounding tissue. A custom ocular prosthesis is a good option when reconstruction by plastic surgery or the use of osseointegrated implants is not possible or not desired. Prosthetic rehabilitation of a patient with missing eye with custom made ocular prosthesis was described. Keywords: Custom made ocular prosthesis, eye, ocular defect
How to cite this article:
Kaira LS, Bhayana R, Asopa V, Pandey AN, Dabral E. Prosthetic management of ocular defects: A case series. Eur J Prosthodont 2014;2:33-6 |
| Introduction | |  |
Eyes are generally the first features of face to be noticed. Removal of this organ either due to tumors, trauma, or any other condition not only cause unaesthetic look but causes of function and has a psychological effect on the patient. The surgical procedures removal of an eye, as described by Peyman, Saunders, and Goldberg into three general categories as "evisceration, enucleation, and exenteration." [1] The surgical process evisceration is where the contents of the globe are removed, leaving the sclera and extraoccular muscles intact. A more invasive procedure is enucleation where there is removal of eye from the orbit while preserving all other orbital structures. Exenteration, which is the most radical, involves removal of the eye, adnexa, and part of bony orbit. Immediate replacement of the lost eye is necessary to promote physical and psychological healing for the patient and to improve social acceptance. The objective of the maxillofacial prosthetic team is to provide the ocular prosthesis to the patient in as comfortable and atraumatic manner as possible. [2] Until World War II, the glass eye was the most popular eye prosthesis. The glass eye was, however, difficult to manufacture and hazardous. The methyl methacylate prosthesis became popular since they offered superior strength and permitted modifications in shape and size. [3]
Flexible material such as silicone [4] is advantageous when the defect extends beyond orbital area and encounters movable tissue beds. A definitive technique for fabricating artificial eyes using acrylic resins was developed by the United States Naval Dental and Medical schools and was published in 1944. The material was lightweight, easy to fit, translucent easily fabricated, had intrinsic and extrinsic coloring capabilities, and was inert to the socket secretions. [5],[6],[7]]
An ocular prostheisis can be either stock or custom made. Stock prosthesis comes in standard shapes, sizes, and color. Custom eyes have several advantages including better mobility, even distribution of pressure due to equal movement thereby reducing the incidence of ulceration, improved fit, improved facial contours, comfort and enhanced esthetic gained from the controlled size of the iris, pupil, and colors of the iris and sclera. [7],[8],[9]
| Case Report | | |
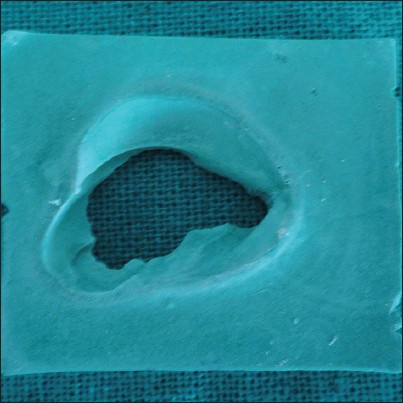
A 35-year-old male patient reported to the Department of Ophthalmology for the chief complaint of pain, bulging, and whitish appearance of the left eye. He was diagnosed with anterior staphyloma after which enucleation was conducted. The patient was then referred to the Department of Prosthodontics for the fabrication of an eye prosthesis. On examination, the defect area was found to be asymptomatic [Figure 1] and it was decided to fabricate an ocular prosthesis. The treatment plan was explained to the patient and an informed consent obtained.
Evaluation of patient ocular defect
In a case of evisceration the extraocular muscles are left intact and hence good mobility of the prosthesis is possible. Therefore, it becomes mandatory to do the defect evaluations. According to the standard procedure, the palpebral fissure was observed both in open and closed positions to rule out any abnormality. Evaluation of the muscular control of the palpebrae and the internal anatomy of the socket in the resting position and full excursive movement was performed. Mobility of the posterior wall of the defect was assessed. Condition of conjunctiva, depth of fornices, and presence of cul-de-sac was noted.
Materials and techniques
The patient was placed in the supine position and draped for the impression procedure. The remnants of the patients' eyebrows and the area of the skin covering the defect and the upper two-third of the face was lubricated with petroleum jelly.
Impression of ocular defect
Direct impression
A low viscosity alginate (Neocolloid Zhermack, Kab Dental supplies) is injected directly into the enucleated socket. The patient is instructed to stare straight ahead as the materials set [Figure 2]. After the impression material was set, the impression was removed and invested in dental gypsum to obtain a positive cast of the eye socket.
Subsequently, the gypsum cast was coated with a separating medium and white paraffin wax was then shaped in an empirical approximation of the anterior curves of the investment form [Figure 3].
Try-in of sclera wax pattern
Wax was added or trimmed from the basic sclera pattern until satisfactory contours of the eyelids were achieved in open and closed positions [Figure 4].
Techniques of iris disc placement:
- Transparent graph grid was used to attach irisdisc
- Certain guidelines were marked on patients' face
- The facial markings were transferred to the grid by placing it on patients' face in place.
Transparent graph grid
Markings were made on the grid template on the X-axis from A to H starting from midline and on the left side from A′ to H′. Similarly, from 1 to 7 on Y-axis and 1′ to 7′ on the left side. The distance between each marking was 1 cm on both X and Y axes.
Guidelines on patients' face
A vertical midline was marked passing through the forehead crease, glabella, tip of the nose, and chin. The distance from the right eye medial canthus to the midline and left eye medial canthus to the midline was measured. This distance standardized the midline marking and was used to reposition the grid template each time during the try-in visit.
Evaluation with grid placed
The patient was asked to gaze straight at an object kept 4 ft away. The vertical lines coinciding with the medial and distal extremities of the iris of the natural eye. Similarly, the horizontal lines referring to the center, inferior, and superior limits of the iris were marked. The facial markings were transferred to the grid template by placing it on the patients' face.
Investing, dewaxing, and packing
The finished pattern was invested in a small two piece brass flask. A two-part mold was constructed by the prototype ocular shell by using dental gypsum in a two-piece brass flask, the anterior portion of the mold was invested, a separating medium was applied and the posterior portion of the mold was then invested. The flask was then placed in a dewaxing bath for 20 minutes. The anterior and posterior portions of the flask were separated. The iris disc was shade matched with the adjacent eye and cut out from a stock eye. The color of the sclera was selected using the tooth color acrylic shade guide. Rayon thread fibrils were used to simulate vasculature, by the monomer polymer syrup method. The selected shade of the sclera was matched with the heat cure resin which was then packed in the two-piece flask. The flask was kept for curing for a period of 2 h and 30 min to avoid any residual monomer.
Placement of ocular prosthesis
The patient was instructed on the aspects of insertion and easy removal of the prosthesis [Figure 5]. Prior to insertion of the polished prosthesis, it was disinfected in a solution of 0.5% chlorhexidine and 70% isopropyl alcohol for 5 min. After disinfection, the prosthesis was rinsed in sterile saline solution to avoid chemical irritation and finally the ocular prosthesis was inserted and postinsertion instructions were given.
Patient instructions
- The method of insertion and removing the prosthesis and its care were demonstrated to the patients
- The prosthesis should be removed at least once a day for cleaning. Cleaning should be done with a mild soap or detergent to avoid crazing, pitting, or clouding of the prosthesis. The patient was asked to return on day 1, 2, and 7 for follow-ups after the prosthetic insertion. There after a 6-month follow-up was done for prosthesis evaluation and adjustment. [10]
| Discussion | | |
The custom-made ocular prosthesis conforms accurately to the socket as the ocular prosthesis fabrication is based on the existing anatomy of the patient, thus giving benefits of increased adaptation, movement of the eyeball, and the exact match of the iris position, as that of adjacent natural eye. [4] The fabrication of a custom acrylic eye provides more esthetic and precise results because an impression establishes the defect contours and the iris and the sclera are custom fabricated. [6]
In this case, retention was achieved by the deep anatomical site of defected area. Nowadays, numerous methods of retention for ocular prostheses have been described in the literature; they include eyeglasses, magnets, and osseointegrated implants. Although osseointegrated implant may provide the most reliable prosthesis retention, additional surgeries, expenses may contraindicate this type of treatment. [11] A subjective measurement of the patient was evaluated to assess the improvement in quality-of-life (QOL). Chang et al. proposed a standard questionnaire to evaluate the patient's satisfaction with facial prosthesis. [12] However, QOL can be used to evaluate patient outcome in any treatment and treated as a "subjective multidimensional concept." [13] In the described case, the patient explained that retention and overall appearance were fair and satisfactory, wearing and cleaning of prosthesis was comfortable, and there was no problem regarding tissue discomfort. This inferred that the patient had overall improvement in QOL during the observation period.
| Conclusion | | |
The use of custom-made ocular prosthesis has been a boon to the average patient, who cannot afford the expensive treatment options available. The esthetic and functional outcome of the prosthesis is superior to stock ocular prosthesis. Although many treatment options are available, the conventional method is most widely used all over India.
| References | | |
| 1. | PermanKI, Baylis HI. Evisceration, enucleation, and exenteration. Otolaryngeal Clin North Am 1988:21;171-82. 
|
| 2. | Lal S, Schwartz AB, Gandhi T, Moss ML. Maxillofacial prosthodonticsfor the paediatric patient: "An eye-opening experience". J ClinPediatr Dent 2007;32:5-8.
|
| 3. | Taicher S, Steinberg HM, Tubiana I, Sela M. Modified stock-eye ocular prosthesis. J Prosthet Dent 1985;54:95-8.
|
| 4. | Supriya M, Ghadiali B. Prosthetic rehabilitation of a patient with an orbital defect using a simplified approach. J Indian Prosthodontic Soci . 2008;8:116-8.
|
| 5. | Rahn AO, Boucher LJ. Orbital and ocular prosthesis. In: Rahn AO, ed. Maxillofacial Prosthetics-Principles and Concepts. 3 rd ed. Philadelphia, W.B.: Saunders Publishers; 1970. p. 151-68.
|
| 6. | Artopoulou II, Montgomery PC, Wesley PJ, Lemon JC. Digital imaging in the fabrication of ocular prostheses. J Prosthet Dent 2006;95:327-30.
|
| 7. | Cerullo L, Mckinstry RE. Ocular prosthesis. In: Mckinstry RE, editor. Fundamentals of Facial Prosthesis. Arlington: ABI Professional Publishers; 1995. p. 99-120.
|
| 8. | El-Dakkak M. Problem solving techniquein ocular prosthesis reconstruction. Saudi Dent Jour 1990;2:7-10.
|
| 9. | Kale E, Meºe A, Izgi AD. A technique for fabrication of an interim ocular prosthesis. J Prosthodont 2008;17:654-61.
|
| 10. | Agarwal KK, Mall P, Alvi HA, RaoJ, Singh K. Fabrication of custom-made eye prosthesis for anophthalmicpaediatric patients: 2 case reports. J Interdiscip Dent 2012;2:128-31.
|
| 11. | Chang TL, Garrett N, Roumanas E, Beumer J 3 rd . Treatment satisfaction with facial prostheses. J Prosthet Dent 2005;94:275-80.
|
| 12. | Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, et al. The functional assessment of cancer therapy scale: Development and validation of the general measure. J ClinOncol 1993;11:570-9.
|
| 13. | Pflughoeft FA, Shearer HH. Fabrication of a plastic facial moulage. J Prosthet Dent 1971;25:567-71.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|













 Search Pubmed for
Search Pubmed for