|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 3 | Page : 76-81 |
|
A comparative clinical and quantitative evaluation of the efficacy of conventional and recent gingival retraction systems: An in vitro study
Deepti Raghav1, Satyavir Singh2, Mohammed Zaheer Kola3, Altaf Hussain Shah4, Hesham Saleh Khalil5, Prince Kumar1
1 Department of Prosthodontics, Shree Bankey Bihari Dental College, Ghaziabad, Saudi Arabia
2 Santosh Dental College, Ghaziabad, Saudi Arabia
3 Department of Prosthodontics, College of Dentistry, Salman bin Abdulaziz University, Alkharj, Saudi Arabia
4 Department of Preventive Dental Sciences, Salman bin Abdulaziz University, Alkharj, Saudi Arabia
5 Department of Maxillofacial Surgery, College of Dentistry, King Saud University, Saudi Arabia
| Date of Web Publication | 10-Sep-2014 |
Correspondence Address:
Deepti Raghav
Department of Prosthodontics, Shree Bankey Bihari Dental College and Research Centre, Masuri, Ghaziabad - 201302, Uttar Pradesh
Saudi Arabia
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.140514

Aim: Gingival deflection techniques can be classified as mechanical, mechanochemical, surgical, or any combination. Comparative evaluations of gingival retraction systems are done rarely mainly because there is no consensus on the evaluation criteria. Therefore, this study aimed to evaluate the efficacy of three different gingival retraction systems, i.e., Magic Foam Cord, expasyl paste, and aluminium chloride-impregnated retraction cord. Materials and Methods: Following impressions, obtained casts were measured for gingival sulcus opening width under optical microscope (with imaging system software). The presence of bleeding after removal of material, ease of procedure, and patient's comfort were also evaluated. The data collected were tabulated and subjected to statistical analysis. Results and Conclusion: Evaluation of the clinical efficacy is relatively difficult because of the lack of appropriate measuring tool. In addition, choice of appropriate gingival retraction system is still a dilemma for the operator. Moreover, a particular clinical situation may indicate the specific technique. Keywords: Gingival retraction, gingival sulcus width, optical microscope with imaging system software
How to cite this article:
Raghav D, Singh S, Kola MZ, Shah AH, Khalil HS, Kumar P. A comparative clinical and quantitative evaluation of the efficacy of conventional and recent gingival retraction systems: An in vitro study
. Eur J Prosthodont 2014;2:76-81 |
How to cite this URL:
Raghav D, Singh S, Kola MZ, Shah AH, Khalil HS, Kumar P. A comparative clinical and quantitative evaluation of the efficacy of conventional and recent gingival retraction systems: An in vitro study
. Eur J Prosthodont [serial online] 2014 [cited 2018 Jul 5];2:76-81. Available from: http://www.eurjprosthodont.org/text.asp?2014/2/3/76/140514 |
| Introduction | |  |
To make accurate impressions, we must be able to visualize the margins of our preparations clearly. Effective gingival retraction is required to open a space surrounding the preparation margin and leave a clean dry field in which to take the impression. If our margins are supragingivally located, capturing them is relatively simple. However, much of the time, the margins are placed subgingivally beyond the presence of existing large restorations or below the gingival crest, for esthetic reasons. A clear dry field, free of blood is the most important element necessary to obtain a good impression. Sulcular bleeding must be controlled before taking the impression. Adequate retraction must be accomplished in all subgingival areas to guarantee that the impression material or digital scan registers beyond the preparation margin. Several different methods of retraction are in use today, the most popular of which are (1) cords (2) laser or electrosurge, and (3) paste systems. Recognition of the preparation margin enables a technician to fabricate a prosthesis having a smooth transition from the prosthesis to the tooth structure. The configuration and location of margin that is in the proximity of the gingival tissue (i.e., cervical finish margin) is difficult to record until the soft tissue is displaced to expose the tooth surface more cervically. [1] There is a continuous endeavor to research and develop a suitable material and technique for this purpose. The mechanico-chemical method of using a retraction cord soaked in various chemicals is the most frequently used method. [2],[3],[4] Utmost care has to be taken while placing retraction cord to avoid any physical trauma to the tissue. [5],[6] Also the chemical may produce undesirable side effects. This has led to the development of some other methods like using a paste containing kaolin and aluminium chloride or using foam, a cordless technique containing addition cure polyvinyl siloxane. This study was conducted to compare the clinical efficacy of three different gingival retraction systems, ease of their application and removal, comfort of the patient as well as post-retraction gingival health.
| Materials and Methods | | |
The study was conducted on healthy unblemished maxillary right first molar of 25 selected human participants of 20-25 years of age range. All patients were selected through the Department of Prosthetic Dentistry, Santosh Dental College, Ghaziabad, India. The patients required various types of indirect fixed restorations in anterior and posterior teeth. As part of preliminary treatment, all patients took part in the dental hygiene program available at the clinic. Before preparation, all teeth had to be free of active periodontal inflammation and have probing depths <3 mm and no bleeding on probing. Further, participants with no significant difference in gingival sulcus depth at transitional line angles and mid buccal areas were only included in the study. Basic materials used for three different methods of gingival displacement were Magic Foam Cord (Coltene/Whaledent Company) [Figure 1], expasyl paste (Satellec Company) [Figure 2], and ultra pack retraction cord impregnated with aluminium chloride [Figure 3] with a safe concentration level of upto 25%. Addition silicone (Light Body Consistancy; Dentsply, India) was used to make the impression. Casts with individual dye were made in type IV Die Stone (Kalrock, Kalabhai Dental Products, India) [Figure 4]. Optical microscope attached to Axiovision (AC Soft Imaging System Software) [Figure 5] was used to measure the width of gingival sulcus [Figure 6]. Four impressions were made for each participant at the time interval of 8 days-one without gingival displacement and the rest three after gingival displacement using three different retraction systems following manufacturer's instructions for their use. Die stone models thus obtained were sectioned along the buccal groove of the maxillary right first molar vertically. Each model was given a label-1A, 1B, 1C, 1D.; 2A, 2B.-25A, 25B.-where numerical denoted the participant and the alphabet indicated retraction method or no retraction. (A - no retraction, B - Magic Foam Cord, C - expasyl paste gingival retraction system, D - aluminium chloride-impregnated retraction cord.)
The sulcus width or amount of gingival retraction was measured as the distance from the tooth to the crest of the gingiva in the horizontal plane. This was done by placing the half section of the model under optical microscope-Axioskop [Figure 4] attached to software system (Axiovision; Ac soft imaging system software). The amount of retraction was calculated by subtracting the measured width (gingiva to the tooth) before retraction from the one which was after retraction. Ease of application and removal of each retraction system was evaluated subjectively. To evaluate the effects of retraction on the health of gingival tissue health, the participants were again reviewed for periodontal health after 8 days of gingival retraction for any evidence of gingival inflammation, change in gingival contour, and bleeding on probing.
| Results | | |
Observations were subjected to statistical analysis. Mean and standard deviation were calculated and Student's "t0" test was applied to statistically analyze the data. Because the observations related to bleeding were taken on scale instead of actual value, a non-parametric test "Wilcoxon Singed Rank's test" was used to compare the material used in the study.
Dentists today desire "smart" products designed to make their jobs faster and easier. In recent years, several retraction paste systems have entered the dental marketplace, claiming to be convenient, fast, and effective. Providing a proper technique is followed, these products are simple to use and can be gentler than cord to the gingival tissues. All the currently available paste systems have a similar placement protocol. Deflecting the gingiva during tooth preparation to establish the margin or exposing the gingival margin of gingival tissues, degree of inflammation, level of margin placement and tissue laceration, and skill of the a preparation before impression making may be one of the difficult procedures for the dentist to perform. The difficulty of the procedure is further complicated by variations in sulcular depth and distensibility of the operator. Basically, any technique used, should create adequate space between the gingival finish line and the gingival tissue to allow the margin of the prepared tooth to be recorded in an impression medium, provide absolute control of gingival fluid seepage and hemorrhage (dry field) especially when hydrophobic elastomeric impression materials are used, should not cause significant irreversible soft or hard tissue damage, and should not produce any potentially dangerous systemic effects. As the purpose of the study was to find out the most effective, painless, and easiest retraction system to be used by the operator, this was carried out by comparing the traditional retraction system of packing the impregnated retraction cord with newer injectable systems like expasyl paste and Magic Foam Cord. To have more chances of optimum gingival health, participants from younger age group of 20-25 years were selected. With advancing age, the health of gingiva deteriorates and the architecture changes. Moreover, healthy gingiva was required to check bleeding due to trauma from retraction procedure and material. All participants demonstrated good oral hygiene, and the gingiva was in optimum health. Eight-days interval was maintained in between retractions as the epithelium, if traumatized heals within 8 days [Figure 7]. [7],[8],[9],[10]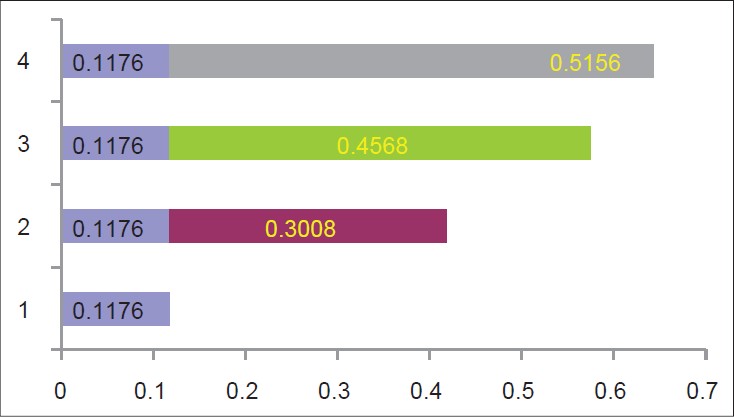 | Figure 7: Amount of gingival sulcus retracted with retraction and without retraction, Blue - Without retraction, Purple - Magic foam cord, Green - Expasyl paste, Grey - Aluminum chloride retraction cord
Click here to view |
Protocols for the use of the retraction cord, expasyl paste, and Magic Foam Cord were carefully followed. Twenty minutes were allowed for the cord to soak in the aluminum chloride solution, to ensure uniform impregnation by the chemical. Cords were left in sulcus for no longer than 10 min to avoid any permanent damage to epithelial attachment. [11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22] Most common method of making the working model, i.e. die stone models, was used to prepare them from the impressions made without retraction and after retraction. To determine even the minute difference in the amount of sulcus width at the crest of gingiva among the models an optical microscope (imaging system software) was used. Change in the width of sulcus recorded with aluminum chloride-impregnated retraction cord was maximum (0.51560 ± 0.087563 mm ) . The application of expasyl paste showed results (0.456800 ± 0.145651) comparable with aluminum chloride-impregnated retraction cord and the Magic Foam Cord resulted the least change in width of sulcus (0.30080 ± 0.135121 mm) [Table 1].
Though, numerically (mean value) of aluminium chloride-impregnated retraction cord appears to be slightly better when compared with the expasyl paste [Table 2], the difference was statistically insignificant (P > 0.05). So it is inferred that the paste has got almost the same effect of retraction than that of retraction cord. Comparing the expasyl paste with the Magic Foam Cord, the sulcus enlargement was found statistically significant as the "P" value was less than 0.05 [Table 3]. It means expasyl paste provided better gingival sulcus enlargement than the Magic Foam Cord. Same result was obtained when Magic Foam Cord and aluminium chloride-impregnated retraction cord were compared. [Table 4] suggests more amount of retraction by aluminium chloride-impregnated retraction cord. The manufacturer claims that the Magic Foam Cord is an addition elastomer that becomes foamy during the addition reaction resulting in a temporary retraction of gingiva. [7],[23] Expasyl paste is a viscous paste having kaolin as one of its constituent, which holds its rigidty while creating a space between the tooth and gingiva. [24],[25],[26] Whereas the impregnated retraction cord absorbs the moisture and the cord swells, thereby mechanically displacing the gingiva. Astringent used for impregnation of the retraction cord causes hemostasis by the vasoconstriction of the blood capillaries, thereby providing dry working field. | Table 2: Comparison of change in width of the gingival sulcus caused by expasyl paste and aluminium
chloride-impregnated retraction cord
Click here to view |
 | Table 3: Comparison of change in width of the gingival sulcus caused by magic foam cord and expasyl paste
retraction system
Click here to view |
 | Table 4: Comparison of change in width of the gingival sulcus caused by magic foam cord and aluminium
chloride-impregnated retraction cord
Click here to view |
None of the materials produced scale two bleeding on removal, though the scale one was seen in few cases with all three materials but the result was statistically insignificant [Table 5]. This suggests that for any retraction procedure, if carefully done, post-retraction bleeding should not be a problem. In the literature, it was mentioned that the bleeding during retraction or after retraction could be controlled by using hemostatic agents. Moreover, bleeding mainly depends on the state of gingival tissue, so an acceptable healthy gingival tissue is a desirable requirement before the retraction. | Table 5: Evaluation of post-retraction bleeding by "Wilcoxon signed ranks test"
Click here to view |
| Discussion | | |
In accordance to the study results of Poss, removal of the retraction material revealed that retraction cord was difficult to place in comparison with other two materials but the removal was easy. [10],[15] Expasyl paste needed flushing of the material with the water jet, though it was not difficult but time consuming in drying the area before making the impression. For the Magic Foam Cord, the manufacturer approves the material to be injected into gingival sulcus and around, keeping it there for 1 ½ min and then maintaining the pressure for 5 min using putty with polyethylene spacer in the stock tray (putty technique). This caused discomfort to the patient. However, this impression is to be used for final relining. So, it cannot be compared with the discomfort/comfort level while using the impregnated retraction cord procedure or the expasyl paste procedure. The compre cap technique, also suggested by the manufacturer while using Magic Foam Cord was not included in the study as there was no preparation of the tooth.
For gingival retraction, the cords are used alone or are impregnated with chemicals. Among the chemicals, aluminium chloride is suitable because it causes minimal tissue damage in terms of inflammation, recession, and change in contour. [22],[27],[28] In a study conducted on dogs by Shaw DH and Krejci RF, no additional inflammation in gingival crevices was seen where dilute aluminium chloride (0.033%) was used compared with the concentrated solutions (60%), which caused severe inflammation and necrosis. [26] In the present study, the different concentrations of aluminium chloride were not compared for the effect on the health of the gingival tissue. The concentration taken was 6% and compared with the other technique of gingival retraction. It was noticed that the health of the gingival tissue remained optimum when examined after 8 days in all the three techniques. This was also expressed in the study of Andrew Shannon and Shaw DH who demonstrated that expasyl paste caused minimal trauma to periodontium. [29],[30],[31],[32] They did not study the Magic Foam Cord.
This study, however, reveals that all three retraction systems are reasonably acceptable as per the results, as all three provide retraction more than the minimum amount of retraction (0.22 mm) required for any fixed partial denture impressions. [20],[33],[34] Within the limited scope of the study it indicates that the use of expasyl paste and Magic Foam Cord was painless and is quick and easy. Therefore, saving chair side time. Though all the possible care was taken to standardize all aspects of the study, every patient's physiology may have differed and hence the response of the gingiva to the retraction material. The result of this study needs to be verified at a larger clinical sample size, in a variety of situations (both in anterior and posterior regions of the jaws, in both maxillary and mandibular arches, prepared tooth), on different gingival biotypes (thick and thin), variety of age groups, and in males and females. Also there is a need of histological analysis of the effect of gingival retraction materials on the soft tissue.
| Conclusion | | |
Though the maximum retraction was produced by aluminium chloride-impregnated retraction cord and even there were statistically significant difference in the width of retracted gingival sulcus among three systems except between expasyl paste and impregnated retraction cord, which was insignificant but enlargement achieved in all the three systems was more than the minimum required. Advantages with expasyl paste and Magic Foam Cord over the retraction cord were their ease of application, painless, quick, and without agony to the patient.
| References | | |
| 1. | Bowles WH, Tardy SJ, Vahadi A. Evaluation of new gingival retraction agents. J Dent Res 1991;70:1447-9. 
|
| 2. | Csempesz F, Vag J, Fazekas A. In vitro Kinetic study of absorbency of retraction cords. J Prosthet Dent 2003;89:45-9.
|
| 3. | Krishna Ch V, Gupta N, Reddy KM, Sekhar NC, Aditya V, Reddy GV. Laser gingival retraction: A quantitative assessment. J Clin Diagn Res 2013;7:1787-8.
|
| 4. | Donovan TE, Ganadra BK, Nemetz H. Review and survey of medicaments used in gingival retraction cords. J Prosthet Dent 1985;53:525-31.
|
| 5. | Forgia AL. Tissue retraction for fixed prosthesis. J Prosthet Dent 1961;11:480-6.
|
| 6. | Kellam SA, Smith JR, Scheffel SJ. Epinephrine absorption from commercial gingival retraction agents in clinical patients. J Prosthet Dent 1992;68:761-5.
|
| 7. | Loe H, Silness J. Tissue reactions to string packs used in fixed restorations. J Prosthet Dent 1963;13:318-25.
|
| 8. | Phatale S, Marawar PP, Byakod G, Lagdive SB, Kalburge JV. Effect of retraction materials on gingival health: A histopathological study. J Indian Soc Periodontol 2010;14:35-9.
[PUBMED]  |
| 9. | Nemetz EH, Seibly W. The use of chemical agents in gingival retraction. Gen Dent 1990;38:104-8.
|
| 10. | Pelzner RB, Kempler D, Stark MM, Lum LB, Nicholson RJ, Soelberg KB. Human blood pressure and pulse rate response to racemic epinephrine retraction cord. J Prosthet Dent 1978;39:287-92.
|
| 11. | Perakis N, Belser UC, Magne P. Final impressions: A review of material properties and description of a current technique. Int J Periodontics Restorative Dent 2004;24:109-17.
|
| 12. | Donovan TE, Chee WW. Current concepts in gingival displacement. Dent Clin North Am 2004;48:433-44.
|
| 13. | Meraner M. Soft tissue management for difficult cervical restorations. Gen Dent 2006;54:117-20.
|
| 14. | Baharav H, Kupershmidt I, Laufer BZ, Cardash HS. The effect of sulcular width on the linear accuracy of impression materials in the presence of an undercut. Int J Prosthodont 2004;17:585-9.
|
| 15. | Bennani V, Schwass D, Chandler N. Gingival retraction techniques for implants versus teeth: current status. J Am Dent Assoc 2008;139:1354-63.
|
| 16. | Al-Ani A, Bennani V, Chandler NP, Lyons KM, Thomson WM. New Zealand dentists' use of gingival retraction techniques for fixed prosthodontics and implants. N Z Dent J 2010;106:92-6.
|
| 17. | Shillingburg HT, Hobo S, Whitsett LD. Fundamentals of fixed prosthodontics. In: Shillingburg HT, Hobo S, Whitsett LD, editors. Fundamentals of Fixed Prosthodontics. Chicago: Quintessence; 1997. p. 260-76.
|
| 18. | Al Hamad KQ, Azar WZ, Alwaeli HA, Said KN. A clinical study on the effects of cordless and conventional retraction techniques on the gingival and periodontal health. J Clin Periodontol 2008;35:1053-8.
|
| 19. | Kazemi M, Memarian M, Loran V. Comparing the effectiveness of two gingival retraction procedures on gingival recession and tissue displacement: Clinical study. Res J Biol Sci 2009;4:335-9.
|
| 20. | Shivasakthy M, Asharaf Ali S. Comparative study on the efficacy of gingival retraction using polyvinyl acetate strips and conventional retraction cord - An in vivo study. J Clin Diagn Res 2013;7:2368-71.
|
| 21. | Gupta A, Prithviraj DR, Gupta D, Shruti DP. Clinical evaluation of three new gingival retraction systems: A research report. J Indian Prosthodont Soc 2013;13:36-42.
|
| 22. | Shannon A. Expanded clinical uses of a novel tissue retraction material. Compend Contin Educ Dent 2002;23:3-6.
|
| 23. | Ruel J, Schuessler PJ, Malament K, Mori D. Effect of retraction procedures on the periodontium in humans. J Prosthet Dent 1980;44:508-15.
|
| 24. | Azzi R, Tsao TF, Carranza FA Jr, Kenney EB. Comparative study of gingival retraction methods. J Prosthet Dent 1983;50:561-5.
|
| 25. | Reiman MB. Exposure of subgingival margins by Nonsurgical gingival displacement. J Prosthet Dent 1976;36:649-54.
|
| 26. | Runyan DA, Reddy TG Jr, Shimoda LM. Fluid absorbency of retraction cords after soaking in aluminum chloride solution. J Prosthet Dent 1988;60:676-8.
|
| 27. | Shaw DH, Krejci RF, Cohen DM. Retraction cords with aluminum chloride: Effect on the gingiva. Oper Dent 1980;5:138-41.
|
| 28. | Shaw DH, Krejci RF. Gingival retraction preference of dentists in general practice. Quintessence Int 1986;17:277-80.
|
| 29. | Tupec RG, Neacy K. A comparison of cord gingival displacement with the gingitage technique. J Prosthet Dent 1981;46:509-15.
|
| 30. | Weir DJ, Williams BJ. Clinical effectiveness of mechanical- chemical tissue displacement methods. J Prosthet Dent 1984;51:326-9.
|
| 31. | Rupali K, Sarandha DL, Chand BD. Advances in gingival retraction. IJCDS 2011;2:64-7.
|
| 32. | Ateeq MP, Soorya PT, Kashinatha HM, Muralidhara G. Conventional and new techniques in gingival displacement. J Dent Oral Biosci 2011;2:33-7.
|
| 33. | Beier US, Kranewitter R, Dumfahrt H. Quality of impressions after use of the magic foamcord gingival retraction system- A clinical study of 269 abutment teeth. Int J Prosthodont 2009;22:143-7.
|
| 34. | Mechanic E. Gingival retraction using paste systems. Available from: http://www.oralhealthgroup.com/news/gingival-retraction-using-paste-systems/1002122009/? and er=NA [Last cited on 2013 Jan 10].
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|















 Search Pubmed for
Search Pubmed for