|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 51-55 |
|
Multidisciplinary approach in rehabilitating flabby ridge in completely edentulous patient
Poonam K Khinnavar, BH Dhanya Kumar, HR Shivakumar, DB Nandeeshwar
Department of Prosthodontics, Bapuji Dental College and Hospital, Davangere, Karnataka, India
| Date of Web Publication | 29-May-2015 |
Correspondence Address:
Dr. Poonam K Khinnavar
Bapuji Dental College and Hospital, Davangere, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.157844

Hypermobile ridges or flabby edentulous ridges are a common occurrence. The mucostatic or minimally displacive impression technique is one of the treatment options in this scenario. Conventional mucostatic methods like employing a window tray technique, double spacers, multiple relief holes, can be utilized. Even the manual placement and manipulation of a custom tray may distort the tissues. This may violate the principles of mucostatic impression technique. Flabby ridges can be managed surgically by excision, ridge augmentation, injection of sclerosing solutions and also by implant retained prosthesis. Proper recording of these hypermobile tissues and stable occlusal contacts can help to manage flabby tissues to certain extent. This case report is about surgical and prosthodontic approach for management of a maxillary flabby edentulous ridge with the aid of a minimally displacive impression technique. Keywords: Bioglass, flabby ridge, impression, minimal clinically important differences analysis, platelet-rich plasma, retention
How to cite this article:
Khinnavar PK, Dhanya Kumar B H, Shivakumar H R, Nandeeshwar D B. Multidisciplinary approach in rehabilitating flabby ridge in completely edentulous patient. Eur J Prosthodont 2015;3:51-5 |
How to cite this URL:
Khinnavar PK, Dhanya Kumar B H, Shivakumar H R, Nandeeshwar D B. Multidisciplinary approach in rehabilitating flabby ridge in completely edentulous patient. Eur J Prosthodont [serial online] 2015 [cited 2018 Aug 27];3:51-5. Available from: http://www.eurjprosthodont.org/text.asp?2015/3/2/51/157844 |
| Introduction | |  |
The glossary of prosthodontic terms defines flabby ridge as excessive movable tissue. [1] Poor stability and support are the drawbacks of excessively moving tissue for the complete denture. [2] A complete radiographic survey, visual and digital examination, and a notation of the patient's denture history are the requisites for preliminary mouth examination. [3]
As proposed by Desjardin and Tolman, various etiological agents for the development of flabby ridge are atrophy, bone resorption, nutritional deficiencies, pressure, functional forces and patients with parafunctional habits. [4] Retention, stability, and support are adversely affected in such cases. [5] Flabby ridges can be managed surgically by excision, ridge augmentation, injection of sclerosing solutions [4] and also by implant retained prosthesis. Proper recording of these hypermobile tissues and stable occlusal contacts can help to manage flabby tissues to certain extent. [6] This case report deals with the surgical approach followed by prosthodontic management of a maxillary flabby edentulous ridge with the aid of a mucostatic impression technique.
| Case Report | | |
A 73-year-old male patient reported to the Department of Prosthodontics, Bapuji Dental College and Hospital, Davangere, Karnataka, India, seeking new complete dentures due to the worn out existing dentures. The previous set of denture was made 10 years back, and the patient had a history of continuous denture use without allowing tissue rest even at night.
Clinical examination
Intraoral examination revealed maxillary and mandibular completely edentulous ridges, with flabby tissue in the anterior ridge area extending from canine to canine region in premaxilla with varying degrees of displaceability and severely resorbed mandibular ridge.
Treatment plan
The following treatment plan was formulated for the patient:
- Management of flabby ridge, with:
- surgical [2] followed by
- prosthodontic approach. [6]
Surgical management by ridge augmentation with graft material was opted for this particular patient as
- patient's general health and motivation level were in favor [6],[7]
- sufficient bone height in posterior maxilla as a guide for grafting [4],[8]
- additional surgery for graft harvesting was not required as allogenous graft material was used. [4],[8]
Treatment procedure
Surgical
Patient's whole blood (that was anticoagulated with citrate dextrose) was collected in 4 tubes before undergoing two stages of centrifugation (TruPRP, TruPlateletRichPlasma) (Harvest) designed to separate the platelet-rich plasma (PRP) aliquot from platelet-poor plasma and red blood cells. [9],[10],[11],[12]
Surgical procedure
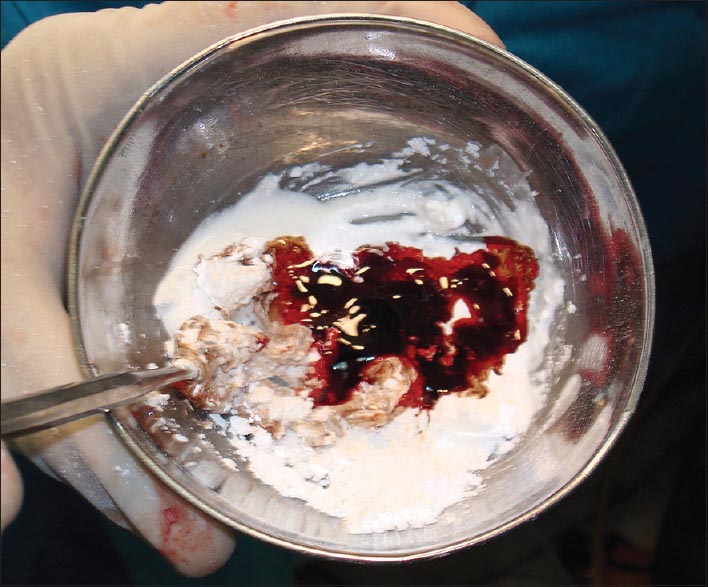
Bioglass
One of the biggest hurdles in tissue engineering was to mimic the extracellular matrix. Studies comparing bioinert with bioactive glass ceramic templates produced increased osteoblast proliferation and differentiation. This system helped osteoblasts to adhere, migrate, proliferate, and mineralize into bone, in the bone defect filling [13] [Figure 1].
Platelet-rich plasma
Platelet-rich plasma is blood plasma that has been enriched with platelets. As a concentrated source of autologous platelets, PRP contains (and releases through degranulation) several different growth factors and other cytokines that stimulate healing of bone and soft tissue [9],[10],[11],[12] [Figure 1].
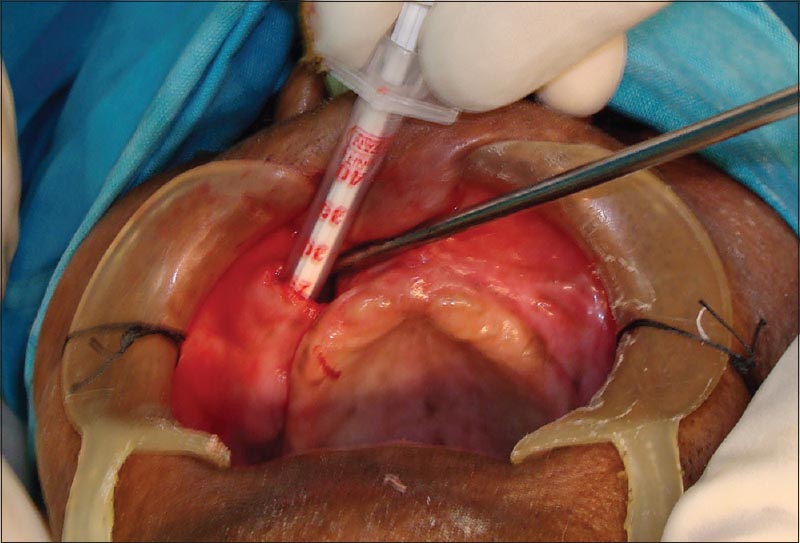
In this case, adequate local anesthesia of anterior maxillary area was achieved, and the canine eminence on either side was identified. Two vertical intraoral incisions were taken just above the attached gingiva from one maxillary buttress to the other. Supra periosteal dissection was performed to create two pockets on either side of the piriform aperture [Figure 2]. The dissection was extended to the muscular attachment level, continuing in the midline by a tunneling effect, extending superiorly up to the base of the piriform aperture taking care not to peforate the nasal cavity. A mixture of platelet rich plasma and bioglass was then filled in this tunnel and was closed with vicryl sutures. [14],[15] Suture removal was done after 2 weeks of surgery.
Patient was reviewed after about 3 months postsurgery, the findings were as follows:
Radiographic findings
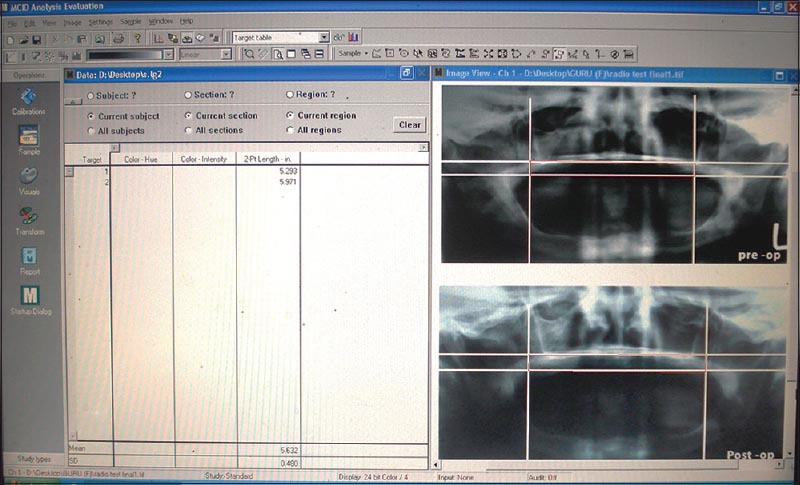
Orthopantomogram (OPG) findings showed increased radio-opacity when compared with the presurgical OPG.
Minimal clinically important differences analysis
Constitute valuable assets in Imaging Research. The figure shows preop and postop length of the radio-opaque density of bone [Figure 3].
Clinical finding
The displacibility of the mucosa was reduced up to 75% in premaxilla.
Though it is not advisable to deliver prosthesis to the patient at least until 3-4 months postsurgery, [14] patient being very particular about his esthetics, we planned to fabricate an interim complete denture prosthesis. Patient was instructed not to wear the denture for functional purpose [eating]. The denture was relined with the chair-side soft liner [GC Liner] to avoid undue pressure on the surgical area. Care was taken to change the soft liner every 8-10 days.
Prosthodontic management
- A diagnostic impression of both the arches was made with low viscosity irreversible hydrocolloid (zelgan, dentsply/caulk) to ensure minimal distortion of the flabby tissue and the primary cast was poured with type II gypsum product
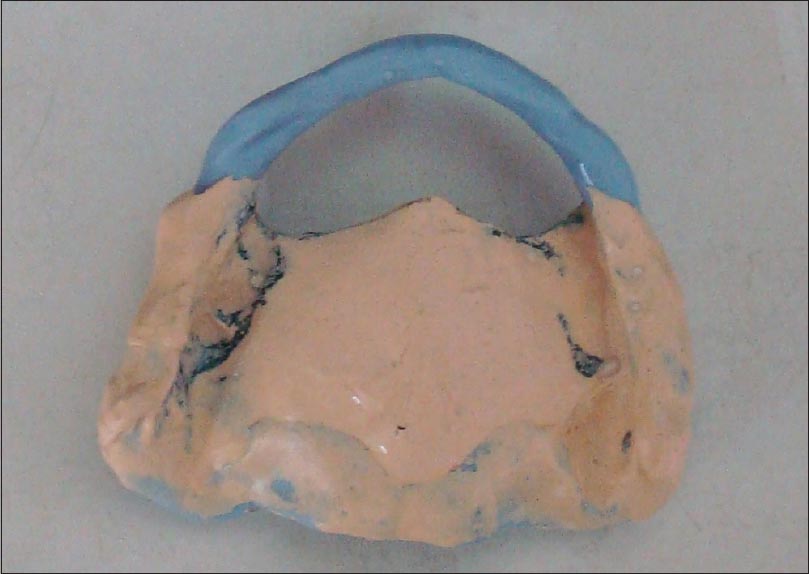
- Flabby ridge area was marked on the cast, special tray was fabriacated providing a window in the area of flabby ridge, providing proper spacer and stops with autopolymerizing resin (M.P.Sai)
- A suitable adhesive was applied on the borders of the tray and single step border molding was done using heavy bodied addition-curing polyvinylsiloxane impression material (Extrude® polyvinylsiloxane impression material; Kerr,) [Figure 4]
- After completion of border molding, the area of the custom tray other than the "flabby" tissues was filled with zinc oxide eugenol impression paste and the wash impression of the normal tissues was made [Figure 4]
- Excess material from the periphery as well as over the window opening was trimmed away
- Impression tray was placed back in the patient's mouth, and impression plaster was applied on the flabby ridge, exposed through the window [Figure 5]
 | Figure 5: Final impression of anterior flabby ridge recorded with impression plaster
Click here to view |
- Impression was removed carefully. Separating medium was applied to the impression plaster area and cast was poured. In this technique, the flabby ridge was recorded in minimally displaced form and rest of the tissue in functional form.
Denture fabrication was then continued in the usual manner. Following face-bow transfer, arrangement of the teeth was done on a semi-adjustable articulator, achieving balanced articulation and paying attention to even tooth contact in excursive movements. The dentures were delivered. Patient expressed satisfaction with stability and aesthetics at subsequent recall appointments.
| Discussion | | |
There are surgical as well as prosthetic treatment options to manage the flabby tissues with its own advantages and disadvantages. Nowadays surgical excision is mainly a historical concept. [4] This procedure results in a shallow ridge with little or no retention and resistance to the lateral forces. [5] Ridge augmentation with autogenous or allogenous graft is another option, which has disadvantages like resorption up to 50% and migration of the graft. [4] Next option would be injection of sclerosing solutions, drawbacks being anaphylactic reactions, patient discomfort and technique sensitivity. So surgical treatment is suitable only when age, general health, dental history, motivation, and personality are in favor. [4] In this particular case report, everything was favorable for the surgery and second surgery was not needed since alloplastic graft material was planned to use. [10]
A muco-displacive impression technique exhibits excellent retention of the denture during the function, reason being displacement of vascular contents of the blood vessels into the interstitial spaces. But when at rest, retention and stability are affected, and the denture becomes loose because blood re-enters the tissues altering its contours. [2],[4],[16],[17],[18],[19],[20],[21] According to the theories of impression making, muco-displacive impression techniques results in an unretentive and unstable denture. Selective pressure or minimally displacive impression techniques overcome these limitations. The use of relief holes, windows and wax relief reduces the hydraulic pressure and minimizes the displacement of the stress bearing tissues. "Pressure" is the only principle on which the ideas of impression making are based, especially for hypermobile tissues. [6]
It is impossible to register flabby tissue in an unstrained position, as mere introduction of trays and amount of force applied result in tissue displaceability. [9],[16],[19] In this case, mucostatic technique enabled a satisfactory recording of generalized ridge hyperplasia, avoiding overcompression.
The choice of impression techniques depends on the personal preference based on the principles of impression making. [4]
Two main impression techniques reported are:
- Mucodisplacive, in which the tissues are compressed
- Mucostatic in which tissues are recorded in their rest position. [7]
No technique is superior over the other.
In this particular case, we preferred a mucostatic impression technique using windowed tray. Usually, the prosthesis is delivered after 6 months of surgery. Since the patient was very keen about the esthetics, we had to plan for the prosthesis after 2½ months of surgery. Opinion from the oral surgeons was taken regarding the stability of the graft, and the prosthetic management was started.
| Conclusion | | |
This case report has described the management of hyperplastic tissues using both surgical and prosthodontic approach.
Surgical removal of flabby tissues has become obsolete now with its own merits and demerits.
This case was a suitable candidate for ridge augmentation, since age, dental health; general health and personality were all in favor. Allogenous graft material mixed with patient's own blood PRP was used which avoided additional surgery for graft harvesting. minimal clinically important differences analysis showed increased length and density of the bone following surgery. Mucosal displacibility was reduced up to 75% in premaxilla.
Patient was satisfied and happy with the procedure.
Patient is kept under periodic review for the follow-up.
| References | | |
| 1. | The glossary of prosthodontic terms. J Prosthet Dent 2005;94:10-92.  |
| 2. | MacEntee MI. Identifying the Problem. The Complete Denture. A Clinical Pathway. Chicago: Quintessence; 1996. p. 1-7. |
| 3. | Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: A mixed-longitudinal study covering 25 years. J Prosthet Dent 1972;27:120-32. [ PUBMED] |
| 4. | Desjardins RP, Tolman DE. Etiology and management of hypermobile mucosa overlying the residual alveolar ridge. J Prosthet Dent 1974;32:619-38. [ PUBMED] |
| 5. | Lynch CD, Allen PF. Management of the flabby ridge: Using contemporary materials to solve an old problem. Br Dent J 2006;200:258-61. |
| 6. | Bindhoo YA, Thirumurthy VR, Kurien A. Complete mucostatic impression: A new attempt. J Prosthodont 2012;21:209-14. |
| 7. | Crawford RW, Walmsley AD. A review of prosthodontic management of fibrous ridges. Br Dent J 2005;199:715-9. |
| 8. | Starshak T, Sanders B. Preprosthetic Oral and Maxillofacial Surgery. St. Louis, MO: Mosby; 1980. p. 165-213. |
| 9. | Aghaloo TL, Moy PK, Freymiller EG. Investigation of platelet-rich plasma in rabbit cranial defects: A pilot study. J Oral Maxillofac Surg 2002;60:1176-81. |
| 10. | Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:638-46. |
| 11. | Schmitz JP, Hollinger JO. The biology of platelet-rich plasma. J Oral Maxillofac Surg 2001;59:1119-21. [ PUBMED] |
| 12. | Fennis JP, Stoelinga PJ, Jansen JA. Mandibular reconstruction: A clinical and radiographic animal study on the use of autogenous scaffolds and platelet-rich plasma. Int J Oral Maxillofac Surg 2002;31:281-6. |
| 13. | Maiorana C, Sommariva L, Brivio P, Sigurtà D, Santoro F. Maxillary sinus augmentation with anorganic bovine bone (Bio-Oss) and autologous platelet-rich plasma: Preliminary clinical and histologic evaluations. Int J Periodontics Restorative Dent 2003;23:227-35. |
| 14. | Wessberg GA, Schendel SA, Epker BN. Modified maxillary submucosal vestibuloplasty. Int J Oral Surg 1980;9:74-8. [ PUBMED] |
| 15. | Bartee BK. The use of high-density polytetrafluoroethylene membrane to treat osseous defects: Clinical reports. Implant Dent 1995;4:21-6. |
| 16. | Devan MM. Basic principles of impression making. J Prosthet Dent 1952;2:26-35. |
| 17. | Appleby RC. Mandibular impression technique for displaceable tissues. J Prosthet Dent 1954;4:335-45. |
| 18. | Porter CG. Mucostatics - Panacea or propaganda. J Prosthet Dent 1953;3:464-6. |
| 19. | Collette HA. Complete denture impressions. J Prosthet Dent 1965;15:603-14. |
| 20. | Klein IE, Broner AS. Complete denture secondary impression technique to minimize distortion of ridge and border tissues. J Prosthet Dent 1985;54:660-4. [ PUBMED] |
| 21. | McCord JF, Grant AA. Impression making. Br Dent J 2000;188:484-92. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|









 Search Pubmed for
Search Pubmed for