|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 77-79 |
|
Management of myofacial pain with liquid oral splint
Anish Amin, Roseline Meshramkar, K Lekha
Department of Prosthodontics, SDM College of Dental Sciences and Hospital, Sattur, Dharwad, Karnataka, India
| Date of Web Publication | 29-Sep-2015 |
Correspondence Address:
Dr. Anish Amin
Post Graduate Student, Department of Prosthodontics, SDM College of Dental Sciences and Hospital, Sattur, Dharwad - 580009, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.166183

Occlusal splint therapy has been one of the conventional modalities of the management of temporomandibular disorders. However, it is important for a clinician to make an evidence.based decision on choosing the appropriate type of splint. Currently, the much-discussed one is the liquid supported the occlusal splints. A 19-year-old girl diagnosed with myofacial pain, presented with a chief complaint of the history of pain and headache which is severe early in the morning and continuous throughout the day since 1-month, also associated with the tenderness of masticatory muscles and attrition of the lower anterior teeth. The patient was provided with a liquid occlusal splint for a period of 3 months with check.up recalls at predefined intervals. Post the liquid occlusal splint therapy, the patient showed a significant decrease in both subjective and objective pain. Keywords: Liquid splint, myofacial pain, temporomandibular joint
How to cite this article:
Amin A, Meshramkar R, Lekha K. Management of myofacial pain with liquid oral splint. Eur J Prosthodont 2015;3:77-9 |
| Introduction | |  |
The American Dental Association President's Conference on temporomandibular disorders (TMD) (1983) defined as a group of orofacial disorders characterized by pain in the preauricular area, temporomandibular joint (TMJ), or muscles of mastication, limitations and deviations in the mandibular range of motion, and TMJ sounds during jaw function.[1]
The reasons for this may be parafunctional habits, stress, or abnormalities of the TMJ. Abnormal dental occlusion appears to be equally common in persons with and without TMJ symptoms.[2],[3] The purpose of choosing the liquid supported splints in this patient is that these are readily available, relatively simple, and noninvasive.[4]
| Case Report | | |
A 19-year-old female reported to the Department of Maxillofacial Prosthodontics, in our institution, with pain on both sides of the mandibular jaw. The patient gave the history of pain and headache which is severe early in the morning and continuous throughout the day since 1 month. On extraoral and intraoral examination, positive findings such as the tenderness of masseter muscle on both sides upon palpation, attrition on the lower anterior teeth, and repetitive subconscious clenching of teeth by the patient was noticed. The radiographic examination did not reveal the presence of any dental infections or TMJ deformities.
After ruling out, previous family and medical history of any suspected TMJ disorder such as inflammatory TMJ, deformity of articular disc, derangement of condyle, etc., the case was diagnosed as masticatory muscle disorder presenting with myospasm and myofacial pain due to the parafunctional habit of constantly clenching her teeth attributed to her studies related stress.
A treatment plan was formulated, and a liquid occlusal splint was advised to meet the need of the patient for decreasing the hyperactivity of masticatory muscles. The concept of the liquid oral splint is that, it automatically eliminates the distorting influence of the occlusion on the functional position of the jaw, harmonizing muscles, bite, and body. The simple insertion of the liquid splint creates a muscle-dominant functionally generated occlusion instantly.[5]
The therapeutic protocol was explained in detail to the patient, and an informed consent was obtained prior to the starting of treatment. A prefabricated liquid occlusal splint (Aqualizer ™, BVM Meditech Pvt. Ltd., New Delhi, India) was inserted, and the post insertion instructions were given [Figure 1].
The patient was scheduled for follow-up visits. The recommended protocol after insertion of the splint is that the patient needed to visit the prosthodontist for adjustments at 24 h, 7 days, 1 month, and 3 months intervals.
The follow-up visits revealed that the total satisfactory results with reduced subjective (MOD-SSI = modified-symptom severity index scores) and objective (digital palpation) pain [6] in the patient. The electromyographic examination of the masticatory muscles before and after liquid splint therapy at rest position and maximum voluntary clenching depicted marked decrease in muscle activity after the splint usage, which indicates that there was an improved balance in the muscular activity after the therapy [Figure 2]a and [Figure 2]b.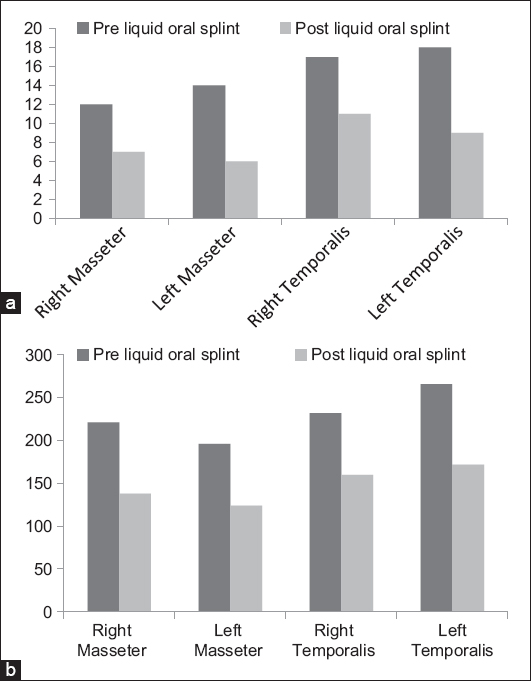 | Figure 2: (a) Electromyographic values of masticatory muscles at rest before and after insertion of liquid oral splints: At rest ( µV) (b) Electromyographic values of masticatory muscles at maximum voluntary clenching before and after insertion of liquid oral splint: At maximum voluntary clenching ( µV)
Click here to view |
| Discussion | | |
According to the Glossary of Prosthodontic Terms (8th ed.), "Occlusal splint is defined as any removable artificial occlusal surface used for diagnosis or therapy affecting the relationship of the mandible to the maxilla. It may be used for occlusal stabilization, for the treatment of TMD, or to prevent wear of the dentition." A common goal of occlusal splint treatment is to protect the TMJ discs from dysfunctional forces that may lead to perforations or permanent displacements. Other goals of the treatment are to improve jaw-muscle function and to relieve associated pain by creating a stable balanced occlusion.[7]
Currently, most of the occlusal splints in use are either the hard or soft splints. Hard splints have an advantage of having a hard occluding surface that does not lose its fit and hence lasts longer. Soft splints are simple to fabricate and are more easily adjusted to adequate contact pattern due to the softness of the occlusal surface.[8] Hard splints can sometimes cause significant occlusal changes which are undesirable.[7] Soft splints can exacerbate bruxism,[9] may be due to premature posterior contacts related to the fact that these splints cannot be balanced.
In the present case report, a prefabricated liquid occlusal splint was inserted into patient's oral cavity. It has a flexible fluid layer that equalizes all bite forces by preventing the tooth to tooth contact, optimizes biomechanics, supports the jaw in a comfortable position, removes the teeth from dominance, placing bite and body in harmony, straightens the bite to maximize other structures, enables the systemic function and balance, and allows the body to naturally balance itself.[10] This occurs because the liquid splint facilitates the muscle dominated mandibular repositioning while it equalizes, axializes, balances, distributes, and makes simultaneous all occlusal forces. Despite the various studies and clinical reports, there is still a certain controversy as to which type of the splint is more effective in managing patients with myofacial pain. Evidence-based decisions should always be made while choosing the appropriate splint therapy for a particular patient.[10]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Al-Riyami S. Temporomandibular Joint Disorders in Patients with Skeletal Discrepancies. PhD Thesis. London: UCL Eastman Dental Institute for Oral Health Sciences; 2010. Available from: http://www.discovery.ucl.ac.uk/575469/1/575469.pdf. [Last cited on 2012 Jun 20].  |
| 2. | Dworkin SF, Huggins KH, LeResche L, Von Korff M, Howard J, Truelove E, et al. Epidemiology of signs and symptoms in temporomandibular disorders: Clinical signs in cases and controls. J Am Dent Assoc 1990;120:273-81. |
| 3. | McNamara JA Jr, Seligman DA, Okeson JP. Occlusion, Orthodontic treatment, and temporomandibular disorders: A review. J Orofac Pain 1995;9:73-90. |
| 4. | Okeson JP. Management of Temporomandibular Disorders and Occlusion. 5 th ed. St. Louis (MO): Mosby; 2003. p. 500. |
| 5. | Srivastava R, Jyoti B, Devi P. Oral splint for temporomandibular joint disorders with revolutionary fluid system. Dent Res J (Isfahan) 2013;10:307-13. |
| 6. | Alencar F Jr, Becker A. Evaluation of different occlusal splints and counselling in the management of myofascial pain dysfunction. J Oral Rehabil 2009;36:79-85. |
| 7. | Yadav S, Karani JT. The essentials of occlusal splint therapy. Int J Prosthet Dent 2011;2:12-21. |
| 8. | Krogh-Poulsen W. Treatment of oro-mandibular dysfunction by means of occlusal splints. Scanodont 1981;1:5-13. |
| 9. | Okeson JP. The effects of hard and soft occlusal splints on nocturnal bruxism. J Am Dent Assoc 1987;114:788-91. |
| 10. | The Revolutionary Aqualizer Self-Adjusting Oral Splint. New Harmony Between Bite and body: TMJ Pain Relief and Treatment with Aqualizer ® Dental Splints. Available from: http://www.aqualizer.com/html/aqualizer.html. [Last accessed on 2013 Feb 17]. |
[Figure 1], [Figure 2]
|










 Search Pubmed for
Search Pubmed for