|
 
 |
|
BRIEF REPORT |
|
|
|
| Year : 2011 | Volume
: 17
| Issue : 2 | Page : 90-93 |
| |
G-C heterozygosis in mutS homolog2 as a risk factor to hereditary nonpolyposis colon cancer in the absence of a family medical history
Jorge Alfonso Arvayo-Zatarain, José Manuel Grijalva-Chon, Reina Castro-Longoria, Alejandro Varela-Romero
Departamento de Investigaciones Científicas y Tecnológicas, Universidad de Sonora, Ave. Colosio s/n, entre Sahuaripa y Reforma, Hermosillo, Sonora 83000, Mexico
| Date of Web Publication | 17-Oct-2011 |
Correspondence Address:
José Manuel Grijalva-Chon
Universidad de Sonora - DICT Ave. Colosio s/n, entre Sahuaripa y Reforma, Hermosillo
Mexico
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.86191

 Abstract Abstract | | |
To detect the presence of point mutations in a small section of the mutS homolog2 (MSH2) gene in both healthy and affected persons treated at the General Hospital of the State of Sonora, a 353 base pair section of the MSH2 gene was amplified and sequenced from six persons affected by hereditary nonpolyposis colorectal cancer and from 19 healthy persons. The affected persons did not show the mutations reported in the scientific literature; however, six healthy persons were heterozygote and mutant-allele carriers. The heterozygote condition implies that carriers are candidates for the development of colorectal cancer. However, it is important to know the family medical history when investigating hereditary mutations.
Keywords: Colorectal cancer, hereditary nonpolyposis colon cancer, mutS homolog 2 gene, point mutation
How to cite this article:
Arvayo-Zatarain JA, Grijalva-Chon JM, Castro-Longoria R, Varela-Romero A. G-C heterozygosis in mutS homolog2 as a risk factor to hereditary nonpolyposis colon cancer in the absence of a family medical history. Indian J Hum Genet 2011;17:90-3 |
How to cite this URL:
Arvayo-Zatarain JA, Grijalva-Chon JM, Castro-Longoria R, Varela-Romero A. G-C heterozygosis in mutS homolog2 as a risk factor to hereditary nonpolyposis colon cancer in the absence of a family medical history. Indian J Hum Genet [serial online] 2011 [cited 2016 May 13];17:90-3. Available from: http://www.ijhg.com/text.asp?2011/17/2/90/86191 |
| Introduction | |  |
Modern biomedical research has reached great advances in the knowledge of the genetic mechanisms involved in the major illnesses, in the improvement of treatments, and consequently in the primary healthcare. For hereditary nonpolyposis colon cancer (HNPCC), the advance involves the knowledge of the responsible genes, named MSH1, MSH2, MSH3, MSH6, PMS1, and PMS2.[1],[2],[3],[4] Our present treatments do not allow us to win the battle at the most advanced stages, but the information generated has contributed to the understanding of the cellular processes and to develop good detection methods to be able to use more efficient therapy. However, healthy people are unaware of the possibility for them to be carriers of genes that predispose them to colorectal cancer, independent of the family background.
According to Fishel et al., [1] HNPCC patients have a microsatellite instability caused by a transition mutation in an mutS homolog 2 (MSH2) intron, in the 2020 position of the cDNA, in which healthy persons have an adenine and the affected persons have a guanine. Recently, Medina-Arana et al. [5] reported another point mutation in MSH2 also responsible for microsatellital instability in HNPCC patients and located 63 base pairs upstream of the Fishel et al. [1] mutation. This new mutation is the replacement of an adenine by a cytosine. Epigenetic factors such as hypermethylation are also believed to be responsible for genetic instabilities that cause colorectal cancer. [6]
Because of the absence of molecular studies that give an idea of the relationship among the DNA modifications and the incidence of HNPCC in the Mexican population, it is necessary to generate knowledge of this. The scarce Mexican statistical information is limited to global and generic figures, which are the reason a pilot study at a molecular level can start a basic research line to investigate the relationship among the kind of diagnosis of colorectal cancer (polyposis or nonpolyposis) with the presence of point mutations in the most important gene responsible for HNPCC.
A routine medical diagnosis does not use molecular tools to allow patients to know their condition or predisposition to develop colorectal cancer. Our objective was to develop a pilot study to determine the presence of allelic variants (point mutations) in a small fraction of the MSH2 gene in healthy persons and in HNPCC-affected persons treated at a public hospital in northwest Mexico.
| Materials and Methods | | |
Over 10 months (August 2008 to June 2009), only six persons were treated at the Hospital General del Estado de Sonora (HGES) with a positive diagnosis for HNPCC. A tissue sample of a colon tumor was obtained from a biopsy of five patients and one from an autopsy of a patient who died 2 days before this research were begun. A blood sample was obtained from only three patients. To corroborate the presence of a mutant allele in healthy people, blood samples were taken from 17 unrelated persons.
Because HNPCC is a hereditary illness, we believed it important to include close relatives, but it was not possible to obtain a complete family history because of refusal or contact difficulties. It was only possible to obtain blood samples from the daughters of two patients. In total, the survey included 25 persons; six affected, two healthy daughters, and 17 healthy unrelated persons. The samples were analyzed to determine the presence of a transition mutation of A to G [1] or the transversion mutation of A to C. [5] All participants in the survey give their informed consent and the protocol of the survey was approved by the Ethics Committee of the Department of Medicine and Health Sciences of the University of Sonora.
DNA from tissue and blood samples was extracted with the QIAamp DNA minikit and DNA blood minikit (QIAgen, Hilden, Germany) following the manufacturer's instructions. The DNA purity and quantification were determined with a UV spectrophotometer Ultrospec 3300pro.
The polymerase chain reactions (PCR) were done using the puReTaq Ready-to-Go PCR beads (GE Healthcare, Little Chalfont, UK) in 25 μl final volume. A 353-base pair fragment of the MSH2 gene that may contain the two reported mutations related to HNPCC [1],[5] was amplified with primers 16324: 5'-CGCGATTAATCATCAGTG-3' and 16340: 5'-GGACAGAGACATACATTTCTATC-3'. [1] The reactions were done with 0.05 μg of DNA and 5 pmol of each primer following the PCR conditions reported by Fishel et al. [1]
The PCR products were visualized in 2% agarose gels with TAE buffer, stained with ethidium bromide, and were sequenced by Macrogen (Seoul, Korea). Sequence ambiguities were resolved with Chromas Pro ver 1.41. A BLAST analysis at GenBank corroborated the identity of the sequences.
| Results | | |
All the PCR reactions successfully amplified the expected amplicon of 353 base pairs. The BLAST analysis shows concordance with three sequences of the MSH2 located at chromosome 2 of Homo sapiens and 100% identity with NM_000251 and NT_022184, and 99% with NW_001838769. Six healthy persons (three men and three women) have a dual guanine-adenine signal at position 260 [Figure 1], which indicates those persons are heterozygotes for the mutations reported by Fishel et al. [1] This incidence is 31% of the healthy persons analyzed [Figure 2] with ages from 21 to 50 years. Fifty percent of those heterozygotes have a family medical history of cancer. None of the 25 persons analyzed were heterozygotes for the point mutation reported by Medina-Arana et al. [5]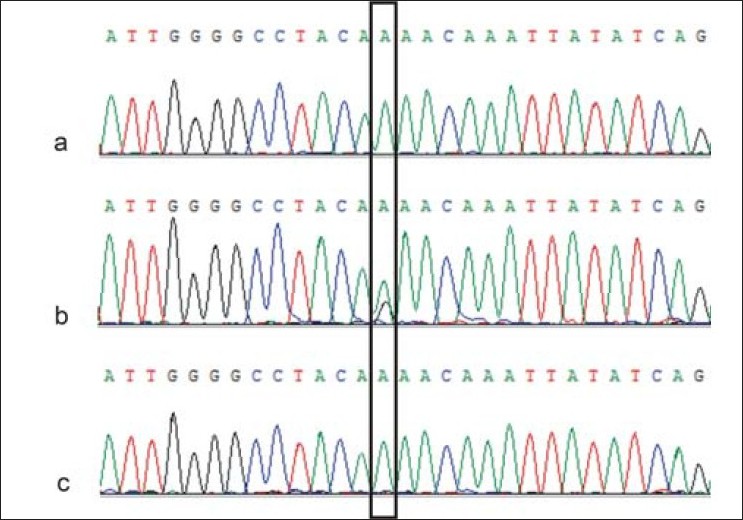 | Figure 1: Examples of the sequences obtained around the transition mutational site (rectangle). (a) Affected person without mutation. (b) Healthy heterozygote person. (c) Healthy person without mutation
Click here to view |
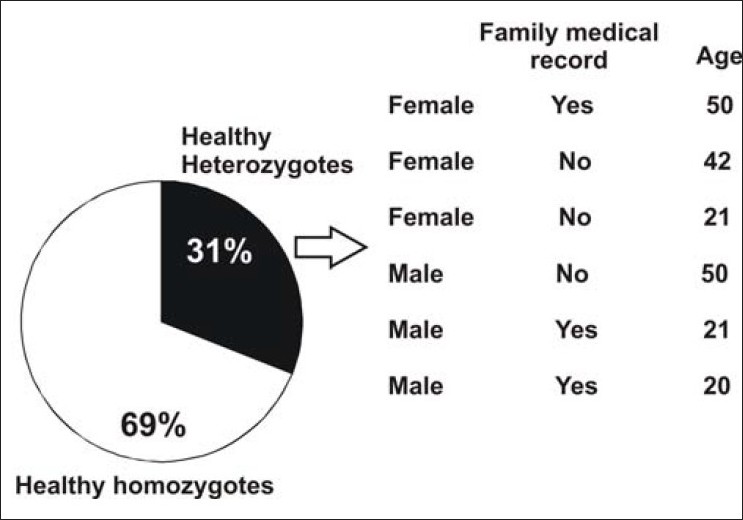 | Figure 2: Percentage of healthy persons and their genetic condition related to the transition mutational site. Data on gender, family medical record, and age
Click here to view |
| Discussion | | |
Because mutations in the MSH2 are responsible at least for a third of the HNPCC cases, [3] we expected to find some affected patients with the reported mutations [1],[5] but they had the healthy version of the gene in both tissue and blood samples. This absence of mutations in the affected patients could be explained by mutations in the other implicated genes in HNPCC (MSH1, MSH6, PMS1 and PMS2) not analyzed in this study. According to the GenBank sequence NM_000251, the codifying region of MSH2 has 3,145 nucleotides distributed in 16 exons. Of the 353 nucleotides analyzed, 204 are located in the exon 13, which is only 6.5% of the codifying region of the MSH2. In addition, the 149 nucleotides of our sequences that are partial segments of the two flanking introns of exon 13 are probably a small portion of the noncoding region in which other mutations related to colon cancer can occur, which is why we can understand the absence of mutations in the 353-nucleotides analyzed from the affected patients.
When a person is a heterozygote, as found in this study, it means that one of the parents inherited the mutant allele. Median-Arana et al. [5] mentioned that if a heterozygote person develops a cancer tumor, the tumor cells are homozygotes and as the tumor develops the proportion of heterozygote cells will drop. An important aspect is that mutations responsible for HNPCC are dominant and had 70%-90% of penetrance. [5] That means that a healthy heterozygote person has a 10%-30% probability to not develop the illness. If people know their genetic condition in advance, they will have the opportunity to get medical advice and monitoring early and pay special attention to the first abnormal symptoms.
Three healthy heterozygotes had a family medical history of colon cancer, which can explain their genetic condition. The other three heterozygotes have no relatives with colon cancer or another associated cancer. However, because of the small sample size we need to include more individuals that meet the Amsterdam II criteria to forcefully validate the possibility of an early diagnosis through a DNA-sequence analysis from blood cells. If the healthy heterozygote persons analyzed do not belong to the small group of persons that will never develop the illness (according to the penetrance of the mutation) then the illness will start at an early mature age.
The availability of the molecular methods makes it possible to prove that persons with apparent good health and without affected relatives can be carriers of a mutant allele. This highlights the need to make a more ambitious survey that includes more people and all the known genes implicated in HNPCC, with a special effort to cover more gene areas. The present gene-sequencing methods are reliable and relatively economic. They could be the basis of new noninvasive procedure for routine diagnosis once the necessary validation is achieved.
| References | | |
| 1. | Fishel R, Lescoe MK, Rao MR, Copeland NG, Jenkins NA, Garber J, et al. The human mutator gene homolog MSH2 and its associaciation with hereditary nonpolyposis cancer. Cell 1993;75:1027-38. 
[PUBMED] [FULLTEXT] |
| 2. | Strachan T, Read AP. Genética humana. 3 rd ed. México City: McGraw-Hill Interamericana; 2006. p. 501.
|
| 3. | Philip HG, Nivatvongs S. Neoplasms of the colon, rectum and anus. 2 nd ed. New York: Informa Healthcare; 2007. p. 61,56.
|
| 4. | Petersen GM, Brensinger JD, Johnson KA, Giardiello FM. Genetic testing and counseling for hereditary forms of colorectal cancer. Cancer 1999;86:2540-50.
|
| 5. | Medina-Arana V, Barrios Y, Fernández-Peralta A, Herrera M, Chinea N, Lorenzo N, et al. New founding mutation in MSH2 associated with hereditary nonpolyposis colorectal cancer syndrome on the Island of Tenerife. Cancer Lett 2005;244:268-73.
|
| 6. | Raedle J, Trojan J, Brieger A, Weber N, Schäfer D, Plotz G, et al. Bethesda guidelines: Relation to microsatellite instability and MLH1 promoter methylation in patients with colorectal cancer. Ann Intern Med 2001;135:566-76.
|
[Figure 1], [Figure 2]
|









