|
 
 |
|
EDITORIAL |
|
|
|
| Year : 2011 | Volume
: 17
| Issue : 3 | Page : 117-119 |
| |
Incidence of down syndrome: Hypotheses and reality
Babu Rao Vundinti, Kanjaksha Ghosh
Department of Cytogenetics, National Institute of Immunohaematology (ICMR), KEM Hospital Campus, Parel, Mumbai, India
| Date of Web Publication | 20-Jan-2012 |
Correspondence Address:
Babu Rao Vundinti
Department of Cytogenetics, National Institute of Immunohaematology (ICMR), 13th Floor, New Multistoried Building, KEM Hospital Campus, Parel, Mumbai - 400012
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.92080

How to cite this article:
Vundinti BR, Ghosh K. Incidence of down syndrome: Hypotheses and reality. Indian J Hum Genet 2011;17:117-9 |
The chromosomal basis of Down syndrome (DS), trisomy 21, has been recognized for half a century [1] and various hypotheses such as gamete aging, production line hypothesis, overripe oocytes, chiasma hormonal hypothesis, altered embryonic selection, and limited oocyte pool were proposed to understand the mechanism of non-disjunction of chromosome 21. [2],[3] The parental age, in particular, maternal age, has been thought as an important factor for DS occurrence. Advanced maternal age, first proposed by Penrose [4] in 1933 as an etiological factor for DS, is still strongly associated with DS births. Cytogenetic studies on DS children from all over the world unambiguously reported pure trisomy 21 in majority of the DS cases, which indicates non-disjunction of chromosome 21 in one of the parents during gametogenesis. In this issue, EI-Gilany and colleagues [5] have reported the cytogenetic data of a large number (712) of DS children. The authors have shown the advanced mean maternal age (36.8 years) in their study group. Though a high frequency of DS children is born to young mothers, the hospital-based studies clearly indicate the increased incidence in mothers of advanced age group. Many researchers have attempted to study the parental origin of extra chromosome 21 using chromosome 21 specific markers and all the reports in the literature show that approximately 90% of meiotic errors are maternal. The investigators started looking into the maternal factors in the birth of DS children. A number of hypotheses center on the general aspects of ovarian function such as maternal age related changes associated with oocyte pool size or hormone function. These general hypotheses stimulated researchers to seek the underlying mechanisms by assessing specific oocyte components for their vulnerability to maternal aging, including mitochondria, the spindle apparatus, and sister cohesion protein complexes. [6] Others have investigated indicators of oocyte pool size such as hormone profiles or antral follicle counts to determine if a woman who has had a non-disjunction also has smaller oocyte reserves than controls. [7] The maternal age dependent chromosome non-disjunction has led investigators to examine the effect of grandmaternal age. [8] The most commonly proposed mechanism for a grandmaternal age effect involves non-disjunction in grandmaternal oocytes resulting in mosaic embryo (mother) with the capability of producing trisomy child, hence undetected mosaicism may be one of the factors for DS at birth.
Recent observations suggesting a relationship between trisomy 21 and maternal polymorphisms in the genes of folate and homocysteine metabolism have generated considerable interest. It was proposed that the altered methylation patterns resulting from abnormal folate metabolism may increase DNA hypomethylation in centromeric and pericentromeric regions, thus increasing the risk of chromosome non-disjunction. This effect indicated that maternal polymorphisms in enzymes involved in this metabolic path way may represent a risk factor for DS. In vivo and in vitro folate deficiency has been associated with DNA hypomethylation, DNA strand break, and abnormal or impaired chromosome segregation. Methylenetetrahydrofolate reductase (MTHFR) is one of the most important enzymes in folate/homocysteine metabolism. It is responsible for the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate through the conversion of homocysteine to methionine for nucleotide synthesis. C677T and A1298C polymorphisms in this MTHFR gene affect this pathway by reducing the enzyme activity. Case-control studies have investigated the effect of folate pathway polymorphisms as possible risk factors for DS. Some of these studies reported an association between MTHFR polymorphisms and trisomy 21, whereas others could not find any association. Epidemiologic studies have shown that the use of periconceptional vitamin supplementation with folic acid decreases the risk of congenital heart disease in offspring, but the mechanisms involved in this protective effect of folic acid are not yet known. [9]
The environmental factors also believed to play an important role in non-disjunction of chromosome 21. Sperling and his group [10] carried out a study in Europe after the Chernobyl reactor accident and reported the increased incidence of DS births in low-dose irradiation exposed regions. More recently, a study conducted by Ghosh et al., [11] from India showed that chewing tobacco and using contraceptive pill play a role as risk factors of DS.
In reality, few published and our unpublished data report that a high frequency of DS birth occurs in mothers of younger age group (mean age 26 years), [12] which indicates fall in mean maternal age and this fall has been thought to be a consequence of environmental pollution. A change in the economic condition and needs of life confront with nutrition, health, and hygiene and show their effect on the future progeny. The triple marker test can be used to screen all the pregnancies and it has limitations and it indicates age-related risk of DS. Though prenatal diagnosis can prevent DS, there is a need to monitor pregnancies through folic acid supplementation in mothers. The paternal factors are less focused at in the birth of DS, but occupational exposure and habits need to be studied for a better understanding of the origin of trisomy 21. Though various hypotheses and presumed factors [Figure 1] are associated with the incidence of birth of trisomy 21 children, the search of the gene controlling chromosomal segregation is yet to add to the understanding of non-disjunction of chromosome 21 in DS children.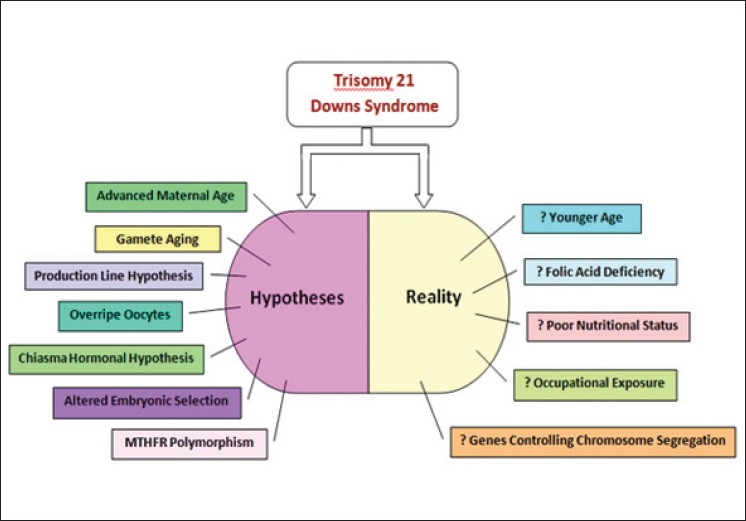 | Figure 1: The factors associated with the non-disjunction of chromosome 21 in DS children
Click here to view |
 References References | |  |
| 1. | Lejeune J. Le Mongolism. Premier exemple d' aberration autosomique humaine. Ann Genet 1959;1:41-9. 
|
| 2. | Rao VB, Kumari CK, Sujatha M, Isaac GS. Maternal reproductive history and the occurrence of Down's syndrome. J Indian Med Assoc 1997;95:495-6.
[PUBMED] |
| 3. | Sherman SL, Freeman SB, Allen EG, Lamb NE. Risk factors for nondisjunction of trisomy 21. Cytogenet Genome Res 2005;111:273-80.
[PUBMED] [FULLTEXT] |
| 4. | Penrose LS. The relative effects of paternal and maternal age in Mongolism. 1933. J Genet 2009;88:9-14.
[PUBMED] [FULLTEXT] |
| 5. | EI-Gilany AH, Yahias, Shoker M, EI-Dahtory. Cytogenetic and comorbidity profile of Down syndrome in Mansoura University children's hospital, Egypt. Indian J Hum Genet 2011;17:157-63.
|
| 6. | Steuerwald NM, Steuerwald MD, Mailhes JB. Post-ovulatory aging of mouse oocytes leads to decreased MAD2 transcripts and increased frequencies of premature centromere separation and anaphase. Mol Hum Reprod 2005;11:623-30.
[PUBMED] [FULLTEXT] |
| 7. | Warburton D. Biological aging and etiology of aneuploidy. Cytogenet Genome Res 2005;111:266-72.
[PUBMED] [FULLTEXT] |
| 8. | Malini SS, Ramachandra NB. Influence of advanced age of maternal grandmothers on Down syndrome. BMC Med Genet 2006;7:4.
[PUBMED] [FULLTEXT] |
| 9. | Brandalise AP, Bandinelli E, dos Santos PA, Roisenberg I, Schuler-Faccini L. Evaluation of C677T and A1298C polymorphisms of the MTHFR gene as maternal risk factors for Down syndrome and congenital heart defects. Am J Med Genet Part A 2009;149A:2080-7.
|
| 10. | Sperling L, Neitzel H, Scherb H. Evidence for an increase in trisomy 21 (Down syndrome) in Europe after the Chernobyl reactor accident. Genet Epidemiol 2011. [In press]
|
| 11. | Ghosh S, Hong CS, Feingold E, Ghosh P, Ghosh P, Bhaumik P, et al. Epidemiology of down syndrome: New insight into the multidimensional interactions among genetic and environmental risk factors in the oocyte. Am J Epidemiol 2011;174:1009-16.
[PUBMED] [FULLTEXT] |
| 12. | Rao VB. Mean maternal age of Down's syndrome in Hyderabad, India. J Indian Med Assoc 1999;97:25.
[PUBMED] |
[Figure 1]
| This article has been cited by | | 1 |
Prevalence of mosaicism for trisomy 21 and cytogenetic variant analysis in patients with clinical diagnosis of down syndrome: A 24-year review (1986-2010) at the servicio de genética, hospital general de México "Dr. Eduardo Liceaga" |
|
| Garduño-Zarazúa, L.M. and Giammatteo Alois, L. and Kofman-Epstein, S. and Peredo, A.B.C. | | Boletin Medico del Hospital Infantil de Mexico. 2013; 70(1): 29-34 | | [Pubmed] | | | 2 |
The incidence of down syndrome in newborns at the department of obstetrics and gynecology of the clinical center Kragujevac during the period 2007-2012 [Incidenca daunovog sindroma kod novorod{stroke |
|
| Dimitrijevic, A. and Varjacic, M. and Davidovic, G. and Lazovic, J. and Novakovic, T. | | Medicinski Casopis. 2013; 47(1): 12-16 | | [Pubmed] | |
|
|
|
|









