|
 
 |
|
ORIGINAL ARTICLE |
|
|
|
| Year : 2011 | Volume
: 17
| Issue : 3 | Page : 201-206 |
| |
Risk conferred by FokI polymorphism of vitamin D receptor (VDR) gene for essential hypertension
N Swapna1, U Mohana Vamsi1, G Usha2, T Padma1
1 Department of Genetics, Osmania University, Hyderabad, India
2 Department of Genetics, Durgabai Deshmukh Hospital, Hyderabad, India
| Date of Web Publication | 20-Jan-2012 |
Correspondence Address:
T Padma
Department of Genetics, Osmania University, Hyderabad-500 007, Andhra Pradesh
India
 Source of Support: None, Conflict of Interest: None  | 16 |
DOI: 10.4103/0971-6866.92104

 Abstract Abstract | | |
Background : The vitamin D receptor (VDR) gene serves as a good candidate gene for susceptibility to several diseases. The gene has a critical role in regulating the renin-angiotensin system (RAS) influencing the regulation of blood pressure. Hence determining the association of VDR polymorphisms with essential hypertension is expected to help in the evaluation of risk for the condition.
Aim : The aim of this study was to evaluate association between VDR Fok I polymorphism and genetic susceptibility to essential hypertension.
Materials and Methods : Two hundred and eighty clinically diagnosed hypertensive patients and 200 normotensive healthy controls were analyzed for Fok I (T/C) [rs2228570] polymorphism by polymerase chain reaction and restriction fragment length polymorphism (PCR-RFLP) analysis. Genotype distribution and allele frequencies in patients and controls, and odds ratios (ORs) were calculated to predict the risk for developing hypertension by the individuals of different genotypes.
Results : The genotype distribution and allele frequencies of Fok I (T/C) [rs2228570] VDR polymorphism differed significantly between patients and controls (χ2 of 18.0; 2 degrees of freedom; P = 0.000). FF genotype and allele F were at significantly greater risk for developing hypertension and the risk was elevated for both the sexes, cases with positive family history and habit of smoking.
Conclusions : Our data suggest that VDR gene Fok I polymorphism is associated with the risk of developing essential hypertension
Keywords: Essential hypertension, risk prediction, VDR gene Fok I polymorphism, vitamin D
How to cite this article:
Swapna N, Vamsi U M, Usha G, Padma T. Risk conferred by FokI polymorphism of vitamin D receptor (VDR) gene for essential hypertension. Indian J Hum Genet 2011;17:201-6 |
How to cite this URL:
Swapna N, Vamsi U M, Usha G, Padma T. Risk conferred by FokI polymorphism of vitamin D receptor (VDR) gene for essential hypertension. Indian J Hum Genet [serial online] 2011 [cited 2016 May 13];17:201-6. Available from: http://www.ijhg.com/text.asp?2011/17/3/201/92104 |
| Introduction | |  |
Essential hypertension is a typical example of a complex, multifactorial, and polygenic trait. It is most likely that there are several causal genes, which together contribute to between 30% and 50% of the variation in blood pressure among humans. [1] These genetic determinants interact with environmental factors to produce the final disease phenotype. Identifying gene variants that contribute to hypertension may not only provide better understanding of the pathophysiology of the disease but also may elucidate the biochemical and physiological pathways that link various risk factors causing susceptibility to the condition. Despite very significant recent progress made in genomic and statistical methodologies, the genetic dissection of human essential hypertension still throws a major challenge.
Growing evidence points to vitamin D as having an important association with blood pressure. Data from animal studies implicate circulating active vitamin D as an inhibitor of renin expression in the juxtaglomerular apparatus and vascular smooth muscle cell proliferation. [2],[3] Oral supplementation with vitamin D is found to lower blood pressure in hypertensive rats. [4],[5] In humans, a cross-sectional data suggest an association between low vitamin D intake (<400 IU per day) and increase in blood pressure [6] and a single interventional study in vitamin D deficient elderly women found that a combination of calcium and vitamin D supplementation had a greater blood pressure lowering effect than calcium supplementation alone [7] Vitamin D is also regarded as a potent endocrine suppressor of renin biosynthesis to regulate the rennin angiotensin system (RAS). [8]
Vitamin-D is a member of the steroid receptor family and mediates the effects of the active metabolite 1, 25(OH) 2 vit D3 by regulating transcription of a number of different cellular genes. The action of vitamin D is mediated through its binding to nuclear receptor (VDR). Studies have demonstrated that vitamin D receptors are present in aortic endothelial [9] and vascular smooth muscle cells [10] and also VDR polymorphisms influence the susceptibility to coronary artery disease. [11]
The gene encoding the VDR is located on chromosome 12cen-q12, [12] contains 11 exons [13] and spans approximately 75 kb of genomic DNA [14] Several polymorphisms have been identified in the gene including the Fok I polymorphism located in exon 2 at the 5′ coding region of the gene. [15] Fok I polymorphism results in different translation initiation sites due to thymine (T) to cytosine (C) substitution in the first translation initiation codon ATG (methionine) which generates long and short variants of VDR. In the VDR ff variant initiation of translation occurs at the first ATG site, giving rise to a full length VDR protein comprised of 427 amino acids. Conversely, in the VDR FF variant translation begins at the second ATG site instead of the first, resulting in a truncated protein with three amino acids less. This is the only known VDR polymorphism resulting in two different VDR protein products. [15]
In the present study, we analyzed the exon 2 initiation codon (VDR-Fok I gene) polymorphism in hypertensive individuals for its contributing role.
| Materials and Methods | | |
Study subjects
A total of 280 individuals in the age group of 35-60 years whose blood pressure measurements exceeded 140 mmHg systolic or 90 mmHg diastolic, recruited at different hospitals in the city of Hyderabad were examined for the Fok I polymorphism of VDR gene. Age- and sex-matched controls (n = 200) whose blood pressure measurements were in normal range (120 mmHg systolic or 80 mmHg diastolic) and without any apparent diseases like diabetes, CAD etc were randomly selected to compare with the patient data.
Assessment of other covariates
From all the cases and controls recorded, information was collected using a proforma specifically prepared. The questionnaire included information on sex, age, age at onset, duration of the disease, body mass index (BMI; calculated as weight in kilograms divided by height in meters squared), smoking status, alcohol consumption, associated conditions like diabetes, CAD etc. Pedigrees covering 3-4 generations were also constructed for each case.
Genotyping of the Fok I polymorphism
With the consent from the individuals chosen for the study, genomic DNA from 280 hypertensives and 200 controls was isolated using salting out method. [16] The genomic DNA was amplified using the primers forward (5'- AGCTGGCCC TGGCACTGA CTCTGCTCT -3') and reverse (5'- ATGGAAACACCTTGCTTCTTCTCCCTC - 3') for the genotyping of Fok I polymorphism of VDR gene.
Polymerase chain reaction (PCR) was carried out in a total volume of 10 μl containing 100-200ng of genomic DNA, 25 pmol of each primer, 200 μM dNTPs, 2.5 units of Taq polymerase, and 1X Taq Polymerase buffer (1.5mM Mgcl2) (Sigma Aldrich Pvt. Ltd.) DNA samples were amplified with cycling parameters as follows: Denaturation at 94° C for 5 min, 35 cycles at 94° C for 30 s, 61° C for 30 s and 72° C for 60 s and one final cycle of extension at 72° C for 7 min. The T/C polymorphism in the first of two-start codon (ATG) at the translation initiation site of the VDR gene was detected by RFLP using the restriction endonuclease Fok-I. The PCR product with 265bp was digested with 3.0 units of Fok I restriction enzyme (New England Biolabs) and incubated at 37° C for 4 h; 5 μl of the digested reaction mixture was then electrophoresed for 2 h at 150 V using 9% PAGE (polyacrylamide gel electrophoresis) containing ethidium bromide and visualized under UV and photographed. The sizes of the digested fragments were determined using 100-bp ladder (New England Biolabs). PCR products with an undigested large band were genotyped as FF homozygotes (265 bp), those with a smaller digested band were genotyped as ff homozygotes(169 bp and 96 bp), and those with a large and small bands were genotyped as Ff heterozygotes (265,169 and 96).
Statistical analysis
The distribution of genotype frequencies of VDR gene polymorphisms in the cases and controls were compared using 2* 2 contingency χ2 -tests. Continuous variables such as age, age at onset, BMI, duration of hypertension (at the time of investigation) and lipid levels were expressed as mean and standard error of mean; these means were compared by Student's t test for independent samples. P < 0.05 was considered as significant.
| Results | | |
[Table 1] describes the demographic features and lipid profile associated with hypertensive (n =280) and normotensive (n=200) individuals. Among the patients, there was higher preponderance of males (53.2%) as compared to females (46.8%). Significant preponderance of cases with positive family history (64.3%) and obesity (20.8%) were observed among hypertensives as compared to controls (familial -39.0%; obese -12.0%). Also there was significant elevation in the mean levels of BMI and reduction of HDL levels in hypertensive as compared to controls [Table 1]. The results suggest that males had high risk for developing hypertension and risk factors like obesity, family history and low HDLcholesterol levels significantly increase the risk for hypertension.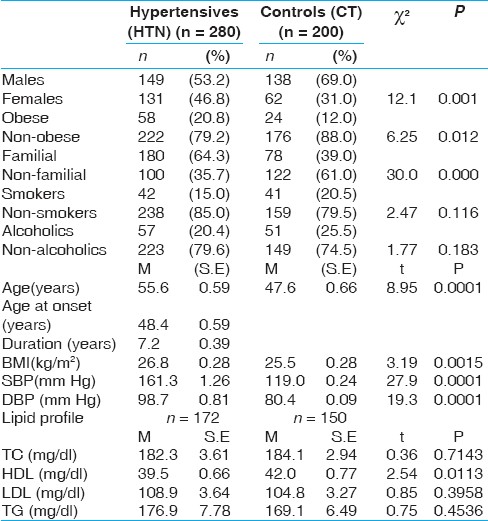 | Table 1: Demographic features and lipid profile of the hypertensives and controls
Click here to view |
The frequencies of Fok I genotypes at VDR locus showed a significant difference with the distribution of genotypes being 53.6% of FF, 35.7% of Ff and 10.7% of ff among patients and 34.0% of FF, 51.0% of Ff and 15.0% of ff among the controls (χ2 of 18.0; 2 degrees of freedom; P = 0.000). Further the frequency of VDR genotypes deviated significantly from Hardy-Weinberg equilibrium (χ2 =4.38, P<0.05, at 1df: frequencies of allele F 0.71 and f 0.29) in hypertensives but not in controls (χ2 =0.675, P>0.05, at 1df: frequencies of allele F 0.59 and f 0.41) indicating possible association of this polymorphism with hypertension [Table 2]. 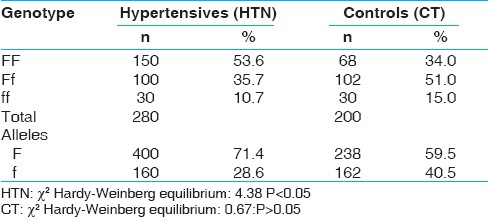 | Table 2: Distribution of genotypes of VDR gene Fok I polymorphism in hypertensives and controls
Click here to view |
Odds ratios were computed to evaluate the risk for each genotype as against other genotypes for developing hypertension [Table 3]. The analysis revealed high risk for hypertension in FF homozygotes which was 2.25 times as compared to Ff heterozygotes and 2.20 times as compared to ff homozygotes, while comparison of Ff vs ff genotypes did not show any significant risk.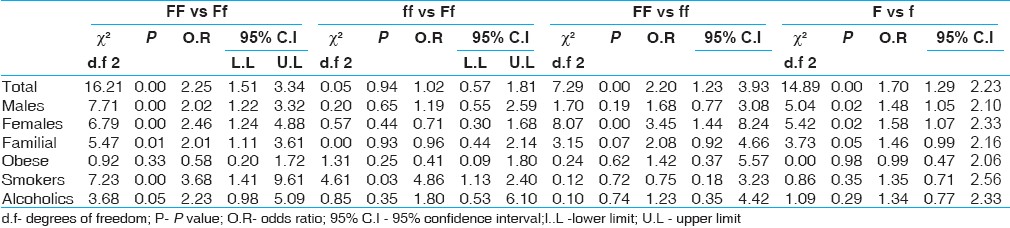 | Table 3: Risk predictions for different genotypes of VDR Fok1 polymorphism causing susceptibility to essential hypertension
Click here to view |
Considering the cohorts, the risk for hypertension was found both for males and females with FF genotypes as against Ff genotypes (χ2 =7.716, P<0.05, at 1df, O.R -2.020;95% C.I 1.228-3.322 and χ2 =6.794, P<0.05, at 1df, O.R -2.467;95% C.I 1.246-4.881). Similarly, risk for hypertension for FF genotype was significant in patients with positive family history (χ2 =5.473, P<0.05, at 1df, O.R -2.011;95% C.I 1.119-3.616) and habit of smoking (χ2 =7.234, P<0.05, at 1df, O.R -3.686;95% C.I 1.414-9.611) and alcohol consumption. (χ2 =3.682, P<0.05, at 1df, O.R -2.239; 95% C.I 0.983-5.096). All these comparisons showed high risk for homozygotes (FF) and this observation could be due to generally observed high risk for FF individuals for developing hypertension [Table 3].
When individuals of FF vs ff genotypes were tested, significant risk was found for hypertension in general (χ2 =7.291, P<0.05, at 1df; with O.R -2.206;95% C.I 1.238-3.932) and for females (χ2 =8.077, P<0.05, at 1df, O.R -3.453; 95% C.I 1.449-8.246) while other cohorts did not show any significant results.
When risk for ff vs Ff individuals was considered, significant OR was obtained only for individuals with the habit of smoking (χ2 =4.613, P<0.05, at 1df, O.R -4.861; 95% C.I 1.13-2.40).
Allele F showed significant risk for hypertension as compared to allele f (χ2 =14.864, P<0.05, at 1df with O.R -1.702; 95% C.I 1.298-2.231) [Table 3]. The risk for F allele carriers was significant for male patients (χ2 =5.045, P<0.01, at 1df, O.R -1.488; 95% C.I 1.052-2.105), and also female patients (χ2 =5.425, P<0.01, at 1df, O.R -1.582; 95% C.I 1.075-2.330) and individuals with positive family history (χ2 =3.738, P <0.05, at 1df, O.R -1.467; 95% C.I 0.995-2.163) of hypertension.
Odd's ratios were also computed for each genotype comparing with the pooled frequencies of other two genotypes [Table 4]. This analysis revealed significant risk for individuals with FF genotype as compared to Ff + ff genotypes (χ2 =17.25, P <0.01, at 1df; with O.R -2.24; 95% C.I 1.54-3.26). This analysis based on pooling the genotypes also supported earlier observation of high risk for FF homozygotes which was 2.2 times as against other genotypes. Significant risk was also observed in both the sexes and in subjects with positive family history [Table 4].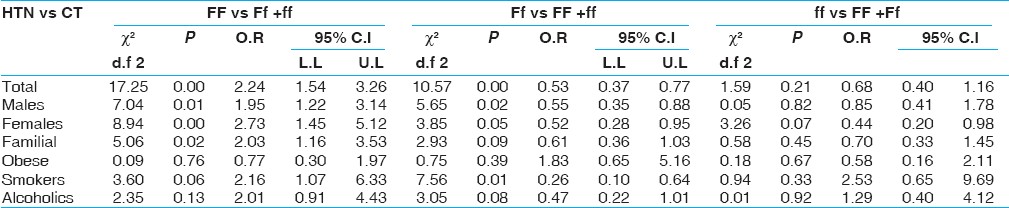 | Table 4: Risk prediction for specific genotype of VDR Fok1 polymorphism in relation to other two genotypes causing susceptibility to essential hypertension
Click here to view |
When the frequency of Ff vs FF + ff was considered, significant risk for hypertension was observed in general (χ2 =10.57, P<0.01, at 1df; with O.R -0.053;95% C.I 0.37-0.77) and also when individuals were males (χ2 =5.65, P<0.01, at 1df, O.R -0.55; 95% C.I 0.35-0.88) and when they were with the habit of smoking (χ2 =7.56, P<0.05, at 1df, O.R -0.26; 95% C.I 0.10-0.64). This analysis reveals that individuals with Ff genotypes are protected from developing hypertension.
In conclusion, the results obtained suggest that FF genotype and allele F were at a greater risk for developing hypertension and the risk was elevated for both the sexes, cases with positive family history and habit of smoking. The data also supported the protection conferred by heterozygous genotype (Ff) for developing hypertension.
| Discussion | | |
The vitamin D receptor (VDR) has been identified in many cell types, tissues, and organs, including those not typically associated with calcium homeostasis and bone metabolism indicating that vitamin D may also be involved in important biological processes beyond calcium homeostasis. [17] 1,25-dihydroxyvitamin D3 [1,25(OH) 2 D3] binds to the VDR, and the activated VDR regulates the rate of transcription of vitamin D-responsive genes [18]
Inappropriate stimulation of the RAS has been associated with hypertension. In wild-type mice, physiological levels of 1.25 dihydroxy vitamin D (1.25(OH) 2 D) found to inhibit renin expression in juxtaglomerular cells, whereas an inhibitor of 1.25(OH) 2 D biosynthesis increased the expression of renin. [8] Vitamin D is thus regarded as a potent endocrine suppressor of renin biosynthesis to regulate the RAS. [8] Mice lacking VDR had elevated production of renin and angiotensin II independent of calcium metabolism, leading to hypertension, cardiac hypertrophy, and increased water intake. In normal mice, vitamin D deficiency stimulated renin expression, whereas injection of 1,25(OH) 2 D3 reduced renin synthesis [8] In cell cultures, 1,25(OH) 2 D directly suppressed renin gene transcription by a VDR-dependent mechanism. Thus, vitamin D-deficiency may increase the risk of hypertension, and vitamin D supplementation may be beneficial to the cardiovascular system.
The molecular effects of vitamin D on the RAS have been clarified by the finding that liganded VDR suppresses renin expression by binding to the transcription factor cAMP-response element-binding protein (CREB). [19] As a result, stimulation of renin transcription is inhibited because CREB is no longer able to stimulate renin transcription by binding to cAMP response elements in the promoter region of the renin gene. [20] In patients with hypertension, renin activity has been inversely associated with 1,25(OH) 2 D levels. [20],[21]
In ff variant of Fok I polymorphism of VDR gene, initiation of translation occurs at the first ATG site, giving rise to a full length VDR protein comprised of 427 amino acids. Conversely, in the VDR FF variant, translation begins at the second ATG site instead of the first, resulting in a truncated protein with three amino acids lesser. The present study found an association of FF genotype of Fok I polymorphism of VDR gene with hypertension. Hence truncated vitamin D receptor protein (VDR) formed in FF homozygotes may have elevated production of renin and angiotensin II leading to the development of hypertension/ elevated blood pressure.
Further studies are needed to find out if and when vitamin D supplementation should be used for treating patients with hypertension. It is apparent that vitamin D supplementation may be appropriate for populations that are most vulnerable to hypovitaminosis D. Studies to find vitamin D analogs with minimal calcemic potential but greater activity on RAS modulation are needed. This may find a group of therapeutic inhibitors of the RAS and potentially offer a new class of antihypertensive drugs that may be used to treat hypertensive individuals with or without vitamin D deficiency.
| References | | |
| 1. | Ward R. Familial aggregation and genetic epidemiology of blood pressure. In: Laragh JH, Brenner BM, editors. Hypertension: Pathophysiology, Diagnosis and Management. New York: Raven; 1990. p. 811-100. 
|
| 2. | Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1, 25-Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin system. J Clin Invest 2002;110:229-38.
[PUBMED] [FULLTEXT] |
| 3. | Carthy EP, Yamashita W, Hsu A, Ooi BS. 1, 25-Dihydroxyvitamin D3and rat vascular smooth muscle cell growth. Hypertension 1989;13:954-9.
[PUBMED] [FULLTEXT] |
| 4. | Borges AC, Feres T, Vianna LM, Paiva TB. Recovery of impaired K channels in mesenteric arteries from spontaneously hypertensive rats by prolonged treatment with cholecalciferol. Br J Pharmacol 1999;127:772-8.
[PUBMED] [FULLTEXT] |
| 5. | Feres T, Vianna LM, Paiva AC, Paiva TB. Effect of treatment with vitamin D3 on the responses of the duodenum of spontaneously hypertensive rats to bradykinin and to potassium. Br J Pharmacol 1992;105:881-4.
[PUBMED] [FULLTEXT] |
| 6. | Sowers MR, Wallace RB, Lemke JH. The association of intakes of vitamin D and calcium with blood pressure among women. Am J Clin Nutr 1985;42:135-42.
[PUBMED] [FULLTEXT] |
| 7. | Pfeifer M, Begerow B, Minne HW, Nachtigall D, Hansen C. Effects of a short-term vitamin D(3) and calcium supplementation on blood pressure and parathyroid hormone levels in elderly women. J Clin Endocrinol Metab 2001;86:1633-7.
[PUBMED] [FULLTEXT] |
| 8. | Li YC, Qiao G, Uskokovic M, Xiang W, Zheng W, Kong J. Vitamin D: A negative endocrine regulator of the renin-angiotensin system and blood pressure J Steroid Biochem Mole Biol 2004;89-90:387-92.
|
| 9. | Merke J, Milde P, Lewicka S, Hügel U, Klaus G, Mangelsdorf DJ Identification and regulation of 1,25-dihydroxyvitamin D3 receptor activity and biosynthesis of 1,25-dihydroxyvitamin D3. Studies in cultured bovine aortic endothelial cells and human dermal capillaries. J Clin Invest 1989;83:1903-15.
|
| 10. | Merke J, Hofmann W, Goldschmidt D, Ritz E Demonstration of 1,25(OH)2 vitamin D3 receptors and actions in vascular smooth muscle cells in vitro. Calcif Tissue Int 1987;41:112-4.
|
| 11. | Van Schooten FJ, Hirvonen A, Maas LM Putative susceptibility markers of coronary artery disease: Association between VDR genotype, smoking, and aromatic DNA adduct levels in human right atrial tissue. FASEB J 1998;12:1409-17.
|
| 12. | Taymans SE, Pack S, Pak E, Orban Z, Barsony J, Zhuang ZThe human vitamin D Receptor Gene (VDR) Is localized to region 12cen-q12 by fluorescent in situ hybridization and radiation hybrid mapping: Genetic and physical VDR Map. J Bone Mineral Res 1999;14:1163-6.
|
| 13. | Crofts LA, Hancock MS, Morrison NA, Eisman JA. Multiple promoters direct the tissue-specific expression of novel N-terminal variant human vitamin D receptor gene transcripts. Proc Natl Acad Sci USA 1998;95:10529-34.
[PUBMED] [FULLTEXT] |
| 14. | Miyamoto K, Kesterson RA, Yamamoto H, Taketani Y, Nishiwaki E, Tatsumi SStructural organization of the human vitamin D receptor chromosomal gene and its promoter. Mol Endocrinol 1997;11:1165-79.
|
| 15. | WhitfieldGK, Remus LS, Jurutka PW, Zitzer H, Oza AK, Dang HT Functionally relevant polymorphisms in the human nuclear vitamin D receptor gene. Mol Cell Endocrinol 2001;177:145-59.
|
| 16. | Miller S, Dykes D, Polesky H. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 1988;16:1215.
|
| 17. | Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr 2004;80(6 Suppl):1678-88S.
|
| 18. | Brown AJ, Dusso A, Slatopolsky E. Vitamin D. Am J Physiol 1999;277:F157-75.
[PUBMED] [FULLTEXT] |
| 19. | Yuan W, Pan W, Kong J, Zheng W, Szeto FL, Wong KE. 1,25-Dihydroxyvitamin D3 suppresses renin gene transcription by blocking the activity of the cyclic AMP response element in the renin gene promoter. J Biol Chem 2007;282:29821-30.
|
| 20. | Resnick LM, Muller FB, Laragh JH. Calcium-regulating hormones in essential hypertension Relation to plasma renin activity and sodium metabolism. Ann Intern Med 1986;105:649-54.
|
| 21. | Burgess E, Hawkins D, Watanabe RG. Interaction of 1,25-dihydroxyvitamin D and plasma renin activity in high renin essential hypertension. Am J Hypertens 1990;3:903-5.
|
[Table 1], [Table 2], [Table 3], [Table 4]
| This article has been cited by | | 1 |
The renin–angiotensin–aldosterone system and calcium-regulatory hormones |
|
| A Vaidya,J M Brown,J S Williams | | Journal of Human Hypertension. 2015; | | [Pubmed] | [DOI] | | | 2 |
Vitamin D receptor gene polymorphisms (TaqI and ApaI) in relation to 25-hydroxyvitamin D levels and coronary artery disease incidence |
|
| Mohamed A. Abu el Maaty,Sally I. Hassanein,Hameis M. Sleem,Mohamed Z. Gad | | Journal of Receptors and Signal Transduction. 2014; : 1 | | [Pubmed] | [DOI] | | | 3 |
Genetic variants of vitamin D receptor and susceptibility to ischemic stroke |
|
| Puttachandra Prabhakar,Vijaya Majumdar,Girish Baburao Kulkarni,Rita Christopher | | Biochemical and Biophysical Research Communications. 2014; | | [Pubmed] | [DOI] | | | 4 |
Vitamin D receptor gene polymorphisms and plasma renin activity in essential hypertensive individuals |
|
| S Cottone,L Guarino,R Arsena,C Scazzone,F Tornese,M Guarneri,C Guglielmo,A Bono,G Mulè | | Journal of Human Hypertension. 2014; | | [Pubmed] | [DOI] | | | 5 |
Vitamin D Receptor Genetic Polymorphism Is Significantly Associated With Decreased Risk of Hypertension in a Chinese Han Population |
|
| Jian Jia,Chong Shen,Lina Mao,Keming Yang,Chen Men,Yiyang Zhan | | The Journal of Clinical Hypertension. 2014; 16(9): 634 | | [Pubmed] | [DOI] | | | 6 |
What Do We Know and Do Not Know About Vitamin D?: A Causal Association Between Vitamin D Receptor Genetic Polymorphism and Hypertension |
|
| Yalcin Solak,Adrian Covic,Mehmet Kanbay | | The Journal of Clinical Hypertension. 2014; : n/a | | [Pubmed] | [DOI] | | | 7 |
The Vitamin D receptor (VDR) gene polymorphisms in Turkish brain cancer patients |
|
| Toptaş, B. and Kafadar, A.M. and Cacina, C. and Turan, S. and Yurdum, L.M. and Yiǧitbaşi, N. and Gökçe, M.O. and Zeybek, Ü. and Yaylim, I. | | BioMed Research International. 2013; 2013(295791) | | [Pubmed] | | | 8 |
Effects of Vitamin D on Blood Pressure and Endothelial Function |
|
| Bokyung Min | | The Korean Journal of Physiology & Pharmacology. 2013; 17(5): 385 | | [Pubmed] | [DOI] | | | 9 |
The Vitamin D Receptor (VDR) Gene Polymorphisms in Turkish Brain Cancer Patients |
|
| Bahar Toptas,Ali Metin Kafadar,Canan Cacina,Saime Turan,Leman Melis Yurdum,Nihal Yigitbasi,Muhammed Oguz Gökçe,Ümit Zeybek,Ilhan Yaylim | | BioMed Research International. 2013; 2013: 1 | | [Pubmed] | [DOI] | | | 10 |
Vitamin D receptor polymorphisms in hypertensive disorders of pregnancy |
|
| Vania B. Rezende,Valeria C. Sandrim,Ana C. Palei,Lorena Machado,Ricardo C. Cavalli,Geraldo Duarte,Jose E. Tanus-Santos | | Molecular Biology Reports. 2012; 39(12): 10903 | | [Pubmed] | [DOI] | | | 11 |
Prevalence of vitamin D receptor gene polymorphisms in Mexican children with chronic kidney disease |
|
| Medina-Hernández, E.O. and RodrÃguez-Espino, B.A. and Hernández-Sánchez, A.M. and Ortiz-Vázquez, L.M. and Oropeza, P. and DÃaz, D. and Aldana-Vergara, R. and Velásquez-Forero, F. and Vega, O. and Correa-Rotter, R. and Medeiros, M. | | Boletin Medico del Hospital Infantil de Mexico. 2012; 69(2): 98-103 | | [Pubmed] | | | 12 |
Systematic testing of literature reported genetic variation associated with coronary restenosis: Results of the GENDER study |
|
| Verschuren, J.J.W. and Trompet, S. and Postmus, I. and Sampietro, M.L. and Heijmans, B.T. and Houwing-Duistermaat, J.J. and Slagboom, P.E. and Jukema, J.W. | | PLoS ONE. 2012; 7(8) | | [Pubmed] | |
|
|
|


|
|
|
|
|








