|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2011 | Volume
: 17
| Issue : 3 | Page : 235-237 |
| |
Acute promyelocytic leukemia with unusual karyotype
Mangala Gowri1, SK Kousar Jahan1, Kavitha1, Prasannakumari1, Madhumathi2, L Appaji3
1 Cytogenetics Unit, Department of Pathology, Kidwai Memorial Institute of Oncology, Bangalore - 560029, India
2 Heamatology Unit, Kidwai Memorial Institute of Oncology, Bangalore - 560029, India
3 Department of Pedotric Oncology, Kidwai Memorial Institute of Oncology, Bangalore - 560029, India
| Date of Web Publication | 20-Jan-2012 |
Correspondence Address:
Prasannakumari
Cytogenetics Unit, Department of Pathology, Kidwai Memorial Institute of Oncology, Bangalore - 560 029, Karnataka
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.92093

 Abstract Abstract | | |
Acute myeloid leukemia (AML-M3) is associated with the translocation t(15;17)(q22;q12-21) which disrupts the retinoic acid receptor alpha (RARA) gene on chromosome 17 and the PML gene on chromosome 15. We report a two-year-old patient with AML-M3 without the usual translocation t(15;17). Cytogenetic studies demonstrated normal appearance of chromosome 15 while the abnormal 17 homologue was apparently a derivative 17, der(17)(17qter-cen-q21:), the rearrangement distinctly shows deletion at 17q21 band and the morphology corresponding to an iso chromosome i(17q-). This case report is a rare cytogenetic presentation of acute promyelocytic leukemia (APML).
Keywords: Acute promyelocytic leukemia, karyotype, RARA
How to cite this article:
Gowri M, Kousar Jahan S K, Kavitha, Prasannakumari, Madhumathi, Appaji L. Acute promyelocytic leukemia with unusual karyotype. Indian J Hum Genet 2011;17:235-7 |
How to cite this URL:
Gowri M, Kousar Jahan S K, Kavitha, Prasannakumari, Madhumathi, Appaji L. Acute promyelocytic leukemia with unusual karyotype. Indian J Hum Genet [serial online] 2011 [cited 2016 May 13];17:235-7. Available from: http://www.ijhg.com/text.asp?2011/17/3/235/92093 |
| Introduction | |  |
Acute promyelocytic leukemia (APML) is a subset of AML with characteristic clinical, morphological and genetic features. The disease is very rare in children below 10 years of age. Its incidence gradually increases, reaching a plateau during early adulthood, remaining constant until it diminishes after 60 years of age. [1] The identification of specific chromosomal abnormality plays an important role in determining therapy and prognosis in certain subtypes of AML. Data from the Pediatric Oncology Group have shown that inv(16) / t(16;16), t(8;21), and normal karyotypes are associated with favorable prognostic outcome, whereas poorer outcome was observed in t(15;17) (without all- trans retinoic acid (ATRA) treatment), 11q23, and other abnormalities. [2]
AML is heterogeneous at the cytogenetic and molecular levels. Over the years, several specific recurrent chromosome aberrations have been described in AML, both unbalanced and balanced rearrangements. [3] Balanced chromosome rearrangements are detected in approximately 25-30% of adults with de novo AML and have attracted a great deal of attention not only because their molecular dissection has led to identification of genes involved in leukemogenesis but also because specific translocations and inversions are associated with clinical features and treatment outcome of patients harboring them. [4],[5],[6] In this article, we discuss the case study of a two-year-old child with unbalanced chromosome aberrations involving chromosome 17 with a cytogenetically normal chromosome 15.
| Case Report | | |
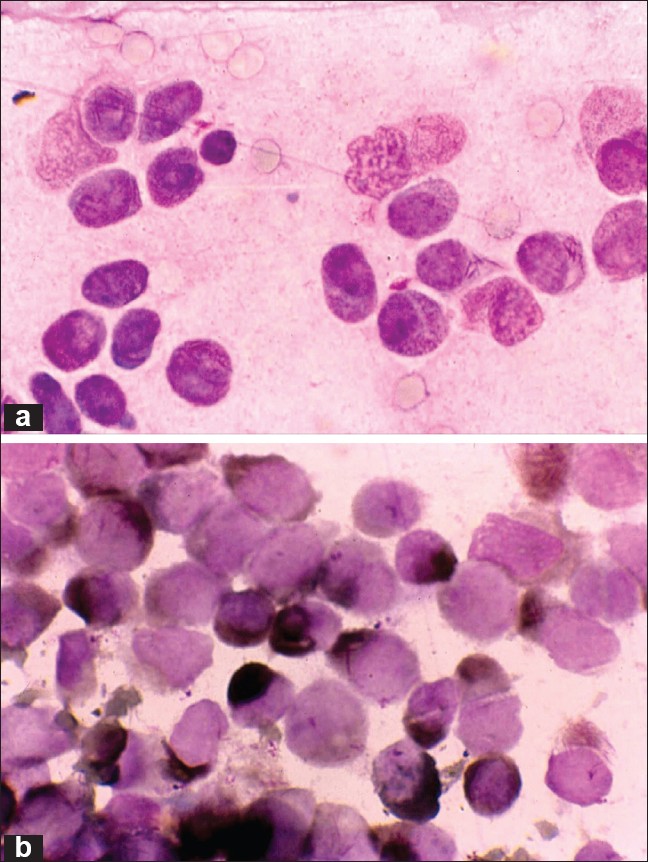
Patient had a history of fever, general weakness and bleeding from the gums. On examination, his general condition was poor, with cervical and axillary lymph nodes. On systemic examination, he had hepatomegaly 2-3 cm, and splenomegaly 1-2 cm. At presentation, hemogram was Hb 69 g/l, total count of 52 × 10 9 /l and platelets 20 × 10 9 /l. Differential count showed neoplastic promyelocytes 80%, neutrophils 12%, lymphocytes 12%, Bone marrow aspiration showed hyper cellular marrow with sheets of neoplastic promyelocytes (70 %). Many bilobed and occasional faggot cells were seen [Figure 1]a. Other elements were suppressed. Myeloperoxidase stain was strongly positive [Figure 1]b. Morphological diagnosis of AML-M3 (hyper granular variant) was made.
Cytogenetic studies
Cytogenetic study was carried out on cells from bone marrow aspiration. Short-term culture of 24 and 48 h were set up using RPMI 1640 medium supplemented with 20% fetal bovine serum. After 16-18 h, 50 μl of colcemid at a final concentration of 10 μg/ml was added for 30 min followed by hypotonic treatment, fixation in Carnoy's fixative. Giemsa (GTG) banding was performed according to standard protocol. Fifteen metaphases were analyzed which consistently showed 46XY, -17,+der(17)(17qter-cen-17q21:) karyotype [Figure 2].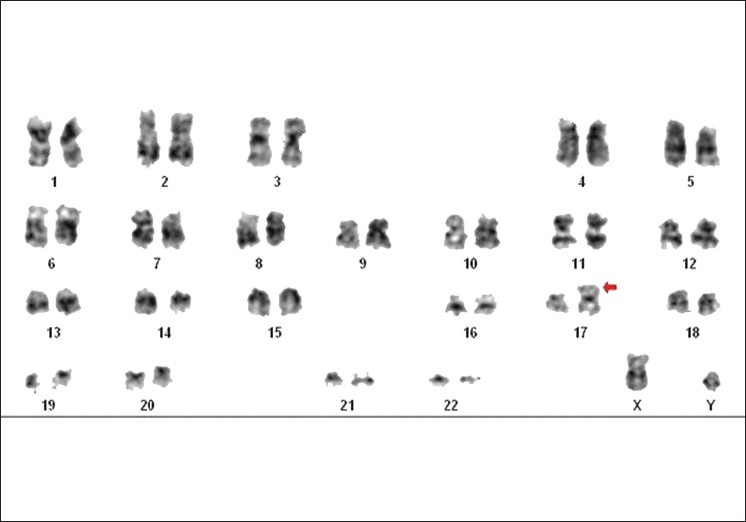 | Figure 2: Karyotype: 46XY, -17, +der(17)(17qter-cen-17q21:) Arrow indicates breakpoint
Click here to view |
| Discussion | | |
To our knowledge, this is a rare cytogenetic abnormality in a child, involving only chromosome 17. The first report of AML-M3 with normal chromosome 15 with -17, ins(17;?) (q11q21;?) was by Baranger et al., [7] in a 35-year-old female. The present case demonstrated normal appearance of chromosome 15's, while one of the 17 homologues appeared to be an iso (17q), but upon detailed examination showed break on one of the arms at q21 band. The presence of 15q+ and i(17q-) is one of the most frequent abnormalities reported besides the standard translocation, [7] but with an i(17q-) and two normal chromosome 15 is extremely rare. Routinely cytogenetics, fluorescence in situ hybridization (FISH), and Polymerase chain reaction (PCR) analysis are employed for the diagnosis and precise localization of the fusion gene. But in our case, FISH could not be performed and even before the cytogenetic results were available the patient died due to disseminated intravascular coagulation. Hence, further molecular studies to establish the type of gene fusion transcript which could have had a prognostic value could not be ascertained.
A small proportion of APML patients do not have t(15;17)/ PML-RARA but do have other chromosomal aberrations and gene fusion, all these rearrangements and t(15;17) are very strongly correlated with characteristic marrow morphology in which abnormal promyelocytes predominate (FAB- M3). The present WHO classification recognizes two main morphological subtypes of APML that includes a more frequent hyper granular variant form featured by abnormal dysplastic promyelocytes with abundant cytoplasmic granules and Auer rods (faggots) and a less frequent micro granular variant of APML characterized by leukemic blast, bilobed nuclei with dusty and minute cytoplasmic granules. The evolution of AML involves leukemogenic events that occur in the stem cell (stem cell origin model) and favors self renewal while disrupting normal hematopoietic cell lineage development. [8],[9],[10]
| References | | |
| 1. | Ribeiro RC, Rego E. Management of APL in developing countries: Epidemiology, challenges and opportunities for international collaboration. Hematology Am Soc Hematol Educ Program 2006:162-8. 
|
| 2. | Raimondi SC, Chang MN, Ravindranath Y. Chromosomal abnormalities in 478 children with acute myeloid leukemia: Clinical characteristics and treatment outcome in a cooperative Pediatric Oncology Group Study - POG 8821. Blood 1999;94:3707-16.
|
| 3. | Mrózek K, Heinonen K, Bloomfield CD. Clinical importance of cytogenetics in acute myeloid leukaemia. Best Pract Res Clin Haematol 2001;14:19-47.
|
| 4. | Byrd JC, Mrózek K, Dodge RK, Carroll AJ, Edwards CG, Arthur DC, et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: Results from Cancer and Leukemia Group B (CALGB 8461). Blood 2002;100:4325-36.
|
| 5. | Slovak ML, Kopecky KJ, Cassileth PA, Harrington DH, Theil KS, Mohamed A, et al. Karyotypic analysis predicts outcome of preremission and post remission therapy in adult acute myeloid leukemia: A Southwest Oncology Group/Eastern Cooperative Oncology Group study. Blood 2000;96:4075-83.
|
| 6. | Grimwade D, Walker H, Harrison G, Oliver F, Chatters S, Harrison CJ, et al. The predictive value of Hierarchical cytogenetic classification in older adults with acute myeloid leukemia (AML): Analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood 2001;98:1312-20.
|
| 7. | Baranger L, Gardembas M, Hillion J, Foussard C, Ifrah N, Boasson M, et al. Laboratoire de Génétique, CHU Angers, France. Rearrangements of the RARA and PML genes in a cytogenetic variant of acute promyelocytic leukemia. Genes Chromosomes Cancer 1993;6:118-20.
|
| 8. | Tallman MS, Nabhan C, Feusner JH, Rowe JM. Acute proyelocytic leukemia: Evolving therapeutic strategies. Blood 2002;99:759-67.
|
| 9. | Lo-Coco F, Ammatuna E. The biology of acute promyelocytic leukemia and its impact on diagnosis and treatment. Hematology Am Soc Hematol Educ Program 2006:156-61.
|
| 10. | Sanz MA. Treatment of acute promyelocytic leukemia. Hematology Am Soc Hematol Educ Program 2006:147-55.
|
[Figure 1], [Figure 2]
| This article has been cited by | | 1 |
Establishment of two-dimensional gel electrophoresis profiles of the human acute promyelocytic leukemia cell line NB4 |
|
| He, P. and Liu, Y. and Zhang, M. and Wang, X. and Wang, H. and Xi, J. and Wei, K. and Wang, H. and Zhao, J. | | Molecular Medicine Reports. 2012; 6(3): 570-574 | | [Pubmed] | |
|
|
|
|