|
 
 |
|
ORIGINAL ARTICLE |
|
|
|
| Year : 2012 | Volume
: 18
| Issue : 2 | Page : 167-171 |
| |
Prevalence and hematological profile of β-thalassemia and sickle cell anemia in four communities of Surat city
Dipal S Bhukhanvala, Smita M Sorathiya, Avani P Shah, Ankur G Patel, Snehalata C Gupte
Surat Raktadan Kendra and Research Centre (NABH Accredited Regional Blood Transfusion Centre), Surat, India
| Date of Web Publication | 8-Sep-2012 |
Correspondence Address:
Snehalata C Gupte
Director, Surat Raktadan Kendra and Research Centre, 1st Floor, Khatodara Health Centre, Besides Chosath Joganiyo Mata’s Temple, Udhana Magdalla Road, Khatodara, Surat – 394 210
India
 Source of Support: None, Conflict of Interest: None  | 3 |
DOI: 10.4103/0971-6866.100752

 Abstract Abstract | | |
Background: From the data of transfusion-dependent thalassemia major cases, the 4 communities (Muslim, Dhodia Patel, Kachhiya Patel, and Modh Bania) with high prevalence but not studied methodically were selected.
Aim: The aim of this study is to find prevalence of β-thalassemia and sickle cell anemia in 4 selected communities and also to evaluate hematological profile in them.
Materials and Methods: For screening of β-thalassemia trait (BTT) and sickle cell trait (SCT), all samples were tested for red cell indices, solubility, HbA 2 level and doubtful cases confirmed on HPLC.
Statistical Analysis: Mean ± SD, χ2 and 't' tests were used to evaluate the significance.
Results and Conclusion: Among 4 selected communities, the highest prevalence of BTT was observed in Modh Bania (6.2%) and Kachhiya Patel (6.05%) and that of SCT in Dhodia Patel (14.0%). Significantly higher prevalence of BTT was observed in Memon ( P < 0.0001) and of SCT in Khalifa 6.6% ( P < 0.0001) compared to other Muslim sub castes. Anemia was more prevalent in BTT compared to non-BTT and non-SCT subjects. 80% of Dhodia Patel non-BTT and non-SCT subjects showed microcytic red cell morphology. Their Mean ± SD Hb concentration was 12.1 ± 1.73, hence iron deficiency cannot be a sole reason. This community needs α-thalassemia and iron studies.
Keywords: β-thalassemia trait, Dhodia Patel, Kachhiya Patel, Modh Bania, Muslim, sickle cell trait, Surat
How to cite this article:
Bhukhanvala DS, Sorathiya SM, Shah AP, Patel AG, Gupte SC. Prevalence and hematological profile of β-thalassemia and sickle cell anemia in four communities of Surat city. Indian J Hum Genet 2012;18:167-71 |
How to cite this URL:
Bhukhanvala DS, Sorathiya SM, Shah AP, Patel AG, Gupte SC. Prevalence and hematological profile of β-thalassemia and sickle cell anemia in four communities of Surat city. Indian J Hum Genet [serial online] 2012 [cited 2016 Jun 1];18:167-71. Available from: http://www.ijhg.com/text.asp?2012/18/2/167/100752 |
| Introduction | |  |
The distribution of β-thalassemia and sickle cell disorders varies geographically and from community to community. Various hemogloginopathies are major public health problem in Gujarat, but the data pertaining to their occurrence and prevalence, especially in Surat, are scarce. According to the census of India Report 2001 (Surat Municipal Corporation), the population of Surat district is 4,995,174; in rural region, it is 1,999,357 and in urban area, it is 2,995,817. Surat has cosmopolitan population, and several communities are living in the district from centuries. Gujarati community dominates and others are Marwaris, Punjabis, Marathi, and Hindi speaking north Indian population. The analysis of transfusion-dependent thalassemia major cases, attending our center, had suggested that there is a high prevalence in Muslims, Patels, Sindhis, Modh Banias, and Mahayavanshi. The sickle cell disease (SCD) was predominantly found in Dhodia Patels, Kolis, and Gamits.
Muslims are divided into 2 major religious, endogamous sects - Shia and Sunni, and several castes like Momins, Memon, Khoja, Bohra, Pathan, Sayied, Shaikh etc. are found in them. As many Muslim sub-castes originate from different geographical locations, this community was selected. This study includes only Sunni Muslims who follow the trend of consanguineous marriages.
Certain sub-castes of Patel [1] and tribal communities are already studied for sickle cell disorders. [2],[3],[4] Dhodia Patel, the third largest tribal group in Gujarat, needs β-thalassemia studies as thalassemia major cases are identified in this community. The majority of them are settled in Surat and Valsad districts, but they are also found in Daman and Diu, Dadra and Nagar Haveli, Madhya Pradesh, Maharashtra, Karnataka, Rajasthan states.
There are no studies on Modh Bania and Kachhia Patel communities of Surat. They originate from town Modhera in Patan district in the northern part of Gujarat. They are predominantly Brahmins or Banias, and those who migrated to Surat are known as Surti Modh Banias or Ghanchi. Majority of Kachhiya Patels are vegetable vendors and cultivators and are basically Kadva Patels. They are inhabitants of Ahmedabad, Surat, Anand, and Khambhat cities in Gujarat.
| Materials and Methods | | |
The study was approved by the institutional ethics committee. As a control, 24,917 randomly selected unrelated individuals including all major castes, attending hemoglobinopathies screening camps organized in different locations (school and colleges) in Surat were screened. Total 9,447 samples of selected communities were collected during functions after taking permission from their leaders.
The informed consent in local language was taken, and then, 2 ml blood was collected in EDTA. All the samples were tested for red blood cell indices by an automated cell counter MEK-5216K (NIHON KOHDEN, Japan), [5] solubility test, [6] and cellulose acetate electrophoresis at pH 8.9. [7] The samples showing HbA 2 >3.5% were initially diagnosed as β-thalassemia trait (BTT). The doubtful cases and all traits were confirmed by high performance liquid chromatography (HPLC) on Hemoglobin Variant Testing System, BioRad Laboratories. [8],[9] Statistical evaluation of the data was done by mean ± standard deviation (SD), χ2 , and 't' tests.
| Results | | |
Among 9,447 study participants, 4,870 were Muslims, 2,249 Modh Bania, 1,173 Kachhiya Patel, and 1155 were Dhodia Patel. Sex- and age-wise analysis of the 9,447 subjects showed that 5,385 (57.0%) were male and 4,062 (42.9%) were female having average age 23.0 ± 15.1 years. In control group, 12,970 were male and 11,947 female and had average age of 17.8 ± 2.61 years.
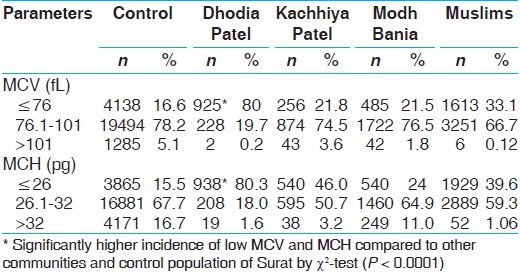
The mean cell volume (MCV) ≤76 fl and mean cell hemoglobin (MCH) ≤26 values suggest BTT. [5] MCV ≤76 fl was observed in 80.0% Dhodia Patel, 33.1% Muslims, 21.8% in Kachhiya Patel, 21.5% Modh Bania, and 16.6% in control population [Table 1]. In Dhodia Patel, incidence of low MCV was significantly higher compared to control population (χ2 = 72, P0 < 0.0001). The MCH value of ≤26 value was observed in 80.3% Dhodia Patel, 46.0% in Kachhiya Patel, 39.6% in Muslims, 24.0% in Modh Bania, and 15.5% in Control population. In Dhodia Patel, significantly more subjects were having MCH ≤26 pg compared to control population (χ2 = 72, P < 0.0001).
The overall prevalence of BTT and SCT in Surat population (control) was 3.2% and 1.38%, respectively [Table 2]. The significantly higher prevalence of BTT was observed in Modh Bania and Kachhia compared to remaining communities and control population of Surat by χ2 -test ( P < 0.0001). Dhodia Patels had significantly higher prevalence of SCT ( P < 0.0001).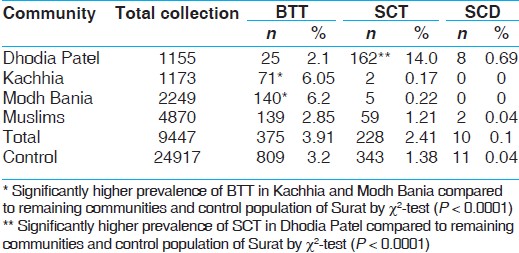 | Table 2: Prevalence of β-thalassemia trait and sickle cell trait in study population
Click here to view |
[Table 3] shows prevalence of BTT and SCT in different Muslims sub-castes. Significantly higher prevalence of BTT is observed in Memon (χ2 = 23.8, P < 0.0001) and of SCT in Khalifa (χ2 = 72, P < 0.0001) compared to other Muslim sub-castes. 4 samples of Muslim community had borderline HbA 2 values.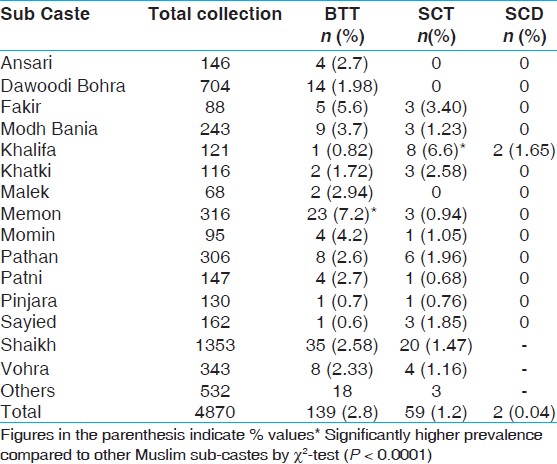 | Table 3: Prevalence of β-thalassemia and sickle cell trait in Muslim sub-castes
Click here to view |
[Table 4] shows highly significant ( P < 0.001) differences in hematological parameters of non-BTT/non-SCT study subjects. In Dhodia Patel, the mean MCV (69.8 ± 8.35) and MCH (23.6 ± 2.03) are significantly lower and RBC (5.24 ± 0.73) values are raised compared to control population. Kachhiya Patels have reduced mean cell hemoglobin concentration (MCHC) (30.82 ± 1.4).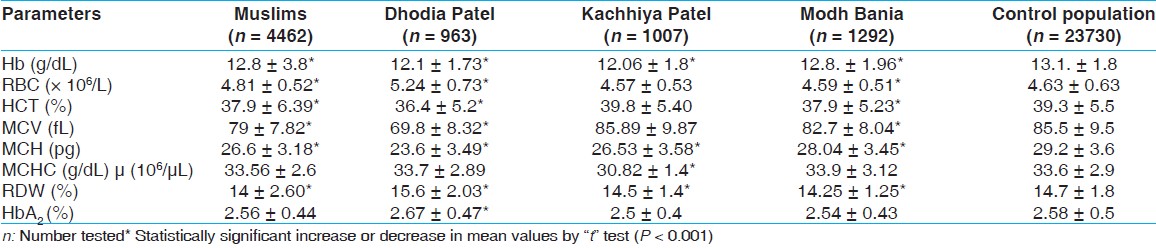 | Table 4: Hematological data (mean ± S.D.) of non-β-thalassemia trait/non-sickle cell trait selected caste groups and control population
Click here to view |
Selected communities and control population showed significantly low values of hemoglobin (Hb) in BTT/SCT subjects compared to non-BTT/non-SCT individuals. As seen in [Table 5], anemia is predominant in Kachhiya Patel BTT subjects, and they also have significantly reduced MCH (18.9 ± 2.9), MCHC (29.18 ± 1.61), compared to control population by " t" test ( P < 0.001). Muslim BTT subjects have lowest values of MCV and RDW compared to control population by " t" test ( P < 0.001).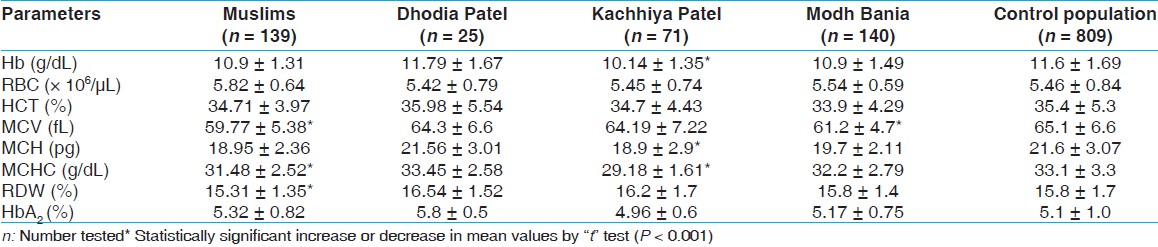 | Table 5: Hematological data (mean ± S.D.) of β-thalassemia trait subjects
Click here to view |
[Table 6] shows the significant reduction in MCV, MCH, and Hb S in Dhodia Patel SCT subjects compared to Muslims and control ( P < 0.001).
Comparison of Hb and HCT in control, BTT, and SCT population shows that anemia is more prevalent in BTT compared to non-BTT/non-SCT subjects.
| Discussion | | |
The first step in population screening for thalassemia trait is the accurate complete blood count. As per Dacie and Lewis, [5] MCV ≤76 fL and MCH ≤26 pg indicate possibility of BTT and should be further screened for HbA 2 level. In our study, majority (80%) of Dhodia Patel samples showed reduced MCV and MCH, but cellulose acetate membrane electrophoresis and HPLC confirmed BTT only in 2.1% subjects [Table 2]. Red blood cell indices are also low in α-thalassemia trait and iron deficiency. [10] In India, because of the high prevalence of iron-deficiency anemia, differential diagnosis of BTT is often complicated. Mehta and Pandya [11] have suggested that the BTT individuals have an advantage in maintaining an iron balance. The mean ± SD Hb concentration in non-BTT/non-SCT Dhodia Patel individuals was 12.1 ± 1.73; hence, iron deficiency may not be present in all those having low indices. However, iron deficiency and α-thalassemia studies are essential for this community to explain reasons for low RBC indices.
An increased HbA 2 level (>3.5%) is the hallmark of diagnosis of β-thalassemia carriers. Samples with borderline HbA 2 probably due to silent mutation, co-inheritance of δ and β thalassemia, some mild β-gene mutations, and γδβ-thalassemia should be repeated on HPLC and may be analyzed by molecular methods. [12] In this study, 4 such samples of Muslims community were found, which need to be further confirmed by molecular analysis. Studies in different Indian regions have reported 1% to 17% prevalence of BTT with mean of about 3.3%. [13],[14] Comparable prevalence of 3.2% of BTT was found in Surat population selected as control. Madan et al.[15] in ICMR multi-center study reported 2.68% BTT prevalence in Mumbai and 5.47% in Delhi. They found 2.7% BTT in Baniya and 2.5% and 1.7% BTT in Sunni Muslims from Mumbai and Delhi, respectively. [15] While in our study, we found 6.2% BTT prevalence in Modh Bania and 2.85% in Muslims. This is the first report on the prevalence of β-thalassemia in Kachhiya Patel community.
Hb AS has been reported as 0% to 31.4% in tribal population of Gujarat. [2] Different non-tribal caste groups are also known to have sickle gene. [16],[17] In our study, the prevalence of SCT was 14.0% in Dhodia Patel (tribal community). Earlier studies have reported 13.76% and 17.84% prevalence in this community, in Valsad and Surat respectively. [2] Mukherjee et al.[3] reported the lower Hb S level (27.9%) in tribal compared to the non -tribal group (35.5%). They also reported very high frequency of α-thalassemia gene in tribal (0.97) compared to the non-tribal (0.24). We found similar results in Dhodia Patel with reduced Hb S level (27.9 ± 3.4) compared to Muslims (34.02 ± 4.2) and control (31.2 ± 5.8). Very high incidence of reduced RBC indices in Dhodia Patel indicates the possibility of α-thalassemia gene in this tribe.
Compared to normal (negative for BTT or SCT) subjects, Hb and hematocrit values were significantly lower in BTT subjects. The ICMR study [15] has also detected more anemic children in BTT series compared to children without any hemoglobinopathy.
| Conclusion | | |
BTT prevalence is higher in Modh Bania and Kachhiya Patel, and higher SCT prevalence is observed in Dhodia Patel, Memon, and Khalifa. As majority of Dhodia Patels show microcytic red cell morphology, this community also needs α-thalassemia and iron study.
| Acknowledgement | | |
We thank the leaders of Dhodia Patel, Muslim, Kachhiya Patel and Modh Bania communities for their support in organizing camps for thalassemia and sickle cell anemia. The financial assistance from Surat Raktadan Kendra and Research Centre management is gratefully acknowledged. The equipment like HPLC and hematology analyzer received from the grant given by Lions club International Fund is thankfully acknowledged.
| References | | |
| 1. | Varawalla NY, Old JM, Sarkar R, Venkatesan R, Weatherall DJ. The spectrum of β-thalassemia mutations on the Indian subcontinent: The basis for prenatal diagnosis. Br J Haematol. 1991;78:242-7. 
|
| 2. | Bhatia HM, Rao VR. Genetic atlas of Indian tribes. Bombay: Institute of Immunohaematology (ICMR) publication; 1986. p. 263-73.
|
| 3. | Mukherjee MB, Lu CY, Ducrocq R, Gangakhedkar R, Colah R, Kadam M, et al. Effect of α-thalassemia on sickle cell anemia linked to the Arab-Indian haplotype in India. Am J Hematol 1997;55:104-9.
|
| 4. | Iyer SR, Iyer RR, Oza GD, Rane RM, Khandwala RM, Desai SD. Sickle cell Syndromes in and around Bardoli. J Assoc Physicians India 1994;42:885-7.
|
| 5. | Dacie JV, Lewis SM. Practical Hematology. 9 th ed. London, UK, Churchill Livingstone; 2001. p. 231-68.
|
| 6. | Huntsman RG, Barclay GP, Canning DM, Yawson GJ. A rapid whole blood solubility test to differentiate the sickle cell trait from sickle cell anemia. J Clin Pathol 1970;23:781-3.
|
| 7. | Graham JL, Grunbaun BW. A rapid method for microeletrophoresis and quantitation of Hb on cellulose acetate. Am J Clin Pathol 1963;39:567-78.
|
| 8. | Joutovsky A, Hazdi-Nesic J, Nardi MA. Retention time as a diagnostic tool for hemoglobin variants and hemoglobinopathies: A study of 60,000 samples in a clinical diagnostic laboratory. Clin Chem 2004;50:1736-47.
|
| 9. | Colah R, Surve R, Sawant P, D'Souza E, Italia K, Phanasgoankar S, et al. HPLC studies in hemoglobinopathies. Indian J Pediatr 2007;74:657-62.
|
| 10. | Eldibany MM, Totonchi KF, Joseph NJ, Rhone D. Usefulness of certain red blood cell indices in diagnosing and differentiating thalassemia trait from iron-deficiency anemia. Am J Clin Pathol 1999;111:676-82.
|
| 11. | Mehta BC, Pandya BG. Iron status of beta thalassemia carriers. Am J Hematol 1987;24:137-41.
|
| 12. | Rathod DA, Kaur A, Patel V, Patel K, Kabrawala R, Patel V, et al. Usefulness of cell counter based parameters and formulas in detection of β thalassemia trait in areas of high prevalence. Am J Clin Pathol 2007;128:585-93.
|
| 13. | Sukumaran PK. Abnormal hemoglobins in India. In: Sen NN, Basu AK, editors. Trends in hematology. Culcutta: Saraswati Press; 1975. p. 225-36.
|
| 14. | Modell B, Petrou M. The problem of the hemoglobinopathies in India. Indian J Hematol 1983;1:5-16.
|
| 15. | Madan N, Sharma S, Sood SK, Colah R, (Late) Bhatia HM. Frequency of β-thalassemia trait and other hemoglobinopathies in northern and western India. Indian J Hum Genet 2010;16:16-25.
[PUBMED]  |
| 16. | Sharma A. Haemoglobinopathies in India. In: ICMR, editor Satyavati GV. Peoples of India: Some genetical aspects. New Delhi: ICMR, New Delhi Publication; 1983. p. 31-49.
|
| 17. | Mohanty D, Mukherjee MB. Sickle cell disease in India. Curr Opin Hematol 2002;9:117-22.
|
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6]
| This article has been cited by | | 1 |
Sickle cell disease in India |
|
| Roshan Colah,Malay Mukherjee,Kanjaksha Ghosh | | Current Opinion in Hematology. 2014; 21(3): 215 | | [Pubmed] | [DOI] | | | 2 |
Molecular characterization of ß-thalassemia in four communities in South Gujarat—codon 30 (G???A) a predominant mutation in the Kachhiya Patel community |
|
| Dipal S. Bhukhanvala,Khushnooma Italia,Pratibha Sawant,Roshan Colah,Kanjaksha Ghosh,Snehalata C. Gupte | | Annals of Hematology. 2013; 92(11): 1473 | | [Pubmed] | [DOI] | | | 3 |
Morbidity pattern of sickle cell disease in India: A single centre perspective |
|
| Tewari, S., Rees, D. | | Indian Journal of Medical Research. 2013; 138: 288-290 | | [Pubmed] | | | 4 |
Micro mapping the frequencies of beta thalassemia and sickle cell anemia in India: A way forward to plan control strategies |
|
| Das, R. | | Indian Journal of Human Genetics. 2012; 18(2): 148-149 | | [Pubmed] | |
|
|
|
|