|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2012 | Volume
: 18
| Issue : 2 | Page : 241-245 |
| |
46,XX, der(15),t(Y;15)(q12;p11) karyotype in an azoospermic male
Serap T Onrat, Zafer Söylemez, Muhsin Elmas
Department of Medical Genetics, Faculty of Medicine, University of Afyon Kocatepe, Afyonkarahisar, Turkey
| Date of Web Publication | 8-Sep-2012 |
Correspondence Address:
Serap T Onrat
Department of Medical Genetics, Faculty of Medicine, University of Afyon Kocatepe, ANS Arastirma Uygulama Hastanesi Morfoloji Binasi, 03200, Afyonkarahisar
Turkey
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.100785

 Abstract Abstract | | |
We report on a Yq/15p translocation in a 23-year-old infertile male referred for Klinefelter Syndrome testing, who had azoospermia and bilateral small testes. Hormonal studies revealed hypergonadotropic hypogonadism. Conventional cytogenetic procedures giemsa trypsin giemsa (GTG) and high resolution banding (HRB) and molecular cytogenetic techniques Fluorescence In Situ Hybridization (FISH) performed on high-resolution lymphocyte chromosomes revealed the karyotype 46,XX, t(Y;15)(q12;p11). SRY-gene was confirmed to be present by classical Polymerase Chain Reaction (PCR) methods. His father carried de novo derivative chromosome 15 [45,X, t(Y;15)(q12;p11)] and was fertile; the karyotype of the father using G-band technique confirmed a reciprocal balanced translocation between chromosome Y and 15. In the proband, the der (15) has been inherited from the father because the mother had a normal karyotype (46,XX). In the proband, the der (15) could have produced genetic imbalance leading to unbalanced robertson translocation between chromosome Y and 15, which might have resulted in azoospermia and infertility in the proband. The paternal translocation might have lead to formation of imbalanced ova, which might be resulted infertility in the proband. Sister's karyotypes was normal (46,XX) while his brother was not analyzed.
Keywords: 46,XX male, azoospermia, Fluorescence In Situ Hybridization, infertility, Yq;15p translocation
How to cite this article:
Onrat ST, Söylemez Z, Elmas M. 46,XX, der(15),t(Y;15)(q12;p11) karyotype in an azoospermic male. Indian J Hum Genet 2012;18:241-5 |
How to cite this URL:
Onrat ST, Söylemez Z, Elmas M. 46,XX, der(15),t(Y;15)(q12;p11) karyotype in an azoospermic male. Indian J Hum Genet [serial online] 2012 [cited 2016 Jun 1];18:241-5. Available from: http://www.ijhg.com/text.asp?2012/18/2/241/100785 |
| Introduction | |  |
Translocations involving the Y and an autosomal chromosome are very rare. That translocation between the heterochromatin of the long arm of chromosome Y (breakpoint at q12) and the short arm of chromosome 15 (breakpoint at p11-13) being the most frequent. [1],[2] This, on the basis of sequence homology, may be the consequence of a frequent association at the pachytene stage of male meiosis of the 15p and Yq heterochromatin. [3]
Yq12 and 15p are located in the heterochromatic region of respective human chromosomes. Some changes in these regions used to be considered as polymorphic variants within a population. Thus, carriers of der(15)t(Y;15)(q12; p11) translocations usually have normal phenotype with unaffected fertility and were usually called variants [4] until it was shown that such carriers could have infertility, repeated spontaneous abortion, stillbirths, or liveborn children with defects. [5],[6]
The frequency of Y/autosome translocations in the general population is approximately 1 in 2000. Hsu (1994) described 130 cases of Y-autosome translocation, with about half (60 out 130) bearing the common translocation of the heterochromatic region (Yq12) onto the short arm of an acrocentric chromosome (13, 14, 15, 21 or 22). These translocation cases can be regarded as interesting variant chromosomes, but they are not associated with any clinical consequence. [7],[8],[9] Like any other chromosome, the Y chromosome can be translocated onto an autosome, an X chromosome or another Y chromosome, either in a balanced or unbalanced way. Translocations between the Y and a non-acrocentric chromosome are rare and may involve any part of the Y chromosome, often leading to an abnormal phenotype and infertility. [10],[11],[12],[13],[14],[15]
We here describe a male with a 46,XX t(Y;15)(q12;p11) chromosomal constitution, normal male phenotype, infertility, and azoospermia. The presence of the SRY gene was confirmed with fluorescent in situ hybridization (FISH). All analyzed STS markers in the AZF region at the Y chromosome were also present.
| Materials and Methods | | |
Clinical Findings
A phenotypically normal 23-year-old male, 170 cm in height, was referred for treatment of infertility due to severe azoospermia. He had been married for two years but could not have children. Semen analysis showed complete absence of spermatozoa, confirming azoospermia. His total semen volume was measured at 3 mL. Physical examination showed a normal sexual development and bilateral small testes with enlarged pampiniform plexus veins. The left testis was 18 × 10 × 16 mm, whereas the right testis was 14 × 10 × 16 mm, and each had a volume of 1.2 and 1.6 cc, respectively. Hormonal studies revealed hypergonadotropic hypogonadism. The round cell and agglutination were negative. Serum FSH level was 9.95 mlU/mL (normal 1.5-12.4 mlU/mL), LH 17.3 mlU/mL (normal 1.7-8.6 mlU/mL), and Testosterone 20.9 ng/dL (normal 286-800 ng/dL). His father and his mother were fertile with three children of whom two were boys and one was a girl.
Cytogenetic Analysis
Chromosomal analysis of peripheral blood lymphocytes was performed according to standard protocols. [16] Peripheral blood (2 mL) was collected in heparin vacutainers (Becton Dickinson, Franklin Lakes, NJ, USA). Cytogenetic studies were carried out on the proband, his parents, his brother, and his sister. Because his brother was on antibiotics use, metaphase could not be obtained. For cytogenetic analysis, whole blood (0.5 mL) cultures were set up in 5 mL Roswell Park Memorial Institute (RPMI) 1640 media (GIBCO BRL, Grand Island, NY, USA) containing 15% fetal calf serum (Biological Industries, KBH, Kibbutz Bet-Haemek, Israel), antibiotic mixture and phytohemagglutinin P (DIFCO Lab, Maryland, USA) for 72 h. Chromosome preparations were obtained from lymphocyte cultures and analyzed after Giemsa-Trypsin-Giemsa (GTG)-banding. [17] For karyotyping, at least 20 metaphases were analyzed, and for karyotypes of suspected mosaicism, 50 cells were counted. The karyotypes were interpreted using the recommendation of the International System for Human Cytogenetic Nomenclature. [18]
Karyotyping and Fluorescence in situ Hybridization
High-resolution chromosomal GTG banding was performed on cultured, Phytohemagglutinin (PHA)-stimulated peripheral blood lymphocytes, according to standard cytogenetic procedures. FISH followed manufacturer's instructions, using centromeric probes for chromosomes CEP 18/X/Y alpha satellite (D18Z1, DXZ1 and DYZ3, 18p11.1-q11.1, Xp11.1-q11.1, Yp11.1-q11.1;Vysis), a SRY-specific probe (SRY, Yp11.3; Vysis) and CEP 15. The slides were analyzed by two independent observers using an Olympus BX50 (Olympus Optical Co.,Ltd., Tokyo, Japan) fluorescence microscope equipped with a filter set for FITC, Texas Red, Aqua and DAPI/Texas, Red/FITC. Normal male lymphocyte preparations were used as controls for the FISH assays.
PCR Amplification for SRY and AZF Regions
Peripheral blood samples (8-10 mL) were pelleted and stored at −20°C until DNA extraction. The patient was screened for Yq11.2 chromosome microdeletions in the AZF regions by classical PCR using STS markers (AZFa: sY81, sY82, sY84; AZFb: sY127, sY142, sY164; AZFc: cdy, bpy2, sY255, sY254, sY277, rbm1). SRY (Yp) was used as an internal positive control. Negative controls included normal male and female DNA and classical PCR reaction with no DNA added.
| Results | | |
In this study, we describe a (Yq;15p) translocation found in a 23-year-old man with azoospermia and infertility referred for Klinefelter Syndrome testing. We have made use of classical PCR and in situ hybridization using Y chromosome-specific probes to characterize a t(Y;15) segregating in a family. In situ hybridization and cytogenetics analyses showed a 46,X,t(Y;15)(q12;p11) karyotype in the fertile father and 46,XX,t(Y;15)(q12;p11) karyotype in his infertile son. The STS analyses for the presence of Y-chromosome microdeletion showed an intact AZF region [Table 1] and FISH results showed the presence of SRY gene. Thus, the present report describes an azoospermic male exhibiting an abnormal karyotype with translocation between chromosome Yq12 and 15p that causes infertility.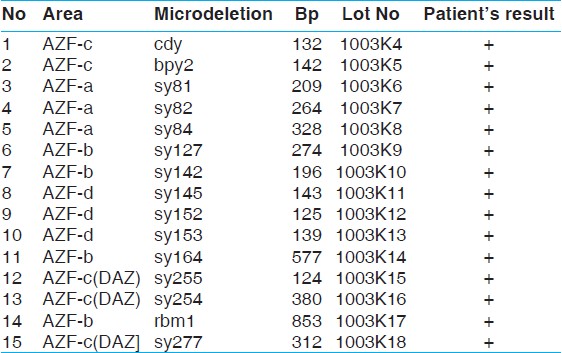 | Table 1: The results of patient's Y chromosome microdeletion test for determining AZF regions
Click here to view |
In all 30 observed metaphases from the patient and his family members, GTG banding showed that the entire Y chromosome was translocated onto a chromosome 15, with breakpoints on their short arms. His karyotype was 46,XX,der(15),t(Y;15), his mother's was 46,XX, and his father's was 45,X der(15)t(Y;15) [Figure 1]. G banded karyotype showing the der(15) (arrow) in the father and patient's karyotype is shown in [Figure 1]. An apparently identical der(15) was observed in the proband and his father. It was not p resent in the paternal grandmother, while the grandfather was deceased.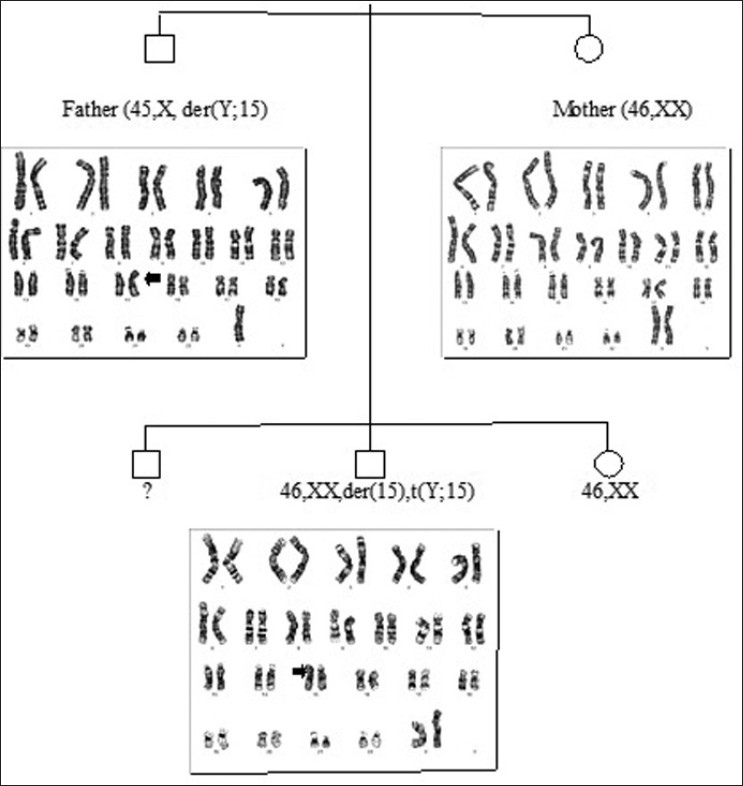 | Figure 1: In G banded karyotype, the der(15) (arrow) in the father and our patient were seen. His mother and sister have normal karyotype. His brother karyotype could not determined and he did not accept giving blood sample for detecting karyotype
Click here to view |
FISH analysis with centromeric probes for chromosomes 18/X/Y [Figure 2] confirmed the presence of two X chromosomes and one Y chromosome. The intact SRY locus on the Yp arm showed that the Yp11.2 region was present [Figure 3], as were also the telomeric specific regions of both arms of the sex chromosomes. Hybridization with a pantelomeric repeat probe showed that the Y and 15 chromosomes had lost their p arms-telomeres, thus defining the breakpoint on the Yp11.32 band. In the control slides of the FISH procedure, 95-98% of the cells gave correct hybridization signals for each of the probes used.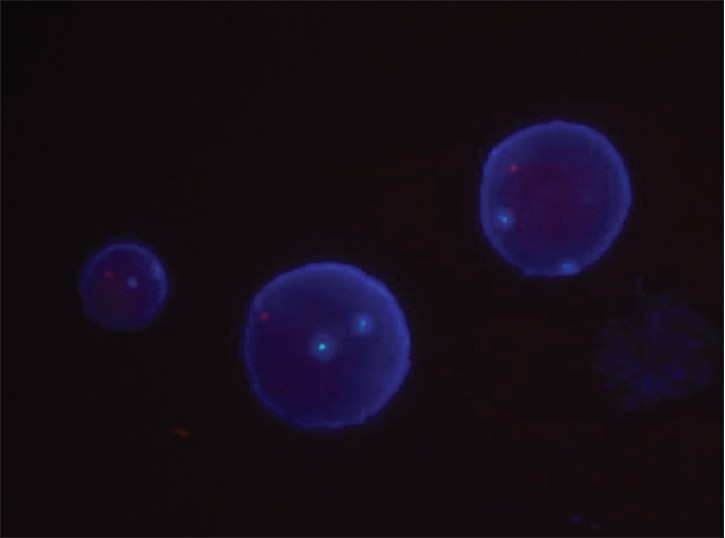 | Figure 2: Spectrum Aqua filter set fluorhopore-labeled alpha satellite DNA 18 probe, Spectrum Green probelabeled alpha satellite DNA X probe and Spectrum Orange probe-labeled alpha satellite DNA Y probe. We used DAPI/Orange/Green Filter set for enumeration to CEP X Spectrum Green/CEP Y Spectrum Orange. Fluorescent in situ hybridization (FISH) result showed that there were two chromosomes X and one Y chromosomes
Click here to view |
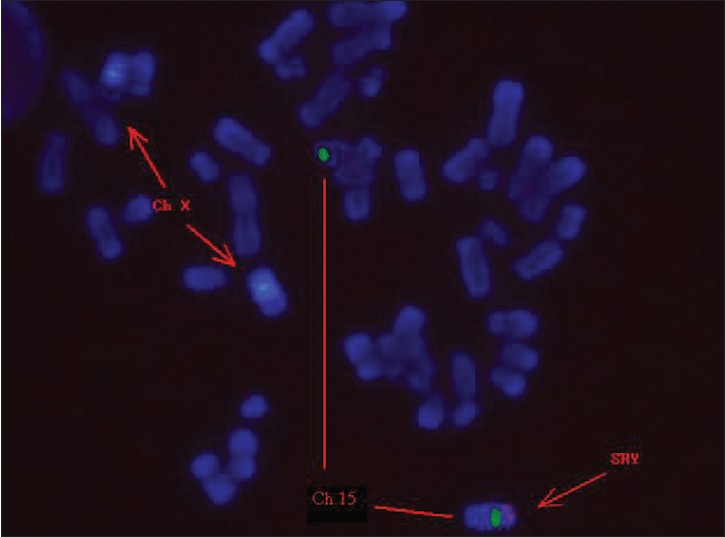 | Figure 3: Fluorescence in situ hybridization on metaphase chromosomes using CEP X/SRY specific probes. Arrows indicate two X chromosome centromeric signals (blue) and one SRY specific signal (red) on the ends of chromosome 15. Fluorescent in situ hybridization (FISH) shows fluorescence illumination of the long arm of the Y chromosome and the short arm (q11 of the Y chromosome) of the derivative chromosome 15. The images were obtained separately and were captured. FISH result showed that there were two chromosomes X and one derived chromosome 15 contained Yq11.1 signals in peripheral blood lymphocyte from the patient.
Click here to view |
| Discussion | | |
Approximately 15% of couples in the reproductive age worldwide are affected by infertility, and it is estimated that about 40-50% of infertilities are of male origin. Genetic factor accounts for 10-15% of severe male infertility, including chromosomal aberrations and single gene mutations. [19]
Different studies demonstrated that 46,XX infertile males have low testosterone levels, normal or elevated FSH and LH levels, and different variants of a phenotype, including small penis, hypospadias, cryptorchidism, flat scrotum, and small testes. [20] In the majority of XX males the SRY gene is positive. Most men are diagnosed in adulthood due to infertility caused by azoospermia. [21]
The association of t(Y;15)(q12;p11) translocations with reproductive abnormalities is still controversial. Most of carriers are fertile, so this karyotype used to be considered as a variant. However, some carriers had history of infertility, abortion, or abnormal phenotypes. [22] Translocations involving gonosomes are rare and are frequently associated with severe male infertility. [23] Brisset et al. (2005) also reviewed reciprocal translocations involving the Yq11 region. All 12 men reported with such rearrangements were infertile. In three cases, molecular analysis of the long arm was performed and no deletion was observed, confirming the leading role of the translocation in failure of spermatogenesis rather than any deletion. [24] In our case; although adult and fertile de novo balanced translocation carrier (the patient's father) has a 45,X, t(Y;15)(q12;p11) karyotype, unbalanced translocation carrier proband has a 46,XX, t(Y;15)(q12;p11) karyotype and he is infertile.
Most Y chromosome/autosome translocations diagnosed by means of routine analysis involve the heterochromatic portion of the Y chromosome. [25] Two distinctly different types of translocations occur. In the more common form, the distal portion of Yq is translocated to the short arm of an acrocentric chromosome. Those forms in which the Y material is translocated onto a non- acrocentric chromosome are much rarer and may involve any part of the Y chromosome. [25],[26] Translocations belonging to the first group, most commonly t(Y;15), have been seen in normal individuals and are therefore thought to be compatible with a normal phenotype including fertility. [27],[28] Translocations of the second type often lead to an abnormal phenotype, notably including sterility. [29]
Translocation to between in Y chromosome and the acrocentric chromosomes should be examined in more detail for the effects of azoospermia. Our study can be used as the data on this issue.
| References | | |
| 1. | Alitalo T, Tiihonen J, Hakola P, la Chapelle A. A Molecular characterization of a Y;15 translocation seggregating in a family. Hum Genet 1988;79:29-35. 
[PUBMED] |
| 2. | Powell C. Sex chromosomes and sex abnormalities. In: Gersen GL, Keagle MB, editors. The principles of clinical cytogenetics. Totowa, NJ: Humana Press; 1999. p. 229-58.
|
| 3. | Metzler-Guillemain C, Mignon C, Depetris D, Guichaoua MR, Mattei MG. Bivalent 15 regularly associates with the sex vesicle in normal male meiosis. Chromosome Res 1999;7:369-78.
[PUBMED] |
| 4. | Neumann A, Robson L, Smith A. A 15p variant shown to be a t(Y;15) with fluorescence in situ hybridization. Ann Genet 1992;5:227-30.
|
| 5. | Fukada Y, Yasumizu T, Amemiya A, Kohno K, Takizawa M, Hoshi K, et al. Prenatal confirmation of the translocation between chromosome 15 and Y-chromosome by fluorescence in situ hybridization. Tohoku J Exp Med 1999;187:285-9.
|
| 6. | Rajcan-Separovic E, Robinson WP, Stephenson M, Arbour L, McFadden D, Guscott J, et al. Recurrent trisomy 15 in a female carrier of der(15)t(Y;1)(q12;p13). Am J Med Genet 2001;99:320-4.
|
| 7. | Nielsen J, Rasmussen K. Y/autosomal translocations. Clin Genet 1976;9:609-17.
[PUBMED] |
| 8. | Gardner RJ, Sutherland GR. Chromosome abnormalities and genetic counseling. Sex chromosome translocations. New York, Oxford: Oxford University Press; 1996. p. 95- 114.
|
| 9. | Smith A, Fraser IS, Elliot G. An infertile man with balanced Y;19 translocation. Review of Y; autosome translocations. Ann Genet 1979;22:189-94.
|
| 10. | Delobel B, Djlelati R, Gabriel-Robez O, Croquette MF, Rousseaux-Prevost R, Rousseaux J, et al. Y-autosome translocation and infertility: Usefulness of molecular, cytogenetic and meiotic studies. Hum Genet 1998;102:98- 102.
|
| 11. | Goodfellow P, Darling S, Wolfe J. The human Y chromosome. J Med Genet 1985;22:324-44.
[PUBMED] |
| 12. | Vogt PH, Edelmann A, Kirsch S. Human Y chromosome azoospermia factors (AZF) mapped to different subregions in Yq11. Hum Mol Genet 1996;5:933-43.
|
| 13. | Vogt PH. Y chromosome and single gene deffects that cause male infertility. In: Jansen R, Mortimer D, editors. Towards reproductive certainty: Fertility and genetics beyond 1999. Carnforth, UK: Parthenon; 1999. p. 298-312.
[PUBMED] |
| 14. | Viguié F, Romani F, Dadoune JR. Male infertility in a case of (Y;6) balanced reciprocal translocation. Hum Genet 1982;62:225-7.
|
| 15. | Hsu LY. Phenotype/karyotype correlations of Y chromosome aneuploidy with emphasis on structural aberrations in postnatally diagnosed cases. Am J Med Genet 1994;53:108-40.
|
| 16. | Moorhead PS, Nowell PC, Mellman WJ. Chromosome preparations of leukocytes cultured from human peripheral blood. Exp Cell Res 1960;20: 613-6.
|
| 17. | Seabright M. A rapid banding technique for human chromosomes. Lancet 1971;2:971-2.
|
| 18. | Shaffer LG, Tommerup N. An international system for human cytogenetic nomenclature. Karger Farmington ISBN 3-8055-8019-3, VI + 128 p. plus foldout, 11 [Figure 4] tab., soft cover, 2005.
|
| 19. | Ferlin A, Arredi B, Foresta C. Genetic causes of male infertility. Reprod Toxicol, 2006;22:133-41.
|
| 20. | Castineyra G, Copelli S, Levalle O. 46,XX Male: Clinical, hormonal/genetic findings. Arch Androl 2002;48:251-7.
|
| 21. | de la Chapelle A. The etiology of maleness in XX men. Hum Genet 1981;58:105-16. doi:10.1007/BF00284157.
|
| 22. | Chen Y, Chen G, Lian Y, Gao X, Huang J, Qiao J, et al. Genetic characterization of two 46,XX males without gonadal ambiguities. J Assist Reprod Genet 2008;25:547- 52. DOI 10.1007/s10815-008-9265-7.
|
| 23. | Van Assche E, Bonduelle M, Tournaye H, Joris H, Verheyen G, Devroey P, et al. Cytogenetics of infertile men. Hum Reprod 1996;11 (Suppl. 4):1-24; discussion 25-6.
|
| 24. | Brisset S, Izard V, Misrahi M, Aboura A, Madoux S, Ferlicot S, et al. Cytogenetic, molecular and testicular tissue studies in an infertile 45, X male carrying an unbalanced (Y;22) translocation: Case report. Hum Reprod 2005;20:2168-72.
|
| 25. | Li JH, Huang TH, Jiang XW, Xie QD. 46, XX Male sex reversal syndrome. Asian J Androl 2004;6:165-7.
|
| 26. | Kaur A, Sachdeva K, Mahajan S, Virk SPS, Singh JR. An SRY-positive 46,XX male. Balkan J Med Genet 2007;10:1:51-2.
|
| 27. | Rego A, Margarit E, Estivill X, Regal M, García-Mayor RV. Development in a 46 XX boy with positive SRY gene. J Pediatr Endocrinol Metab 1996;9:623-6.
|
| 28. | Spence JE, Perciaccante RG, Greig GM, Willard HF, Ledbetter DH, Hejtmack JF, et al. Uniparental disomy as a mechanism for human disease. Am J Hum Genet 1988;42:217-26.
|
| 29. | White LM, Treat K, Leff A, Styers D, Mitchell M, Knoll JH, et al. Exclusion of uniparental inheritance of chromosome 15 in a fetus with a familial dicentric (Y;15) translocation. Prenatal Dýagnosýs 1998;18:111-6.
|
[Figure 1], [Figure 2], [Figure 3]
[Table 1]
|









