|
 
 |
|
ORIGINAL ARTICLE |
|
|
|
| Year : 2012 | Volume
: 18
| Issue : 3 | Page : 285-289 |
| |
Evaluation of C677T polymorphism of the methylenetetra hydrofolate reductase gene and its association with levels of serum homocysteine, folate, and vitamin B12 as maternal risk factors for Down syndrome
Pankaj K Mohanty, Seema Kapoor, Anand P Dubey, Sanjeev Pandey, Renuka Shah, Hemant K Nayak, Sunil K Polipalli
Department of Pediatrics, LNJP, MAMC, New Delhi, India
| Date of Web Publication | 4-Mar-2013 |
Correspondence Address:
Pankaj K Mohanty
Department of Pediatrics, LNJP, MAMC, New Delhi - 110 002
India
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/0971-6866.107977

 Abstract Abstract | | |
Aims and Objective: Evaluation of C677T polymorphisms of the methylenetetra hydrofolate reductase (MTHFR) gene and its association with level of serum homocysteine, folate, and vitamin B12 as possible maternal risk factors for Down syndrome.
Design: This was a case-control study.
Material and Methods : Fifty-two mothers (mean age 27.6 years) with babies having free trisomy 21 of North Indian ethnicity and 52 control nonlactating mothers (mean age 24.9 years) of same ethnicity attending services of genetic lab for bloodletting for other causes were enrolled after informed written consent. Fasting blood was collected and was used for determination of plasma homocysteine, vitamin B12, and folate (serum and RBC), and for PCR amplification of the MTHFR gene.
Results: The prevalence of MTHFR C677T polymorphism in north Indian mothers of babies with trisomy 21 Down syndrome was 15.38% compared to 5.88 % in controls. The difference between two groups was not statistically significant ( P = 0.124). Low serum folate was demonstrated in 34.62% of cases vs. 11.54% in controls, which was significant ( P = 0.005). Low RBC folate was found in 30.7% of cases versus 11.53% in controls, which was not significant ( P = 0.059), when analyzed independently. But on multiple regression analysis the difference was statistically significant. Low serum vitamin B12 was found in 42.31% of cases versus 34.62% in controls, which was not significant ( P = 0.118). The mean serum homocysteine in cases was 10.35 ± 0.68 while controls were 9.02 ± 0.535.
Conclusion: Serum levels of folate were low in cases. The RBC folate levels were comparable in both groups. However the combined serum folate and RBC folate were low in cases compared to control groups. Homocysteine levels in our study were higher in Down syndrome mothers compared to controls; however high-serum level of Homocysteine had no association with MTHFR polymorphism. No association of serum vitamin B12 with MTHFR polymorphism in occurrence of Down syndrome births was found. Peri- or preconceptional folate supplementation may therefore lead to a decline in DS births, if supported by larger studies.
Keywords: Down syndrome, methylenetetra hydrofolate reductase gene, serum and RBC folate, serum homocysteine, serum vitamin B12
How to cite this article:
Mohanty PK, Kapoor S, Dubey AP, Pandey S, Shah R, Nayak HK, Polipalli SK. Evaluation of C677T polymorphism of the methylenetetra hydrofolate reductase gene and its association with levels of serum homocysteine, folate, and vitamin B12 as maternal risk factors for Down syndrome. Indian J Hum Genet 2012;18:285-9 |
How to cite this URL:
Mohanty PK, Kapoor S, Dubey AP, Pandey S, Shah R, Nayak HK, Polipalli SK. Evaluation of C677T polymorphism of the methylenetetra hydrofolate reductase gene and its association with levels of serum homocysteine, folate, and vitamin B12 as maternal risk factors for Down syndrome. Indian J Hum Genet [serial online] 2012 [cited 2016 Jun 1];18:285-9. Available from: http://www.ijhg.com/text.asp?2012/18/3/285/107977 |
| Introduction | |  |
Trisomy 21 Down syndrome (T21DS) is the most common aneuploidy at birth and the most common genetic cause of mental retardation. It results from the gene expression of an extra chromosome 21, which occurs due to failure of normal chromosomal segregation during meiosis. [1] Eighty percent of these are lost during pregnancy [2] with the birth frequency of 1: 700-1: 1000. [3],[4] In addition to the maternal age which is an important risk factor, identification of the mechanistic basis for T21 requires an understanding of the cellular-molecular events and other biochemical pathways that could promote maternal meiotic nondisjunction. [3] DNA hypomethylation, abnormal gene expression, and abnormal chromosomal segregation occur as a consequence of folate deficiency. [4] The prime function of folate (Vit B 11 ) is to provide one-carbon moieties for the synthesis of three of the four bases of DNA, i.e., guanine, adenine, thymine as well as for the synthesis of methionine and S-adenosyl methionine (SAM) for essential methylation reactions including DNA methylation. Folate deficiency (RBC folate level <160 ng/ml) can be best diagnosed by determination of the RBC folate level. [5] The RBC folate level is not affected by recent folate intake by food and is indicative of the remote folate status of an individual. Homocysteine, small sulfur containing amino acid generates methyl groups for all kinds of transmethylation reaction including DNA methylation which is essential for life. This study attempted to document the association of the levels of homocysteine which may reflect altered folate status and MTHFR C677T polymorphisms as risk factors for Down's syndrome in North Indian mothers. We also studied vitamin B12 and RBC folate leading to delineation of the causes of hyperhomocysteinemia if any.
The association of the C677T polymorphism of the MTHFR gene has been studied in Indian Gujrati mothers and East Indian mothers by Rai, et al.[6] and Seth, et al.[7] respectively. Both reported a significant correlation with homozygous TT genotype. However, its simultaneous correlation with the biochemical parameters in the Indian subcontinent has not been investigated so far. The practice implications of these findings may answer the intriguing question as to whether folic acid supplementation in women around conception can be effective in reducing risk of Down's syndrome.
| Material and Methods | | |
This case-control study was conducted in Department of Paediatrics and Microbiology in Maulana Azad Medical College and associated Lok Nayak Hospital, New Delhi from February 2008 to January 2009. Fifty-two Down syndrome cases were enrolled along with their mothers. Fifty-two controls were taken who were voluntary nonlactating mothers attending genetic clinic for any other cause. Proper informed consent was taken before enrolling the cases and control study group. Children diagnosed as Down syndrome up to age of 18 years were included along with their mothers. Children with the translocation karyotype, mothers taking food supplements or vitamins with fortified food were excluded from the study. Control mothers with children with any known single gene disorder, chromosomal abnormality or syndrome were also excluded.
Seven milliliters of blood was collected from mothers in fasting state. Five milliliter aliquots each was used for plasma homocysteine, vitamin B12, and folic acid and 2 ml for PCR amplification for the MTHFR gene in our study. Another 5 ml was collected from the child with Down syndrome for karyotyping and thyroid function tests. Plasma homocysteine was measured from the mother's blood using the ELISA technique by Bio-Rad kits with external quality control in Genetic Laboratory of Lok Nayak Hospital. RBC folate was measured by using the Elecsys Folate ll assay. For calculating the folate concentration in erythrocyte, the dilution factor and the hematocrit value were taken into account.
Vitamin B12 was also analyzed using electrochemiluminescence using ROCHE kits. Genomic DNA was extracted by the salt extraction method in Genetic Laboratory. The genomic DNA was amplified by polymerase chain reaction and the results were further confirmed by polyacrylamide gel electrophoresis. A control band of 198 bp was normally obtained; heterozygotes had fragments of 178 and 20 and homozygotes had a fragment of 178 kb only. A value serum homocysteine >15 μmol/l was considered as hyperhomocysteinemia
Statistical analysis
Results of continuous data, e.g., serum homocysteine, serum folate, serum vitamin B12, were expressed as Means ± SEM. Comparisons of percentages between groups were performed with a one-sided Chi-square test corrected for continuity. The odds ratio for having a child affected by trisomy 21 was estimated for homozygous, heterozygous or absence of above-mentioned MTHFR polymorphism and regression analysis obtained from interacting variables.
| Results | | |
We found a low value of serum folate (< 3 ng/ml) in 34.62% in cases vs. 11.54% in controls, which was significant (P value 0.005). This actually reflected the recent folate status and may not have had a correlation with folate levels at the time of conception. Abnormal RBC folate levels, an important long-term predictor of folate status (<160 ng/ml), were found in 30.7% of cases versus 11.53% in controls, which was not significant when analyzed independently, however giving an emerging trend (P value 0.059). Low values of serum vitamin B12 levels (<150 μg/l) were found in 42.31% of cases versus 34.62% in controls, which was not significant (P value 0.118). The mean level of homocysteine in cases was 10.35 ± 0.686 while in controls was 9.02 ± 0.535. We found 15.38 % of MTHFR polymorphism (all heterozygous) in cases versus 5.88% in controls, which was not significant (P value 0.124). The regression analysis depicted a significant association of serum folate but not with RBC folate, but the combination of both serum and RBC folate was significant (P value 0.020). The emerging data also highlighted the impoverished nutritional status of both the case and control mothers which may have had a significant impact on other fetal growth parameters.
| Discussion | | |
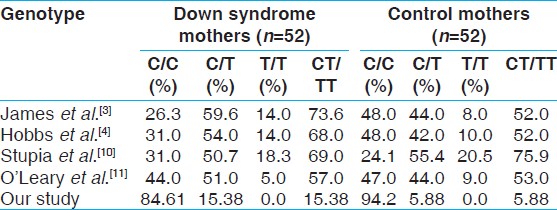
Down syndrome is the first clinically defined genetic disorder shown to be chromosomal in origin. It is characterized by multiple somatic anomalies and cognitive impairment. Although common cellular and molecular mechanism involved in this meiotic nondisjunction remain unknown, folic acid and polymorphism on gene coding for enzymes involved in its metabolism are thought to influence meiotic disjunction. [8],[9] As shown below [Table 1] the frequency of homozygous normal (C/C) in our study was 84.61% in comparison to 26.3% in study by James, et al. [3] The heterozygous mutant (C/T) in our study was 15.38% in comparison to 59.6% in the above study. We did not find any homozygous mutant either in cases or in controls. This is not surprising given the low incidence of T allele in Asians as well as a small sample size. The low T allele frequency was also observed in south India in a study by Cyrus, et al., [12] the minor allele frequencies (T allele) in case mothers and fathers were 4.17% and 6.94% respectively. The cause may be no preferential transmission of T allele and ethnicity genetic prevalence. The frequency of the C/C genotype was significantly higher in the mothers of children with Down syndrome than in control mothers. The overall mutant allele frequency was not significantly higher in mothers of children with Down syndrome than in control mothers.
We found combined mutant allele frequency in Down, 15.38%, and in control mothers 5.88 % in our study. In an Indian study by Sheth, et al. [7] the mutant alleles were 53.84% and 28.5% in cases and controls respectively. In some Indian studies [Table 2] combined mutants were not higher in Down syndrome mothers compared to controls. In our study though combined mutants were higher in Down syndrome mothers than controls in absolute number, the relationship was not statistically significant. We did not get any homozygous TT genotype in our case and control groups. Low frequency of the T allele and its heterozygous distribution among Indians has been well documented by Franco, et al. [14] Singh, et al. did not get a single homozygous in the control group where this polymorphism was evaluated for male infertility. [15] A study done in AIIMS by Kohli, et al. (2004) showed 28.16% mutant allele against 15.38% in our case. They did not find any homozygous TT genotype in case mothers.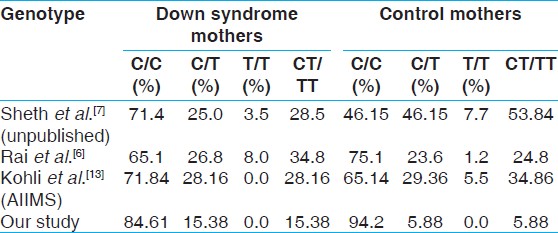 | Table 2: Comparison of maternal methylenetetra hydrofolate reductase genotype with Indian studies
Click here to view |
Analyzing the data of MTHFR polymorphism in relation to the age group of below and above 30 we found no significant association in the age group less than 30 years (P = 0.445) and in more than 30 years (0.220) [Table 3]. Although we did not find association with polymorphism and Down syndrome, there might also be a possible independent effect of maternal MTHFR polymorphism on meiotic nondisjunction by an indirect effect on oocyte DNA. The reduced MTHFR enzyme activity results in increased level of homocysteine, reducing the resynthesis of methionine and producing DNA hypomethylation. [3]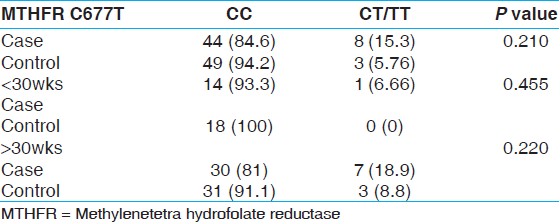 | Table 3: Prevalence of maternal methylenetetra hydrofolate reductase genotype in down syndrome-affected pregnancies and control mothers
Click here to view |
We studied serum levels of folate, RBC folate, vitamin B12, homocysteine, and MTHFR polymorphism in mothers of Down syndrome versus control mothers. [16],[17],[18] We studied RBC folate in addition as it is a preferred marker to assess long-term folate status. Plasma folate is indicative about recent folate status. In our study, even though the isolated analysis of polymorphism did not show an association with maternal risk for Down syndrome, we observed the higher median number of polymorphic alleles in Down syndrome mothers compared to controls. The result of this initial study indicates that folate metabolism is abnormal in mothers of children with Down syndrome and this may be explained, in part, by the genetic susceptibility due to polymorphism in the MTHFR gene. [15]
Published literature had shown that folate and vitamin B12 may not be the only cause of nondisjunction and meiotic error in Down syndrome. It has also been observed that low thiols is indicative of low protein intake can be a cause of hyperhomocysteinemia. Hyperhomocysteinemia, whether caused by a genetic mutation or diet, alters the abundance of several liver proteins involved in homocysteine/methionine metabolism, and antioxidant defense. [16] We also studied the association of serum folate, vitamin B12, and homocysteine levels with C677T polymorphism of MTHFR gene. We found significant association of serum folate with C677T polymorphism (P value 0.005). There were no significant association of RBC folate but was depicting an emerging trend and vitamin B12 and homocysteine with C677T polymorphism (P values 0.118, 0.16, and 0.124 respectively).
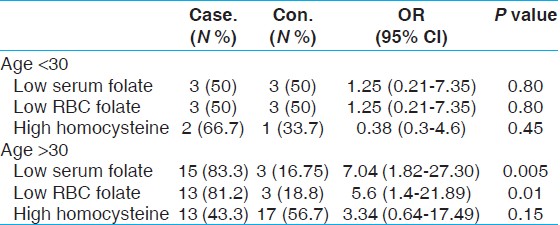
Nevertheless vitamin B12 status is almost normal in the study and control groups. In the combined risk factor study we found significant correlation in combining serum and RBC folate (OR = 3.41, 95% C1-1.21-9.59, P value = 0.02), but we did not find any significant correlation in other combinations as the number was very small, and hence statistical analysis could not be [Table 4], carried out. Nevertheless, we found statistical significant low serum and RBC folate in > 30yr age group mothers [Table 5]. This was a limitation in our study. The serum vitamin B12 level in controls was normal and in cases there were four abnormal values only reflected in our study, so low folate may have had a direct impact on high homocysteine leading to meiotic error, the most common cause of Down syndrome. | Table 4: Serum folate, vitamine B12, homocysteine and methylenetetra hydrofolate reductase polymorphism in mothers of down syndrome vs. the following
Click here to view |
 | Table 5: Relation of risk factors with the age group of mothers with down syndrome babies
Click here to view |
| Conclusion | | |
Our study also revealed higher amount of plasma homocysteine in Down syndrome mothers compared to control mothers though it could not satisfy significant statistical association with MTHFR gene polymorphism. Our study failed to statistically confirm the association of low RBC folate with occurrence of Down syndrome, although it gave a trend as RBC folate is a more reliable marker. However the combined factors of low serum and RBC folate are significantly associated. Larger studies in the Indian subcontinent are therefore required with adequate power to assess the results of our study. The increase of homocysteine can be lowered or prevented by folic acid; thus the metabolic imbalance with genetic mutation can be largely prevented. Our study though initially suggesting the importance of interaction between gene and folate (environment) failed to confirm the association. This has also been suggested by another North Indian cohort study done by Kohli et al.; [13] they however did not analyze vitamin B12 or RBC folate in relationship to the polymorphism.
Currently, we may suggest that a much larger multicentric study needs to look into the geo-ethnic variation in folate and polymorphism and evaluate its association in this era of nutrigenomics.
| Acknowledgment | | |
The study is dedicated to my beloved parents: Barendra Kumar Mohanty (Father), Pramila Mohanty (Mother) and my uncle Harihar Mohanty from whom I draw constant inspiration. I will be indebted to my guide and mentor Dr. Seema Kapoor for her constant help and inspiration. I also thank all the staffs of Genetic Department, MAMC and associated LNH for their constant support in this research work.
| References | | |
| 1. | Epstein CJ. Down syndrome (Trisomy 21). In: Stansbury JB, Fredrickson DS, editors. The metabolism and molecular bases of inherited disease. 7 th ed. New York: Mc Graw-Hill; 1995. p. 749-95. 
|
| 2. | Mikkelsen M. Down syndrome. Cytogenetic epidemiology. Hereditas 1977;6:45-50.
|
| 3. | James SJ, Pogribna M, Pogribny IP, Melynk S, Jean Hine R, Gibson JB, et al. Abnormal folate metabolism and mutation in the MTHFR gene may be maternal risk factors for Down syndrome. Am J Clin Nutr 1999;70:495-550.
|
| 4. | Hobbs CA, Sherman SL, Yi P, Hopkins SE, Torfs CP, Hine RJ, et al. Polymorphism in genes in folate metabolism as maternal risk factor for Down syndrome. Am J Hum Genet 2000;67:623-30.
|
| 5. | Ganji V, Kafai MR. Trends in serum folate, RBC folate, and circulating total homocysteine concentration in United States. J Nutr 2006;136:153-8.
|
| 6. | Rai AK, Singh S, Mehta S, Kumar A, Pandey LM, Raman R. MTHFR C677T and A1298C polymorphisms are risk factors for Down syndrome in Indian mothers. J Hum Genet 2006;51:278-83.
|
| 7. | Sheth JG, Sheth FJ. Gene polymorphism and Folate Metabolism: A Meternal Risk Factor for Down syndrome. Indian Pediatr 2003;40:115-23.
|
| 8. | Ulrey CL, Liu L, Andrews LG, Tollefsbol TO. The impact of metabolism on DNA methylation. Hum Mol Genet 2005;14: R139-47.
|
| 9. | Biselli JM, Goloni-Bertollo EM, Zampieri BL, Haddad R, Eberlin MN, Pavarino-Bertelli EC. Genetic polymorphisms involved in folate metabolism and elevated plasma concentrations of homocysteine: Maternal risk factors for Down syndrome in Brazil. Genet Mol Res 2008;7:33-42.
|
| 10. | Stuppia L, Gatta V, Gaspari AR, Antonucci I, Morizio E, Calabrese G, et al. C677T polymorphism of MTHFR gene as maternal risk of Down syndrome in Italy. Eur J Hum Genetics 2002;10:388-90.
|
| 11. | O'Leary VB, Parlie-McDermott A, Molloy AM, Kirke PN, Johnson Z, Colney M, et al. MTRR and MTHFR polymorphism; Link to Down syndrome. Am J Med Genet 2002;107:151-5.
|
| 12. | Cyrus C, Padmalata R, Chandra N, Gopinath PM, Sathyamoorty K. MTHFR gene variants C677T, A1298C and association with Down syndrome: A case control study from South India. India J Hum Genet 2009;15:60-4.
|
| 13. | Kohli U, Arora S, Kabra M, Kabra M, Ramakrishnan L, Gulati S, et al. Prevalence of MTHFR C677T polymorphism in north Indian mothers having babies with Trisomy 21 Down syndrome. Down Syndr Res Pract 2008;12:133-7.
|
| 14. | Franco RF, Araújo AG, Guerreiro JF, Elion J, Zago MA. Analysis of the 677 C-->T mutation of the methylenetetrahydrofolate reductase gene in different ethnic groups. Thromb Haemost 1998;79:119-21.
|
| 15. | Singh K, Singh SK, Sah R, Singh I, Raman R. Mutation C677T in the methylenetetrahydrofolate reductase gene is associated with male infertility in an Indian population. Int J Androl 2005;28:115-9.
|
| 16. | Chadefaux VB, Conde M, Muller F, Oury JF, Chabli A, Jais J, et al. Methylene tetrahydrofolate reductase polymorphism in the aetiology of Down syndrome. Pediatr Res 2002;51:766-76.
|
| 17. | Lemaire-Adkins R, Radke K, Hunt PA. Lack of check-point control at metaphase/anaphase transition: A mechanism of meiotic nondisjunction in mammalian females. J Cell Biol 1997;139:1611-9.
|
| 18. | Da Silva LR, Vergani N, Galdieri LC, Porto MP, Longhitano SB, Brunono D, et al. Relationship between polymorphism in genes involved in homocysteine metabolism and maternal risk of Down syndrome in Brazil. Am J Med Genet 2005;135A: 263-7.
|
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
| This article has been cited by | | 1 |
Meta-analysis of Methylenetetrahydrofolate reductase maternal gene in Down syndrome: increased susceptibility in women carriers of the MTHFR 677T allele |
|
| D. B. Victorino,M. F. Godoy,E. M. Goloni-Bertollo,E. C. Pavarino | | Molecular Biology Reports. 2014; | | [Pubmed] | [DOI] | |
|
|
|
|