|
 
 |
|
BRIEF REPORT |
|
|
|
| Year : 2014 | Volume
: 20
| Issue : 1 | Page : 92-95 |
| |
Split-hand/feet malformation in three tamilian families and review of the reports from India
S. Deepak Amalnath, Maya Gopalakrishnan, Tarun Kumar Dutta
Department of Medicine, Jawaharlal Institute of Medical Education and Research, Pondicherry, India
| Date of Web Publication | 19-May-2014 |
Correspondence Address:
S. Deepak Amalnath
Department of Medicine, Jawaharlal Institute of Medical Education and Research, Pondicherry 605 006
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.132769

 Abstract Abstract | | |
Split-hand/foot malformation (SHFM) is a rare condition which can be either syndromic or nonsyndromic. We report three unrelated pedigrees, one with autosomal dominant (AD) inheritance and the other two with autosomal recessive (AR) pattern. We also briefly review the published reports from India.
Keywords: Autosomal dominant, autosomal recessive, ectrodactyly, Indian, split-hand/foot malformation
How to cite this article:
Amalnath SD, Gopalakrishnan M, Dutta TK. Split-hand/feet malformation in three tamilian families and review of the reports from India. Indian J Hum Genet 2014;20:92-5 |
How to cite this URL:
Amalnath SD, Gopalakrishnan M, Dutta TK. Split-hand/feet malformation in three tamilian families and review of the reports from India. Indian J Hum Genet [serial online] 2014 [cited 2016 Aug 24];20:92-5. Available from: http://www.ijhg.com/text.asp?2014/20/1/92/132769 |
| Introduction | |  |
Split-hand/foot malformation (SHFM) also known as ectrodactyly or Lobster hand foot malformation, is defined as longitudinal deficiency of a digital ray of the hand or foot except the first or fifth digits [1] (Biesecker, 2009).
SHFM can be a part of a syndrome or can manifest as an isolated malformation. Nearly 50 syndromes have been described with SHFM, the most common being the ectrodactyly-ectodermal dysplasia-cleft syndrome (EEC). Nonsyndromic SHFM can be autosomal dominant (AD), recessive (AR), or X-linked recessive (XLR). [2] We report three unrelated families with nonsyndromic SHFM.
| Case Report | | |
Pedigree 1
A 40-year-old man was admitted for poisoning. His son was incidentally noted to have SHFM. He was born of nonconsanguineous marriage. Similar deformities were present in his mother and brother [Figure 1]. This was present over four generations of the mother's family (seven more members) suggesting AD pattern of inheritance. None of the observed members had any features of ectodermal dyplasia. Despite the deformities, both the brothers were employed, while the mother could knit clothes in her free time. | Figure 1: Mother and two siblings with s plit-hand/foot malformation (SHFM)
Click here to view |
Pedigree 2
A 12-year-old girl who had come to visit a patient was found to have SHFM without any skin or teeth anomalies. Similar deformities were present in her sister [Figure 2], but not in the parents; suggestive of AR pattern.
Pedigree 3
A 19-year-old boy was on follow-up for diabetes. He had developmental delay with deaf mutism. He had SHFM of the left upper limb [Figure 3]. Skin and teeth were normal. He was born of consanguineous marriage and his father said that the boy's elder sibling died after birth and it had similar shaped hands and feet. The parents were normal suggesting AR inheritance.
| Discussion | | |
The basis for SHFM is related to the defects in the patterning of the limb development. The three major tissues responsible for limb patterning are: Apical ectodermal ridge (AER), zone of polarizing activity (ZPA), and progress zone (PZ). The AER determines the proximodistal axis by directing the PZ. The ZPA determines the anteroposterior axis of the limb. [2]
Three mechanisms have been proposed for the limb defects in SHFM. Experimental evidence suggests a defect in the AER or ZPA. Second, involvement of late limb patterning genes like Ho × 13 could produce similar defects. A third explanation involves viewing the defect as a branching rather than a patterning defect. [2]
SHFM can be nonsyndromic or as a part of other syndromes like EEC. Nonsyndromic form can have associated long bone defects like tibial aplasia, known as SHFM with long bone deficiency (SHFLD).
The EEC syndrome is the most common form of syndromic SHFM, with cleft lip/palate and teeth and skin anomalies. Mutations in the p63 locus (SHFM 4) are often associated with EEC and SHFM.
So far six genetic loci have been described for SHFM [2] [Table 1]. These include AD (most common), AR (SHFM 6) and XLR inheritances (SHFM 2) have been described. Of these, only p63 [3] and Wnt10B [4] have been identified conclusively as the disease causing genes. | Table 1: Split - hand/foot malformation types and associated conditions with genes responsible
Click here to view |
Review of reports from India
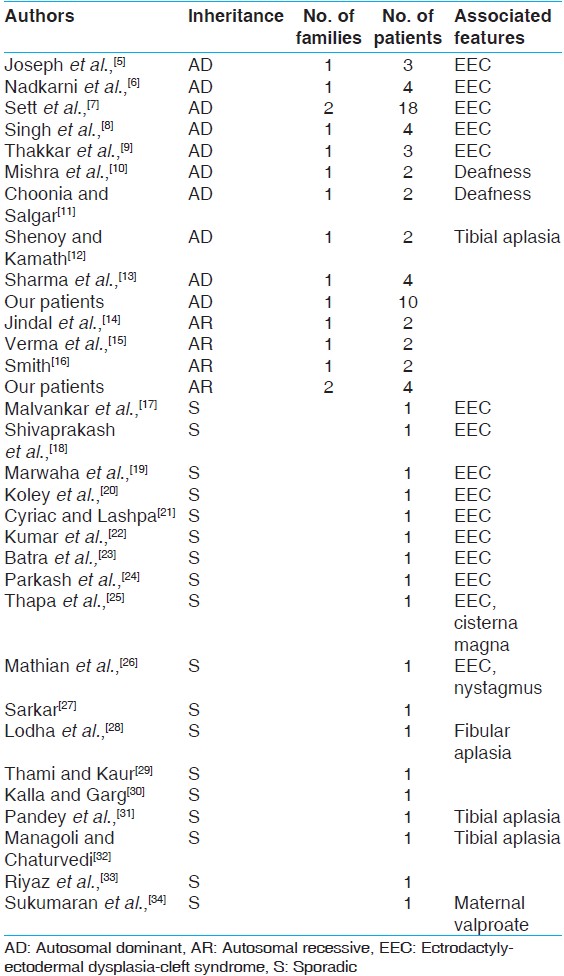
We searched PubMed, Google, and IndMed with the keywords: SHFM, ectrodactyly, India, EEC syndrome. One report was not included due to the nonavailability of any details. A total of 30 prior published reports were included for analysis. Adding our 14 persons to the previously published 66 people, a total of 80 were analyzed [Table 2].
Two-thirds of the 80 individuals were familial (AD 65% and AR 12%), with the rest being sporadic (23%). Maternal valproate use was implicated in one case.
The EEC syndrome was present in 50% of the patients with AD inheritance in 32 and sporadic occurrence in 10 patients. There were no AR cases with EEC syndrome.[34]
Of the 18 sporadic cases, EEC syndrome was present in 10, tibial aplasia in two, and fibular aplasia in one with only five having SHFM. Only one of the nine AD families had isolated SHFM; whereas, all the AR cases had isolated SHFM.
Overall, other associated anomalies included tibial aplasia (four), deafness (two), enlarged cistern magna (one), fibular aplasia (one), and nystagmus (Karsch-Neugebauer syndrome - one).
| Conclusion | | |
This report highlights the varied presentation and inheritance of SHFM in India, with a significant number of reports with a negative family history. These patients may have recessive inheritance or new mutations. Further analysis of these persons could help in understanding this unique condition.
| References | | |
| 1. | Biesecker LG, Aase JM, Clericuzio C, Gurrieri F, Temple IK, Toriello H. Elements of morphology: Standard terminology for the hands and feet. Am J Med Genet Part A 2009;149A: 93-127. 
|
| 2. | Duijf PH, van Bokhoven H, Brunner HG. Pathogenesis of split-hand/split-foot malformation. Hum Mol Genet 2003;12:R51-60.
|
| 3. | Celli J, Duijf P, Hamel BC, Bamshad M, Kramer B, Smits AP, et al. Heterozygous germline mutations in the p53 homolog p63 are the cause of EEC syndrome. Cell 1999;99:143-53.
|
| 4. | Khan S, Basit S, Zimri FK, Ali N, Ali G, Ansar M, et al. A novel homozygous missense mutation in WNT10B in familial split-hand/foot malformation. Clin Genet 2012;82:48-55.
|
| 5. | Joseph R, Nath SG. Association of generalized aggressive periodontitis and ectrodactyly-ectodermal dysplasia-cleft syndrome. Indian J Hum Genet 2012;18:259-62.
[PUBMED]  |
| 6. | Nadkarni J, Ganesh H, Dwivedi R. Familial clustering of a rare syndrome. Indian J Hum Genet 2011;17:26-8.
[PUBMED] |
| 7. | Sett TK, Sengupta S. Familial ectrodactyly-split hand foot malformation. J Anat Soc India 2008;57:151-4.
|
| 8. | Singh D, Daniel R, Verma M, Akhter Z, Beri RS. Split hand/split foot syndrome with atresia of nasolacrimal ducts and buphthalmos. Indian Pediatr 1989;26:1053-5.
|
| 9. | Thakkar S, Marfatia Y. EEC syndrome sans clefting: Variable clinical presentations in a family. Indian J Dermatol Venereol Leprol 2007;73:46-8.
[PUBMED] |
| 10. | Mishra P, Muranjan M, Bharucha BA. Autosomal dominant ectrodactyly with sensorineural deafness. Clin Dysmorphol 2000;9:119-21.
|
| 11. | Choonia AS, Salgar NM. Syndromic form of autosomal dominant split foot malformation. Bombay Hosp J 2011;53.
|
| 12. | Shenoy R, Kamath N. Bilateral congenital split hand with tibial aplasia. Indian J Pediatr 2004;71:948.
|
| 13. | Sharma S, Chhetri A, Singh A. Congenital cleft foot and hand. Indian Pediatr 1999;36:935-8.
|
| 14. | Jindal G, Parmar VR, Gupta VK. Ectrodactyly/split hand feet malformation. Indian J Hum Genet 20009;15:140-2.
|
| 15. | Verma IC, Joseph R, Bhargava S, Mehta S. Split-hand and split-foot deformity inherited as an autosomal recessive trait. Clin Genet 1976;9:8-14.
|
| 16. | Smith R. Available from: http://fovuk.tripod.com/home.html [Last accessed o n 2013 Apr 05].
|
| 17. | Malvankar DD, Sacchidanand S, Mallikarjun M. Ectrodactyly, ectodermal dysplasia, and cleft lip-palate (EEC) syndrome without clefting: A rare case report. Dermatol Online J 2012;18:5.
|
| 18. | Shivaprakash PK, Joshi HV, Noorani H, Reddy V. Ectrodactyly, ectodermal dysplasia, and cleft lip/palate syndrome: A case report of "Incomplete syndrome". Contemp Clin Dent 2012;3:S115-7.
|
| 19. | Marwaha M, Nanda KD. Ectrodactyly, ectodermal dysplasia, cleft lip, and palate (EEC syndrome). Contemp Clin Dent 2012;3:205-8.
[PUBMED] |
| 20. | Koley S, Choudhary SV, Salodkar A, Saoji V. Ectrodactyly, ectodermal dysplasia with cleft lip and palate: A case report. J Pak Assoc Derma 2009;19:240-2.
|
| 21. | Cyriac MJ, Lashpa E. Lobster-claw hand: A manifestation of EEC syndrome. Indian J Dermatol Venereol Leprol 2006;72:54-6.
[PUBMED] |
| 22. | Kumar HN, Kugar TS, Rao RJ, Kodkany S. EEC syndrome. Indian J Ophthalmol 2007;55:162-3.
[PUBMED] |
| 23. | Batra P, Duggal R, Parkash H. EEC syndrome: A case report. J Indian Soc Pedod Prev Dent 2003;21:75-8.
[PUBMED] |
| 24. | Parkash H, Grewal MS, Sidhu SS. Ectrodactyly, ectodermal dysplasia, cleft lip and palate (EEC): A rare syndrome. Indian J Pediatr 1983;50:337-40.
|
| 25. | Thapa R, Mallick D, Biswas B, Ghosh A. Mega cisterna magna in ectrodactyly, ectodermal dysplasia and cleft lip/palate syndrome. Indian J Pediatr 2010;77:706.
|
| 26. | Mathian VM, Sundaram AM, Karunakaran R, Vijayaragavan R, Vinod S, Rubini R. An unusual occurrence of Karsch-Neugebauer syndrome with orodental anomalies. J Pharm Bioallied Sci 2012;4:S171-3.
|
| 27. | Sarkar S. Orodental abnormalities in lobster claw syndrome (a type of syndactyly). J Indian Soc Pedod Prev Dent 1999;17:107-10.
[PUBMED] |
| 28. | Lodha A, Mody P, Malik A, Singh S. Ectrodactyly fibular aplasia. Indian Pediatr 1993;30:1123-5.
|
| 29. | Thami GP, Kaur S. Split hand-foot malformation: A congenital central limb ray deficiency. J Postgrad Med 2002;48:209-10.
[PUBMED] |
| 30. | Kalla G, Garg A. Ectrodactyly. Indian J Dermatol Venereol Leprol 2002;68:152-3.
[PUBMED] |
| 31. | Pandey D, Pai MV, Nambiar J, Lewis L, Pandey V. Gollop-Wolfgang Complex-A rare limb deficiency syndrome: Case report and review of literature. Internet J Gynecol Obstet 2008;9:1.
|
| 32. | Managoli SS, Chaturvedi P. Tibial hemimelia-split hand/foot syndrome with rare anomalies. Indian Pediatr 2005;42:190-1.
|
| 33. | Riyaz N, Riyaz A, Chandran R, Rakesh SV. Focal dermal hypoplasia (Goltz syndrome). Indian J Dermatol Venereol Leprol 2005;71:279-81.
[PUBMED] |
| 34. | Sukumaran S, Krishnamoorthy T, Thomas SV. Split-hand/split-foot malformation associated with maternal valproate consumption. Neurol India 2005;53:251-2.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2]
|