| |


 |
| Year : 2012 | Volume
: 6
| Issue : 2 | Page : 67-70 |
|
|
|
|
|
CASE REPORT Triple disruption of the superior shoulder suspensory complex
Sae Hoon Kim, Seok Won Chung, Se Ho Kim, Seung Han Shin, Young Ho Lee
Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul National University Hospital, Republic of Korea
Correspondence Address:
Young Ho Lee
Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul National University Hospital
Republic of Korea
 Source of Support: None, Conflict of Interest: None  | 5 |
DOI: 10.4103/0973-6042.96999

|
|
|
|
| Date of Web Publication | 7-Jun-2012 |
 Abstract Abstract | | |
The superior shoulder suspensory complex (SSSC) is an extremely important structure composed of a ring of bone and soft tissues at the superior aspect of the shoulder. Double disruption leads to instability of the construct and usually requires operative treatment. Triple disruption of the SSSC is extremely rare and is encountered in high-energy trauma cases often in association with other injuries. The authors experienced a case of triple disruption involving the acromion, coracoid process, and acromioclavicular separation. This type of SSSC disruption is unlikely to have been caused by a single impact and is rather caused by multiple impacts during one traumatic event.
Keywords: Superior shoulder suspensory complex, SSSC, triple disruption
How to cite this article:
Kim SH, Chung SW, Kim SH, Shin SH, Lee YH. Triple disruption of the superior shoulder suspensory complex. Int J Shoulder Surg 2012;6:67-70 |
| Introduction | |  |
The Superior Shoulder Suspensory Complex (SSSC) is an extremely important structure in terms of shoulder biomechanics, and is composed of a ring of bony and soft tissues at the superior aspect of the shoulder. [1],[2] It comprises the glenoid process, the coracoid process, the coracoclavicular ligament, the distal end of the clavicle, the acromioclavicular joint, the coracoacromial ligament, and the acromial process. [1],[2] Single traumatic disruptions of the SSSC, such as type I distal clavicle fractures, are common, but double disruptions are known to be rare. [1],[2],[3] Double disruption can occur in combination with bone and soft tissue injuries, [2] and leads to construct instability. Therefore, they usually require operative treatment. [1],[3],[4] On the other hand, it is difficult to conceive of triple SSSC disruption during a single traumatic event. In fact, only two non-English case reports were found in a comprehensive literature search.
Here, we present the case of a patient with combined fractures of the coracoid and acromion with acromioclavicular separation after a severe in-car traffic accident.
| Case Report | | |
A 27-year-old man with no previous shoulder problems experienced direct trauma during an in-car traffic accident. Although no definite neurovascular abnormalities of the right upper extremity were found, he had lower extremity paraplegia below the T8 level. In addition, he had dyspnea because of bilateral hemothorax and pleural effusion caused by direct traumatic lung injury.
Initial radiographs of the right shoulder showed comminuted fractures in the right scapular superior border, acromion, and coracoid process, and a humerus shaft fracture with acromioclavicular joint separation [Figure 1]. Fracture of the acromion and acromioclavicular joint separation had substantial displacement and fracture of the coracoid is regarded as type I according to Ogawa's classification. [5] These fractures were also confirmed by computed tomography (CT) scan with 3D reconstruction [Figure 2]. 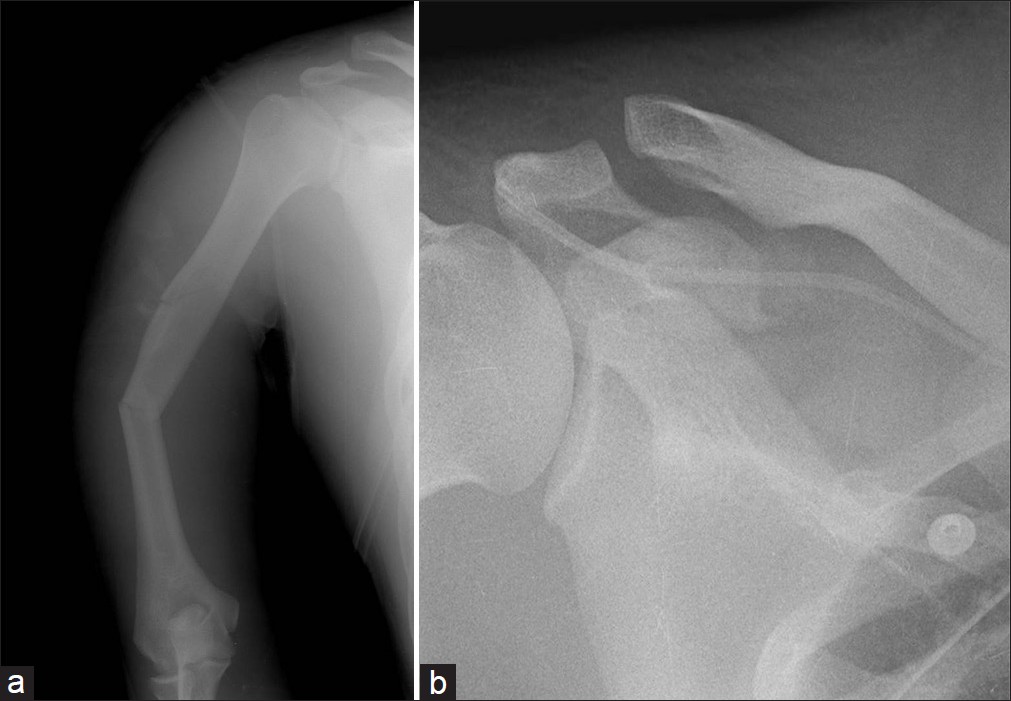 | Figure 1: Radiographs demonstrating comminuted fractures in the right scapular superior border, acromion, and coracoid process, and a humerus shaft fracture with acromioclavicular ligament separation
Click here to view |
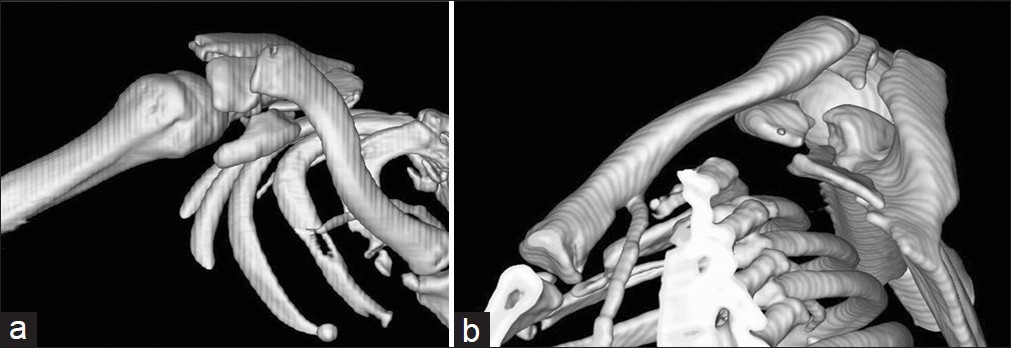 | Figure 2: Preoperative 3D CT images: Anterior view (a) and medial view (b)
Click here to view |
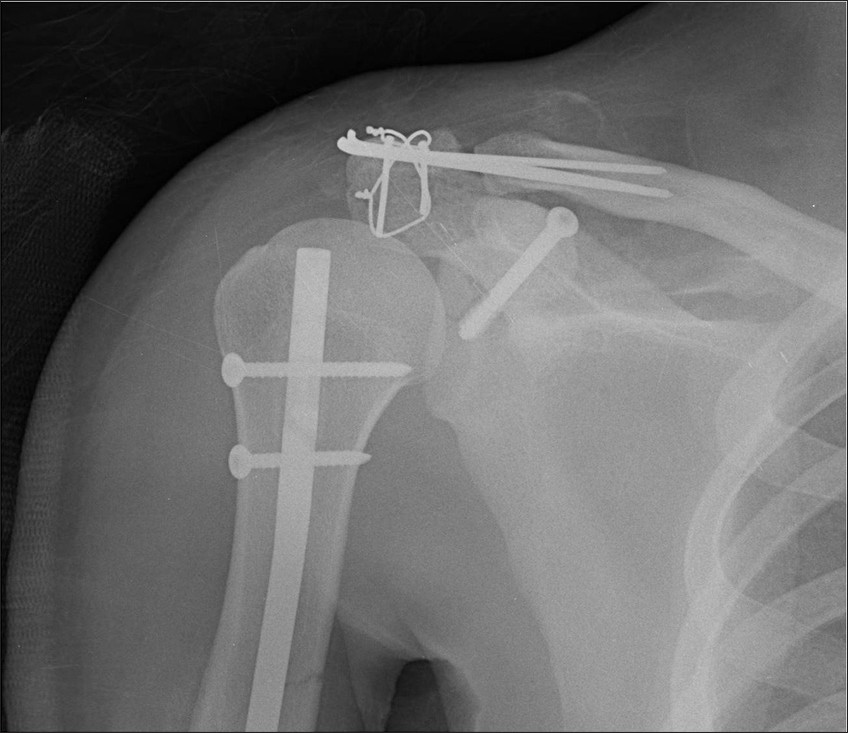
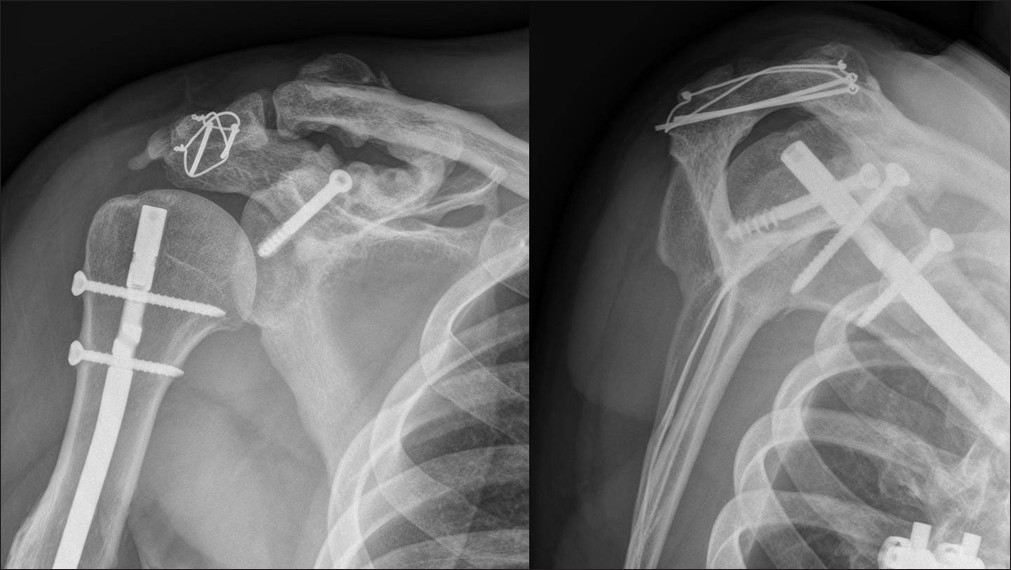
On the 7 th day post-injury, surgery for the shoulder was undertaken on the triple disruption injury of the SSSC and fracture of the humeral shaft. Under general anesthesia, with the patient in beach chair position, a saber cut approach was adopted from the posterior border of the acromion to the coracoid. Prior to the fixation of SSSC injuries, intramedullary nailing (Synthesis, Paoli, PA, USA) of the humeral fracture was performed. The entry point of the nail was established through the detachment of the anterior deltoid and fracture site of the acromion. After humeral shaft fixation, the coracoid fracture was reduced and fixed with one cancellous screw [Figure 3] (6.5 mm × 50 mm, 16 mm half thread; Synthes Australia, North Ryde, Australia). The acromial fracture was then reduced and fixed with tension band wiring [Figure 4] (Tension Band Pin System, Acumed, Hillsboro, OR, USA), and finally, the acromioclavicular joint was fixed with three transarticular Steinmann pins [Figure 5]. After meticulous reattachment of the deltoid, the wound was closed in layers [Figure 6].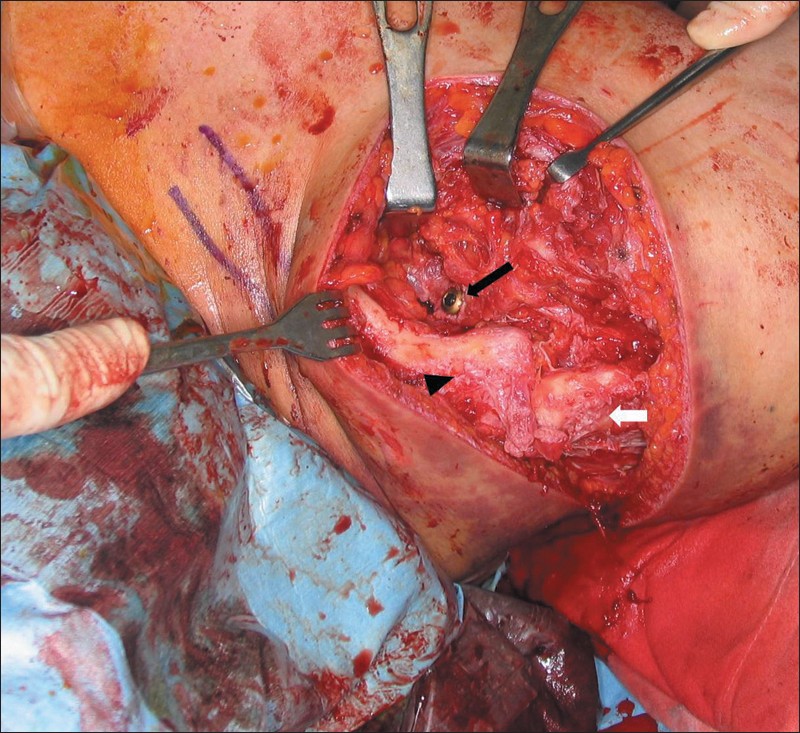 | Figure 3: Radiograph showing fixation of the coracoid process with a cancellous screw (black arrow), the clavicle (arrowhead), and the acromion (white arrow)
Click here to view |
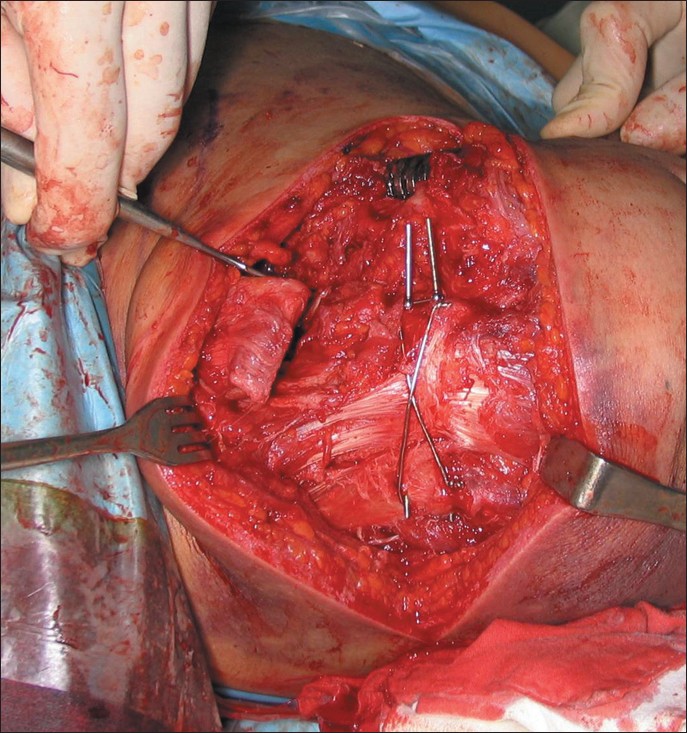 | Figure 4: The acromial fracture was fixed using the tension band wiring technique
Click here to view |
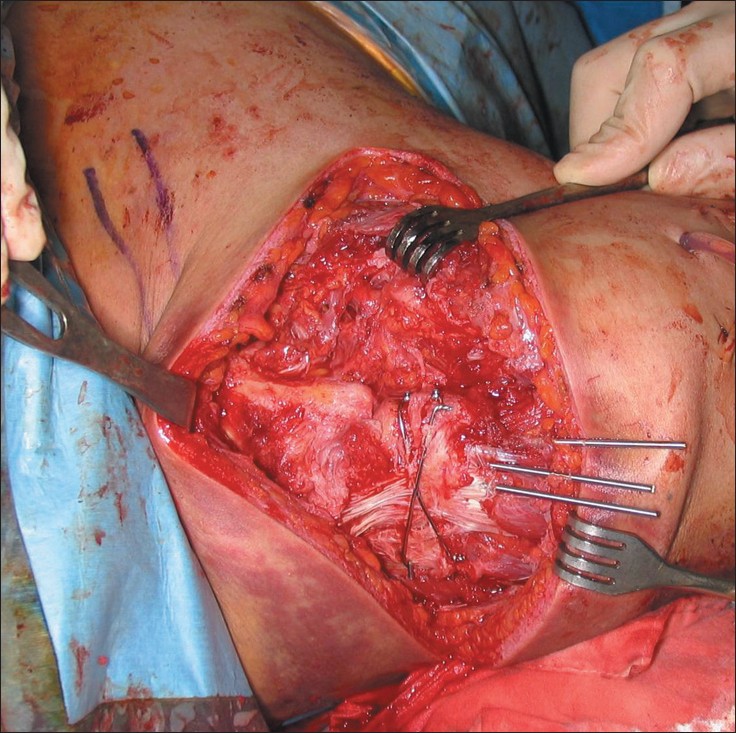 | Figure 5: The acromioclavicular joint was fixed using three transarticular S-pins
Click here to view |
Postoperatively, the patient was immobilized with an abduction brace for 6 weeks. During this period, shoulder joint motion, including pendulum exercise, was not allowed. However, shrugging of the affected shoulder, and active hand and wrist motion were encouraged immediately after surgery. At 6 weeks post-injury, a self-assisted range of stretching exercises was encouraged. Active range of motion exercise was allowed from 9 weeks. At 12 weeks, transarticular S-pins were removed under fluoroscopic guidance and local anesthesia at an outpatient clinic. No other implant was removed. At 6 months, the patient had painless full range of motion. He was followed for 5 years, and had a good functional outcome at the last follow-up [Figure 7] and [Figure 8].
| Discussion | | |
Fractures of the scapula are relatively rare injuries and account for 3-5% of all fractures involving the shoulder girdle and 1% of all fractures. [6] Direct trauma to the lateral or posterosuperior aspect of the forequarter is the most common mechanism of injury. [7] Fractures of the coracoid process account for 2-5% of all scapular fractures, [8] and the mechanisms involved determine fracture sites. According to Ogawa et al., [9] coracoid fractures can be classified into two types by location. Type I fractures, which are proximal to the coracoclavicular ligament, are usually associated with other injuries, such as acromioclavicular separation (the most frequent) scapular fractures, deltoid lacerations, clavicle fractures, and acromion fractures. Type I fractures are more common but unstable, and thus require open reduction and internal fixation. [9] However, avulsion fractures and type II fractures which are distal to the coracoclavicular ligament could be caused by contractions of the coracobrachialis, the short head of the biceps, and the pectoralis minor. [10] It would appear that type I coracoid fracture commonly occurs with concomitant acromioclavicular separation by a similar mechanism as acromioclavicular-coracoclavicular separation. In this case, the coracoclavicular ligament is usually saved. Besides, acromion fracture also occurs in 8% of scapular fractures. [11]
Previous studies mentioned that double disruption of the SSSC is a rare injury around the shoulder. [1],[3],[12] However, if one considers the structures involved in common injuries at the SSSC, for example, the acromioclavicular and coracoclavicular ligaments for acromioclavicular-coracoclavicular separation, and the clavicle and coracoclavicular ligament for type II distal clavicle fractures, double disruption of the SSSC should not be regarded as a rare injury. [1],[2] In ring structure concept, like the pelvis, it is more reasonable to think if the ring is broken in one area and the fragments displaced, then there must be a fracture or dislocation in another portion of the ring. [13]
However, triple disruption of the SSSC, which is breakage of the ring in three different locations, is a very rare injury indeed. A comprehensive literature search showed this type of injury has only been reported twice in the non-English literature, [14],[15] and both of these cases had a displaced fracture of the coracoid process associated with fracture of the acromion and a minimally displaced fracture of the distal clavicle. [14],[15] On the other hand, our patient had a displaced fracture of the coracoid process associated with fracture of the acromion, and the separation of the acromioclavicular joint.
In the two reported cases, the etiologies were a traffic accident in one like our case [15] and a fall from height in the other. [14] We consider that these triple disruptions could not have been caused by a single impact to the shoulder and that rather they were caused by multiple impacts during one severe traumatic event. Our case had a fracture of humeral shaft on the ipsilateral humerus and vertebral fractures. Although associated injuries were not mentioned in one report, [14] the other did mention multiple associated rib fractures.
In structures with the ring concept, complete disruptions at more than two other locations cause instability, thus surgical intervention is usually indicated. [1],[3] In our case, triple disruption of the structure was a definite indication for surgery.
In conclusion, triple disruption of the SSSC is an extremely rare injury caused by high-energy trauma and it is often associated with other injuries. We report satisfactory outcome in this injury.
| References | | |
| 1. | Goss TP. Double disruptions of the superior shoulder suspensory complex. J Orthop Trauma 1993;7:99-106. 
[PUBMED] |
| 2. | Goss TP, Owens BD. Fractures of the Scapula. Vol. 1, In: Rockwood CA Jr, Matsen FA, Editors, 4th ed. The Shoulder. Philadelphia, PA: Saunders/Elsevier, 2009. pp. 333-80.
|
| 3. | Oh W, Jeon IH, Kyung S, Park C, Kim T, Ihn C. The treatment of double disruption of the superior shoulder suspensory complex. Int Orthop. 2002;26:145-9.
|
| 4. | Goss TP. Scapular fractures and dislocations: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:22-33.
[PUBMED] [FULLTEXT] |
| 5. | Ogawa K, Yoshida A, Takahashi M, Ui M. Fractures of the coracoid process. J Bone Joint Surg Br 1997;79:17-9.
[PUBMED] [FULLTEXT] |
| 6. | Thompson DA, Flynn TC, Miller PW, Fischer RP. The significance of scapular fractures. J Trauma 1985;25:974-7.
[PUBMED] |
| 7. | Lapner PC, Uhthoff HK, Papp S. Scapula fractures. Orthop Clin North Am 2008;39:459-74, vi.
[PUBMED] |
| 8. | Ada JR, Miller ME. Scapular fractures. Analysis of 113 cases. Clin Orthop Relat Res 1991;269:174-80.
[PUBMED] |
| 9. | Ogawa K, Yoshida A, Takahashi M, Ui M. Fractures of the coracoid process. J Bone Joint Surg Br 1997;79B:17-9.
|
| 10. | Rounds RC. Isolated fracture of the coracoid, process. J Bone Joint Surg Am 1949;31A:662.
[PUBMED] |
| 11. | McGahan JP, Rab GT, Dublin A. Fractures of the scapula. J Trauma 1980;20:880-3.
[PUBMED] |
| 12. | Lim KE, Wang CR, Chin KC, Chen CJ, Tsai CC, Bullard MJ. Concomitant fracture of the coracoid and acromion after direct shoulder trauma. J Orthop Trauma 1996;10:437-9.
[PUBMED] [FULLTEXT] |
| 13. | Tile M. Pelvic ring fractures: Should they be fixed? J Bone Joint Surg Br 1988;70B:1-12.
|
| 14. | Jung CY, Eun IS, Kim JW, Ko YC, Kim YJ, Kim CK. Treatment of triple fracture of the superior shoulder suspensory complex. J Korean Orthop Assoc 2011;46:68-72.
|
| 15. | Lecoq C, Marck G, Curvale G, Groulier P. Triple fracture of the superior shoulder suspensory complex. Acta Orthop Belg 2001;67:68-72.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8]
| This article has been cited by | | 1 |
Triple rotura del complejo suspensorio del hombro |
|
| I. Tamimi Mariño,I. Martin Rodríguez,J. Mora Villadeamigo | | Revista Española de Cirugía Ortopédica y Traumatología. 2013; 57(5): 371 | | [Pubmed] | [DOI] | | | 2 |
Triple injury to the superior shoulder suspensory complex |
|
| Andy Li-Jen Liu,Perng-Jong Chen,Po-Wen Shen | | Formosan Journal of Musculoskeletal Disorders. 2013; 4(3): 81 | | [Pubmed] | [DOI] | | | 3 |
Triple fracture of the shoulder suspensory complex |
|
| I. Tamimi Mariño,I. Martin Rodríguez,J. Mora Villadeamigo | | Revista Española de Cirugía Ortopédica y Traumatología (English Edition). 2013; 57(5): 371 | | [Pubmed] | [DOI] | |
|
|
|
|