| |


 |
| Year : 2012 | Volume
: 6
| Issue : 3 | Page : 76-81 |
|
|
|
|
|
ORIGINAL ARTICLE The outcome of surgical fixation of mid shaft clavicle fractures; looking at patient satisfaction and comparing surgical approaches
Zeiad A Alshameeri, Krishnaiah Katam, Mohammed Alsamaq, Paresh Sonsale
Department of Trauma and Orthopaedics Surgery, Good Hope Hospital, Heart of England NHS foundation Trust, Rectory Road, Sutton Coldfield, Birmingham, B75 7RR, United Kingdom
Correspondence Address:
Zeiad A Alshameeri
C/o Mr. Sonsale secretary office, Good Hope Hospital Rectory Road, Sutton Coldfield, Birmingham, B75 7RR
United Kingdom
 Source of Support: None, Conflict of Interest: None  | 3 |
DOI: 10.4103/0973-6042.102556

|
|
|
|
| Date of Web Publication | 17-Oct-2012 |
 Abstract Abstract | | |
Introduction: Clavicle fractures represent 2.5% of fractures in adults and almost 44% of shoulder injuries. The treatment is usually non-surgical with good results; however, significantly displaced fractures can be associated with high non-union rate and therefore many would advocate surgical fixation. This is traditionally carried out by direct approach over the clavicle but an infraclavicular approach has also been used for clavicular fixation. The aim of this study was to identify the main indications for surgical intervention at our unit and patient satisfaction following surgery. We also wanted to compare the direct and the infraclavicular surgical approaches in relation to the outcome of surgical intervention.
Materials and Methods : Retrospective study looking at all the clavicle fractures managed surgically over 5 years at our department. Information relating to surgical indication, surgical approach, complications, outcome, patient satisfaction, and oxford shoulder score were collected.
Results : A total of 35 patients were identified, the majority were males (n = 25) and most (n = 29) were working at the time of injury. The commonest indication for surgery was displacement with shortening (n = 16). The infraclavicular approach was used in the majority of patients (n = 21), the rest (n = 14) had direct incision. Evidence of radiological and union was achieved in all patients after an average of 13 (8-24) weeks. There were no major complications but minor complications were reported in 28% and 19% of cases with direct and infraclavicular approaches, respectively. Plates were removed from six symptomatic patients; infraclavicular (n = 2) and direct approach (n = 4). Four asymptomatic plates were removed on patients' requests. All patients returned to work (after an average 2.6 months), had good oxford shoulder score between 12-20, regardless of the surgical approach used. All patients except one would recommend it to a friend.
Conclusion : Our study showed excellent surgical outcome for displaced clavicle fractures supported by the high union rate, good oxford shoulder score, high return to work rate, and good patient's satisfaction. The number of minor complications and symptomatic metal work removal was less in the infraclavicular approach.
Keywords: Mid shaft clavicle fracture, outcome, patient satisfaction, surgical approaches
How to cite this article:
Alshameeri ZA, Katam K, Alsamaq M, Sonsale P. The outcome of surgical fixation of mid shaft clavicle fractures; looking at patient satisfaction and comparing surgical approaches. Int J Shoulder Surg 2012;6:76-81 |
How to cite this URL:
Alshameeri ZA, Katam K, Alsamaq M, Sonsale P. The outcome of surgical fixation of mid shaft clavicle fractures; looking at patient satisfaction and comparing surgical approaches. Int J Shoulder Surg [serial online] 2012 [cited 2016 Jun 7];6:76-81. Available from: http://www.internationalshoulderjournal.org/text.asp?2012/6/3/76/102556 |
| Introduction | |  |
Clavicle fractures are caused by falls and high-velocity injuries commonly associated with sport. They represent 5% of fractures in adults and almost 44% of shoulder injuries. [1],[2] The clavicle is commonly fractured in the thin middle portion where it is most devoid of muscle attachments. [2],[3],[4] According to Socrates, clavicle fractures need little more than benign neglect and therefore nonoperative treatment using figure of eight brace or a sling [5],[6] have been the mainstream of treatment for clavicle fractures. This was also reinforced by Neers and Browns [7],[8] studies which showed high nonunion and complication rates in surgically treated patients. Subsequently, more studies refuted this generalized attitude [6],[9] and showed that nonunion rate, especially in displaced middle clavicle fractures, can be as high as 24%. [4],[10] A relatively recent randomized control trial has shown that surgical treatment of these fractures can reduce nonunion rate from 15% to 2.2%. [11] However, there is still a lack of consensus on when surgical treatment is indicated for many types of mid clavicle fractures.
In surgical plate fixation, traditionally a direct incision is made over the clavicle. An infraclavicular approach has been proposed by some authors. [12] This approach leaves the scar lying below the clavicle and therefore we thought that this potentially could lead to less scar and metal irritations.
At our small unit, clavicle fractures are mainly managed nonoperatively; however, few cases had to have surgical interventions and both surgical approaches have been used over the last few years. Therefore, in this single unit retrospective study, we aimed to identify why surgical fixation was carried out in some patients and to compare the outcome of the direct and infraclavicular approaches in relation to the complications and overall outcome of surgery using patient feedback and oxford shoulder score.
| Materials and Methods | | |
We searched the database over a period of 5 years to identify the patients who had clavicle fractures treated surgically. After obtaining a list of patients, their radiographs were reviewed and only mid shaft clavicle fractures were selected. Subsequently, patients' notes were pulled out to review the operation notes and all the clinical follow-up letters.
Information relating to patients demographics, mechanism of the injury, indication for surgery, type of surgical intervention, type of theatre used, operating surgeon, and complications of surgery were gathered.
Subsequently, two questionnaires were sent to the patients. One questionnaire asked patients regarding employment status and their satisfaction following surgery. The second questionnaire was the oxford shoulder score to assess the functional outcome following the treatment.
Method of fixation
All the patients had plate fixation. The procedure is normally carried out on a beach chair position under general anesthesia with the head of the patients turning away from the site of surgery to facilitate access. Two types of surgical approaches were employed, infraclavicular and direct approach. The infraclavicular approach as described by Coupe et al.[12] is achieved by proximally retracting the skin in the supraclavicular fossa, allowing an incision to be marked onto the clavicle centered over the fracture. When the skin retraction is released, the incision mark comes to lie below the inferior border of the clavicle. Skin incision is then made along the mark up to the pectoralis fascia. This thick flap is elevated up to superior surface of the clavicle. This preserves the pectoralis attachment. The rest of the fixation is carried out in the traditional way. At our department, plates were used to achieve rigid fixation. The plates types used are described in the results section. Two-layer closure techniques were used in all patients (Pectoralis fascia is closed over the plate and skin with subcuticula 3/0 suture). Postoperatively, AP and 15° cephalad radiographs are taken and at 6 weeks later and at subsequent times until union of fracture.
| Results | | |
Over a period of five years, 35 patients were identified to have undergone surgical treatment for their mid shaft clavicle fractures. Some of these patients were seen in the follow up clinic where they were clinically assessed and the shoulder score and patients' satisfaction forms were filled in. For the majority of patients, the questionnaire was sent via post. We had 100% response rate mainly because all patients lived locally.
The majority of patients were males (n = 25, 71.4%), and half of all the patients (n = 18) did intensive manual work. The fracture was commonly on the non-dominant side (n = 22, 62.9%) because the left side was the commonest fractured clavicle (n = 23, 65.7%) [Table 1].
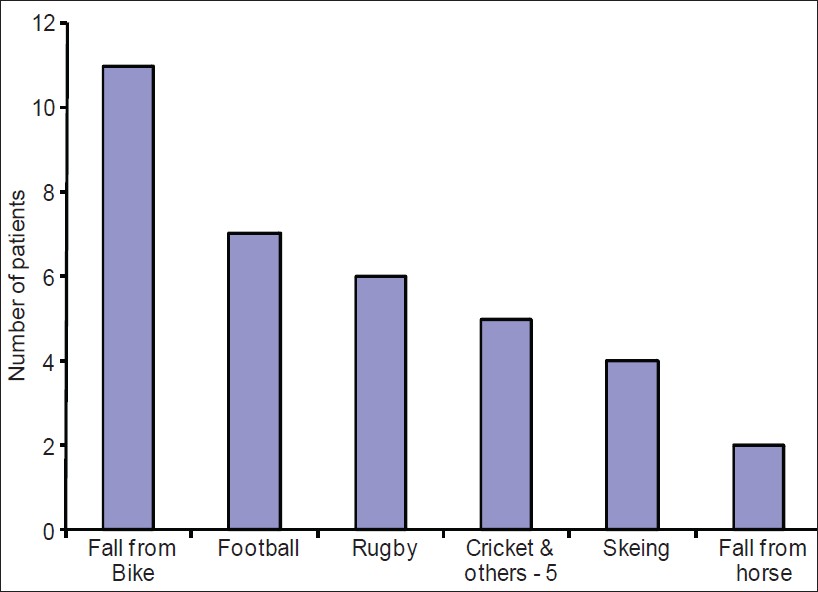
Almost all the injuries were associated with sport [Figure 1] and the majority involved high-velocity injury, n = 32.
The main indications for surgery are depicted in [Table 1]. Many of the patients had more than one indication for surgery; however, displacement, shortening, and communition were the most frequent reasons for surgical intervention. The majority of the patients (n = 28) had acute surgical intervention (less than one week) and only seven had delayed surgically procedures after nonoperative treatment failed and these had elective admissions for surgery. Twenty-four (68.6%) were operated on by a consultant, and the rest (except one performed by a registrar) were operated on by associated specialist.
The infraclavicular approach was used in 21 cases (60%) and the rest had direct approach. Soft tissue interposition and displacement were the commonest interoperative finding [Table 2].
Plating was the only mode of fixation, the type of plates used are depicted in [Table 2]. In addition to plating, interfragmentary screws or suture tying of fragments was used in few cases. Bony grafting was used in 12 cases in the form of Iliac crest (n = 7) or bony putty (n = 5). Bone grafting was used in all delayed or nonunion fractures (n = 7) and in severely comminuted fractures resulting in bone loss (n = 5).
No major complications were recorded. The minor complications are listed in [Table 3]. Some patients had more than one complication.
There was a 100% clinical and evidence of radiological union rate after an average duration of 13 weeks. One, 10-year-old patient, re-fractured the clavicle with the plate in situ after 8 weeks but complete union achieved 24 weeks later following the initial surgery.
Almost all patients (n = 29) returned back to work after an average sick leave duration of 2.5 months (2 weeks to 6 months). Three patients were school going and, two patients were unemployed and one patient who was employed at the time of surgery did not state whether he had gone back to work.
The average shoulder score was 15.14 indicating a satisfactory joint function [Table 3] and almost all patients (n = 34) were satisfied with their outcome and would recommend it to a friend. The only patient who was not satisfied had a painful shoulder but no pain at the fracture site.
In total, 10 (28.6%) plates were removed after an average of 35 weeks [Table 3]. Six patients suffered minor complaints (4 with direct and 2 with infraclavicular approach) warranting the removal of the plates, whilst the rest (n = 4) had no clinical indications for plates removal, but were removed on patients' requests. Nine of the plates removed were from those treated acutely. Furthermore, half of the female patients had their plates removed, but overall there was no single factor associated with high metal work removal [Table 4]. | Table 4: Factors and metal removal (including asymptomatic plate removal)
Click here to view |
| Discussion | | |
Falls and sport-related injuries in mainly young male patients are the commonest cause for clavicle fractures [1],[2],[13] and this is what has also been shown in this study. Most of simple mid clavicle fractures can be treated nonoperatively and heal with little or no complications. [4],[13],[14] Surgery is absolutely indicated in cases such as painful nonunion, open fractures, floating shoulders, and fractures associated with neurovascular injuries. [14] In other situations, there is no consensus regarding method of treatment; [13] however, fractures that are more likely to go into nonunion have been shown to be associated with total displacement, sever communition, advanced age, and female gender. [10],[13],[15] Furthermore, malunion of the clavicle in association with shortening (of at least 15 mm [16],[17] )
is thought to result in winging of the scapula, change in glenoid orientation, and upward angulations of the clavicle at the sternoclavicular joint. [17],[18] The combination of these changes results in a decrease in the moment arm of individual shoulder girdle muscles. This is thought to be the reason for the residual deficit in the shoulder girdle muscles' strength and their fatigability as demonstrated by functional and computer modeling studies. [16],[17],[18],[19] Therefore, restoration of the clavicular length is believed to be a pretext for surgical fixation of clavicle fractures, especially in the active young group of patients. [16],[17]
Nonoperative management of mid shaft clavicle fractures remains the mainstream at our department which explains the small number of patients over a period of five years. Hence, only a small number of patients (n = 7) went to painful none or delayed union and were subsequently surgically fixed. Those patients who had acute surgical interventions had justifiable indications consistent with high risk of nonunion. The justification for surgery was also supported by the interoperative findings such as soft tissue interposition and multi-fragment fractures.
The surgical approach for fixation of the clavicle is dependent of the devise used. Two of the main surgical approaches have been described for plate fixation; the infraclavicular and the direct approach. [12],[20]
To our knowledge, no direct comparison has been made between the infraclavicular and the direct approaches for the treatment of clavicle fractures. A randomized controlled study using the direct approach [20] reported few major and minor complications. From a total of 62 patients, there were two non-unions, eleven hardware-related complications (5 requiring removal), three cases of wound infection (requiring plate removal), and one had mechanical failure. Another study looking at the outcome of infraclavicular approach [12] reported two major complications; one plate broke and the other was deep infection; 6 minor complications including dysesthesia over the scar and in total 17 symptomatic plate removals.
From our small study, we could not find major differences in the outcome of both approaches, but the infraclavicular approach is slightly favored when looking at the number of minor complications encountered and the rate of symptomatic plate removal. However, our numbers are very small to get any statistical significant differences. Our overall outcome of surgery (using both approaches) is however better in comparison with few studies [4],[7],[8],[11],[14] and this could be due to the continuing improvement in the operative techniques but importantly in our study, the majority of operations were carried out by senior surgeons. The majority of the patients went back to their manual work (after varying duration of sick leaves) and all had satisfactory shoulder score. This yields further support for the surgical management of these fractures. Furthermore, the good Oxford Shoulder Score obtained in this study is consistent with the good Constant shoulder scores and DASH scores that have been reported in surgically treated patients. [11] Vender et al. also found that patient who had surgical intervention had a quicker radiological union and returned to work earlier. [9]
Only very small number of patient had a delayed fixation following nonunion but this did not have an impact on the final outcome of surgery, which is consistent with Potter et al. who showed that timing of surgical fixation did not result in significant difference in the overall function or satisfaction outcome of surgery. [21] This lends support to the argument that surgery can be reserved for those patients who fail conservative treatment in the absence of absolute indications for acute surgical fixation.
The minor complications encountered have been reported in previous studies, [4],[9],[11],[12],[14] and the prominence of the plate because of the subcutaneous nature of the clavicle is a major factor in plate removal regardless of the presence of any symptoms. [22] The plate is usually placed on the anterior-superior side of the clavicle where it provides the best stability [23] but also lies directly under the incision causing the irritation. This could be improved by the difficult positioning of the plate infraclavicularly as it has been shown to confer a better visual analogue score [4] and reduce rate of plate removal [24] but bothersome hardware is still reported. Another way is by using intermedullary fixation device which improves the cosmetic appearance [25] but confer less rigid fixation. [13] In our study, we could not identify one single factor associated with high metal work removal but almost all the plates that were removed were from those patients treated acutely. Furthermore, half of the female patients had their plates removed.
We did not encounter major complications. Authors however reported complications, such as non-union (although the rate is far less than nonoperative management), infection, lung damage, neurovascular injuries, hardware failure, and re-fracturing of the clavicle. [4],[11],[12],[13],[14],[22],[25]
In conclusion, the conservative treatment remains the treatment of choice for simple mid clavicle fractures, but for displaced and comminuted fractures surgical intervention is appropriate, especially when considering the overall outcome results. Our study included a small cohort of patients and suggests that the infraclavicular approach has lower rate of complications when compared with the direct approach. More importantly, it shows that there is a need to look into comparing the different surgical approaches in order to reduce the complications and the rate of metal work removal.
| References | | |
| 1. | Nowak J, Mallmin H, Larsson S. The aetiology and epidemiology of clavicular fractures. A prospective study during a two-year period in Uppsala, Sweden. Injury 2000;31:353-8. 
[PUBMED] |
| 2. | Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg 2002;11:452-6.
[PUBMED] |
| 3. | Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80:476-84.
[PUBMED] |
| 4. | Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD. Treatment of acute midshaft clavicle fractures: Systematic review of 2144 fractures: On behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma 2005;19:504-7.
[PUBMED] |
| 5. | Andersen K, Jensen PO, Lauritzen J. Treatment of clavicular fractures. Figure-of-eight bandage versus a simple sling. Acta Orthop Scand 1987;58:71-4.
[PUBMED] |
| 6. | McKee MD. Clavicle fractures in 2010: Sling/swathe or open reduction and internal fixation? Orthop Clin North Am 2010;41:225-31.
[PUBMED] |
| 7. | Rowe CR. An atlas of anatomy and treatment of midclavicular fractures. Clin Orthop Relat Res 1968;58:29-42.
[PUBMED] |
| 8. | Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc 1960;172:1006-11.
[PUBMED] |
| 9. | Vander Have KL, Perdue AM, Caird MS, Farley FA. Operative versus nonoperative treatment of midshaft clavicle fractures in adolescents. J Pediatr Orthop 2010;30:307-12.
[PUBMED] |
| 10. | Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am 2004;86:1359-65.
[PUBMED] |
| 11. | Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am 2007;89:1-10.
|
| 12. | Coupe BD, Wimhurst JA, Indar R, Calder DA, Patel AD. A new approach for plate fixation of midshaft clavicular fractures. Injury 2005;36:1166-71.
[PUBMED] |
| 13. | Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg Am 2009;91:447-60.
[PUBMED] |
| 14. | Jeray KJ. Acute midshaft clavicular fracture. J Am Acad Orthop Surg 2007;15:239-48.
[PUBMED] |
| 15. | Brinker MR, Edwards TB, O'Connor DP. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am 2005;87:676-7.
[PUBMED] |
| 16. | Bajuri MY, Maidin S, Rauf A, Baharuddin M, Harjeet S. Functional outcomes of conservatively treated clavicle fractures. Clinics (Sao Paulo) 2011;66:635-9.
[PUBMED] |
| 17. | Ledger M, Leeks N, Ackland T, Wang A. Short malunions of the clavicle: An anatomic and functional study. J Shoulder Elbow Surg 2005;14:349-54.
[PUBMED] |
| 18. | Hillen RJ, Burger BJ, Poll RG, de Gast A, Robinson CM. Malunion after midshaft clavicle fractures in adults. Acta Orthop 2010;81:273-9.
|
| 19. | McKee MD, Pedersen EM, Jones C, Stephen DJ, Kreder HJ, Schemitsch EH, et al. Deficits following nonoperative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg Am 2006;88:35-40.
[PUBMED] |
| 20. | Altamimi SA, McKee MD. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. Surgical technique. J Bone Joint Surg Am 2008;90 Suppl 2 Pt 1:1-8.
[PUBMED] |
| 21. | Potter JM, Jones C, Wild LM, Schemitsch EH, McKee MD. Does delay matter? The restoration of objectively measured shoulder strength and patient-oriented outcome after immediate fixation versus delayed reconstruction of displaced midshaft fractures of the clavicle. J Shoulder Elbow Surg 2007;16:514-8.
[PUBMED] |
| 22. | Bostman O, Manninen M, Pihlajamaki H. Complications of plate fixation in fresh displaced midclavicular fractures. J Trauma 1997;43:778-83.
|
| 23. | Iannotti MR, Crosby LA, Stafford P, Grayson G, Goulet R. Effects of plate location and selection on the stability of midshaft clavicle osteotomies: A biomechanical study. J Shoulder Elbow Surg 2002;11:457-62.
[PUBMED] |
| 24. | Collinge C, Devinney S, Herscovici D, DiPasquale T, Sanders R. Anterior-inferior plate fixation of middle-third fractures and nonunions of the clavicle. J Orthop Trauma 2006;20:680-6.
[PUBMED] |
| 25. | Boehme D, Curtis RJ Jr., DeHaan JT, Kay SP, Young DC, Rockwood CA Jr. Non-union of fractures of the mid-shaft of the clavicle. Treatment with a modified Hagie intramedullary pin and autogenous bone-grafting. J Bone Joint Surg Am 1991;73:1219- 26.
|
[Figure 1]
[Table 1], [Table 2], [Table 3], [Table 4]
| This article has been cited by | | 1 |
Complications of operative treatment of clavicle fractures in a Level I Trauma Center |
|
| Federico Persico,Eric Lorenz,David Seligson | | European Journal of Orthopaedic Surgery & Traumatology. 2013; | | [Pubmed] | [DOI] | | | 2 |
Operative Therapie der Klavikulapseudarthrose |
|
| C. Kirchhoff,I.J. Banke,M. Beirer,A.B. Imhoff,P. Biberthaler | | Operative Orthopädie und Traumatologie. 2013; 25(5): 483 | | [Pubmed] | [DOI] | |
|
|
|
|