| |


 |
| Year : 2012 | Volume
: 6
| Issue : 3 | Page : 86-89 |
|
|
|
|
|
ORIGINAL ARTICLE Mid-term results of arthroscopic subacromial decompression in patients with or without partial thickness rotator cuff tears
Ahmed S Eid, Amitabh J Dwyer, Andrew F. W. Chambler
Yeovil Elbow and Shoulder Service, Department of Trauma and Orthopaedic Surgery, Yeovil District Hospital, Higher Kingston, Yeovil, Somerset BA21 4AT, United Kingdom
Correspondence Address:
Amitabh J Dwyer
Department of Trauma and Orthopaedic Surgery, Yeovil District Hospital, Higher Kingston, Yeovil, Somerset BA21 4AT
United Kingdom
 Source of Support: None, Conflict of Interest: Approval For this Study: Granted by the Department of Clinical Governance, Yeovil District Hospital, Higher Kingston, Yeovil, Somerset BA21 4AT UK  | 6 |
DOI: 10.4103/0973-6042.102558

|
|
|
|
| Date of Web Publication | 17-Oct-2012 |
 Abstract Abstract | | |
Aim: To evaluate mid-term outcome in patients who underwent arthroscopic subacromial decompression (ASD) for shoulder impingement syndrome with intact and partially torn rotator cuffs.
Materials and Methods: A total of 80 consecutive patients (83 shoulders) who underwent ASD for impingement syndrome between 2003 and 2006 were analyzed. Mean age was 57.1 years. Patients' self-reported Oxford Shoulder Score (OSS) for pain was collected prospectively and was used as an instrument to measure surgical outcome.
Results: The mean initial and final OSS for patients with an intact rotator cuff was 26.1 and 40.3, respectively, at a mean follow up of 71.9 months (nearly 7 years). The mean initial and final OSS for patients with a partially torn articular sided tear was 22.6 and 41.9, respectively, at mean follow up of 70.7 months. Both groups showed significant sustained improvement (P < 0.0001). The mean improvement of OSS following ASD was statistically greater (P < 0.03) for partially torn rotator cuff group (19.3 points) as compared to those with normal rotator cuff (14.2 points).
Conclusion: Patients with dual pathology (partial rotator cuff tear and impingement) appreciated a significantly greater improvement following ASD compared to those with impingement alone. Both groups of patients had a similar final outcome at a mid-term follow up.
Level of Evidence: IV, retrospective study on consecutive series of patients.
Keywords: Arthroscopic subacromial decompression, rotator cuff, patient reported outcome measures, partial rotator cuff tear, surgical outcome
How to cite this article:
Eid AS, Dwyer AJ, Chambler AF. Mid-term results of arthroscopic subacromial decompression in patients with or without partial thickness rotator cuff tears. Int J Shoulder Surg 2012;6:86-9 |
| Introduction | |  |
Impingement syndrome is a common shoulder disorder involving repetitive microtrauma to the soft tissues in the subacromial space. [1] It results in significant pain, [1] reduction in function and quality of life for patients including being unable to lift weight and work in their usual employment. [2] The use of arthroscopy as an alternate technique for subacromial decompression was first published by Ellman [3] with short-term follow-up demonstrating 89% satisfaction at 2 to 5 years, [4] though proponents of open acromioplasty in the last decade found no essential difference in results between the two procedures except for cosmesis and personal preference. [5],[6] Further studies have validated arthroscopic subacromial decompression (ASD) as an effective treatment for subacromial impingement syndrome. [6],[7] It is also suggested that articular sided partial tears of the supraspinatus may not be repaired if less than 50% of the foot print is involved. [8] The aim of this study was to evaluate the difference in the outcome of treatment by ASD for impingement syndrome of the shoulder in presence of an intact or partially torn rotator cuff using the validated patient-reported Oxford Shoulder Score (OSS) as an assessment tool to measure the outcome [9] at 4 to 8 years of follow up.
| Materials and Methods | | |
A total of 80 consecutive patients (83 shoulders, 3 bilateral) with normal rotator cuff and partial rotator cuff tear who underwent ASD for impingement syndrome between September 2003 and August 2006 were included in the study. Patients were classified into two groups at arthroscopic examination of the shoulder and all partial tears were on the articular side of the rotator cuff [Table 1]. The mean age of patients was 57.1 years (range: 32-84 years, SD: 11.9). There were 38 men and 42 women with 49 right and 34 left shoulders.
Impingement syndrome of the shoulder was diagnosed on the basis of history and clinical examinations in which a Neer's sign [10] and Hawkins-Kennedy test [11] were positive in all patients. All patients had preoperative radiographic examination of the shoulder. Patients with full thickness rotator cuff tear, glenohumeral instability, frozen shoulder, cervical radiculitis, nerve compression, and coracoid impingement syndrome were excluded from our study. All patients had a minimum of 3 months of conservative treatment that included rest, anti-inflammatory medication, steroid injection(s) in the subacromial space, modification of activities, and physiotherapy before surgery. Majority of patients had preoperative imaging; however, the relation between comparisons of imaging vs findings has been published before. [12]
All patients were operated in the beach chair position under general anesthesia and interscalene nerve block. Cefuroxime (1.5 g) was administered at induction to all patients. The surgical procedure included glenohumeral joint arthroscopy from the standard posterior portal for assessment of articular cartilage of the humeral head and glenoid, inflammatory pathology of the rotator interval, integrity of the labrum and the long tendon of the biceps brachii, for any osteophytes and loose bodies in the inferior recess. The insertion of the rotator cuff (supraspinatus and infraspinatus) was inspected and either a normal appearance or partial tear was recorded. The tear size and its depth were intentionally not measured as this would bias the surgeon into repairing the partial tears and would defeat the purpose of the study. Bursal tears were not investigated but bursal side of cuff was inspected. The partial rotator cuff tears were debrided with 4.5-mm Elite shaver through an anterosuperior portal. The subacromial space was then entered from the posterior portal and the subacromial bursa, the bursal surface of rotator cuff, and the under surface of the acromion inspected. The ASD included excision of the subacromial bursa with a 4.5-mm Elite shaver (Smith Nephew), resection of the coracoacromial ligament from anteroinferior aspect of acromion was performed with Vulcan diathermy (Smith + Nephew), and the anterior inferior aspect of the anterior third of the acromion which included the enthesophytic spur was excised with a 5.5-mm burr (Smith & Nephew - Acromionizer). The operation was performed by the senior author or by an orthopedic trainee under direct supervision of the senior author. The postoperative regime was the same for all patients. This included application of a cryo cuff (North Star Orthopaedics) immediately after the operation for approximately two hours, monitoring of postoperative pain and neurovascular status, a sling to be discarded when shoulder comfortable (approximately 1-2 weeks), physiotherapy advice at discharge, and a physiotherapy follow up at 3 weeks postoperatively.
The assessment tool for comparison of clinical outcome in both groups was the patients' self-reported OSS for pain, consisting of 12 questions involving activities of daily routine. It has a best possible score of 48 and the least (minimum) score of 0. OSS is a patient-reported outcome measure and its reliability has been validated against Western Ontario Rotator Cuff Index (WORC) and Shoulder Pain and Disability Index (SPADI). [13] The OSS was collected prospectively preoperatively on the day of operation and compared at final follow up with scores obtained by post. The patients were assessed by an independent researcher who had not participated in treatment of these patients. Students t test was used to compare the two groups, with a P value of <0.05 considered significant.
| Results | | |
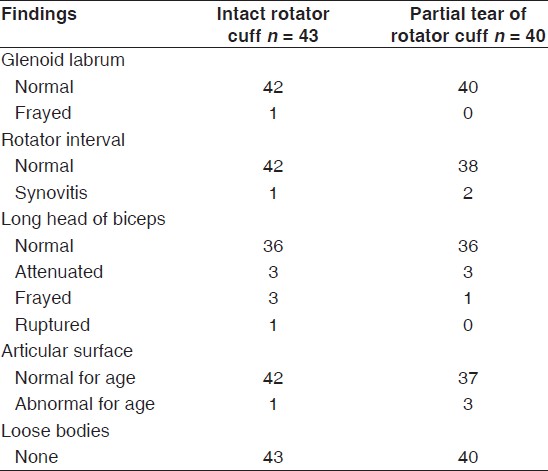
There were 41 patients (43 shoulders) with intact rotator cuff and 39 (40 shoulders) with partially torn rotator cuff. The intraoperative arthroscopic findings of glenohumeral joint are summarized in [Table 2]. The mean initial OSS for patients with an intact rotator cuff was 26.1 (SD: 9.1). This improved to 40.3 (SD: 10.7) at a mean follow up of 71.9 months (range: 53.7-82.6 months). The mean initial OSS for patients with a partially torn articular-sided tear was 22.6 (SD: 8.7) and this improved to 41.9 (SD: 10.1) at a mean follow up of 70.7 months (range: 58.1-88.5 months). The mean initial OSS of the partial tear group was 3.5 points lower than that of the normal rotator cuff group; however, this difference was not statistically significant (P = 0.075). The improvement of OSS following ASD was greater for partially torn rotator cuff group (mean: 19.3 points, SD: 10.2) as compared to those with normal rotator cuff (mean: 14.2 points, SD: 11.7) and this improvement of score was statistically significant (P = 0.03). The median increase of OSS among patients with partially torn rotator cuff was 19.5 and was greater than the median increase of OSS of 14 among patients with normal rotator cuffs. The mean final OSS of the partial tear group was slightly higher, by 1.6 points, than that of the normal rotator cuff group; however, this difference was once again not statistically significant (P = 0.46).
Overall, both groups showed significant and sustained improvement between OSS (P < 0.0001, 95% confidence interval from -18.13 to -11.29 for intact rotator cuff groups and 95% confidence from -22.59 to -15.77 for partially torn rotator cuffs) before and after the procedure, except two patients with intact rotator cuff who deteriorated by 1 and 17 points at a follow up of 78 and 57 months, respectively. None of the patients among the partially torn group showed a decrease of OSS from the initial score; however, there was no improvement of the score in one patient with initial and final score was 27 with a follow up of 65 months. The OSS of this patient, however, improved to 34 at one year but later dropped down to preoperative score. There were no complications in either group.
| Discussion | | |
Most partial-thickness rotator cuff tears in older patients occur on the articular side of the supraspinatus tendon, [14] possibly due to the critical zone of hypovascularity on the articular side that extends from the musculotendinous junction to within 5 mm of its insertion. [15] In contrast, tear of the bursal side of the rotator cuff is less common [14] as it has better ability to undergo a greater deformation by having greater tensile strength. [16] The above findings were reflected in all our patients who showed only articular-sided partial rotator cuff tears. Good to excellent mid- to long-term results have been achieved by acromioplasty without repair of the rotator cuff in articular-sided partial tears where less than 50% of the footprint was exposed and the outcome reached almost 95% of the value of a healthy shoulder after surgery, [8] however, little scientific information is available to support the 50% rule as a precise decision-making criterion where surgeons use their subjective discretion in the management. [17] Furthermore, a study reported that simple debridement of partial tears in combination with an acromioplasty is not sufficient and leads to progression to full thickness tears. [18] As all patients, bar one, had subjective improvement and did not require further investigation or treatment, any possible progression of the partial rotator cuff tear has been not possible to offer evidence to support or refute this study. Our results show that despite lower initial OSS, patients with partially torn rotator cuff had a similar final outcome as compared to the patients with intact rotator cuff at an average follow up of 5.9 years (71.9 months). Also, none of patients with partial rotator cuff tears had deterioration in their OSS at final follow up as compared to two patients in the intact rotator cuff group. They had developed signs and symptoms of osteoarthritis of the glenohumeral joint at follow up. Our results further exhibit a statistically greater mean improvement of the OSS among patients with partially torn rotator cuff, thus suggesting that partially torn rotator cuff patients may benefit more from ASD and that they have an eventual outcome similar to those with intact rotator cuff. The reasons for this are unclear. It may be that the subacromial decompression offers a better biomechanical environment for the damaged tendon to function compared to their normal counterparts.
Our study is a retrospective analysis of prospectively collected OSS data and does have a drawback of having a relatively small number of patients in each group. Mid-term results show that subacromial decompression alone gives similar results in both groups; however, prediction of long-term outcome cannot be made. The partial tears were diagnosed arthroscopically but they were not further divided as per Ellman's classification [19] and therefore our results may have a confounding factor leading to biased results.
| Conclusion | | |
Our study suggests that patients with intact and partially torn rotator cuff showed improvement of OSS for pain at a mid-term follow up following ASD. Patients with dual pathology (partial rotator cuff tear and impingement) appreciated a significant greater improvement as compared to those with impingement alone. Both groups had a similar final outcome revealing that a partial rotator cuff tear may not need to be addressed if found coincidentally at surgery, particularly if consented for a subacromial decompression alone.
| Acknowledgments | | |
Approval For this Study: Granted by the Department of Clinical Governance, Yeovil District Hospital, Higher Kingston, Yeovil, Somerset BA21 4AT UK.
| References | | |
| 1. | Nielsen KD, Wester JU and Lorentsen A. The shoulder impingement syndrome: the results of surgical decompression. J Shoulder Elbow Surg 1994;3:12-6. 
|
| 2. | Chipchase LS, O'Connor DA, Costi JJ, Krishnan J. Shoulder impingement syndrome: Preoperative health status. J Shoulder Elbow Surg 2000;9:12-5.
[PUBMED] |
| 3. | Ellman H, Kay SP. Arthroscopic subacromial decompression for chronic impingement. Two to five-year results. J Bone Joint Surg Br 1991;73:395-8.
[PUBMED] |
| 4. | Ellman H. Arthroscopic subacromial decompression: analysis of one to three-year results. Arthroscopy 1987;3:173-81.
[PUBMED] |
| 5. | Husby T, Haugstvedt JR, Brandt M, Holm I, Steen H. Open versus arthroscopic subacromial decompression: A prospective randomised study of 34 patients followed for 8 years. Acta Orthop Scand 2003;74:408-14.
[PUBMED] |
| 6. | Rao SE, Muzammil S, Hobbs NJ. Subacromial decompression for shoulder impingement syndrome. J Coll Physicians Surg Pak 2006;16:208-11.
[PUBMED] |
| 7. | Roye RP, Grana WA, Yates CK. Arthroscopic subacromial decompression: two to seven year follow-up. Arthroscopy 1995;11:301-6.
[PUBMED] |
| 8. | Liem D, Alci S, Dedy N, Steibeck J, Marquardt B, Mollenhoff G. Clinical and structural results of partial supraspinatus tears treated by subacromial decompression without repair. Knee Surg Sports Traumatol Arthrosc 2008;16:967-72.
|
| 9. | Dawson J, Rogers K, Fitzpatrick R, Carr A. Oxford shoulder score revisited. Arch Orthop Trauma Surg 2009;129:119-23.
[PUBMED] |
| 10. | Neer CS 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: A preliminary report. J Bone Joint Surg Am 1972;54:41-50.
[PUBMED] |
| 11. | Hawkins RJ, Kennedy JC. Impingement syndrome in athletes. Am J Sports Med 1980;8:151-8.
[PUBMED] |
| 12. | Ferri M, Finlay K, Popowich T, Stamp G, Schuringa P, Friedman L. Sonography of full-thickness suprapinatus tears: Comparison of patient positioning technique with surgical correlation. AJR Am J Roentgenol 2005;184:180-4.
[PUBMED] |
| 13. | Ekeberg OM, Bautz-Holter E, Tveita EK, Keller A, Juel NG, Brox JI. Agreement, reliability and validity in 3 shoulder questionnaires in patients with rotator cuff disease. BMC Musculoskelet Disord 2008;68:1-9.
|
| 14. | Wolff AB, Sethi P, Sutton KM, Covey AS, Magit DP, Medvecky M. Partial-thickness rotator cuff tears. J Am Acad Orthop Surg 2006;14:715-25.
[PUBMED] |
| 15. | Lohr JF, Uhthoff HK. The microvascular pattern of the supraspinatus tendon. Clin Orthop Relat Res 1990;254:35-8.
[PUBMED] |
| 16. | Nakajima T, Rokuuma N, Hamada K, Tomatsu T, Fukuda H. Histologic and biomechanical characteristics of the supraspinatus tendon: Reference to rotator cuff tearing. J Shoulder Elbow Surg 1994;3:79-87.
[PUBMED] |
| 17. | Pedowitz RA, Higashigawa K, Nguyen V. The "50% Rule" in arthroscopic and orthopaedic surgery. Arthroscopy 2011 Sep 1. [Epub ahead of print] doi:10.1016/j.arthro.2011.06.014
|
| 18. | Kartus J, Kartus C, Rostgard-Christensen L, Sernert N, Read J, Perko M. Long-term clinical and ultrasound evaluation after arthroscopic acromioplasty in patients with partial rotator cuff tears. Arthroscopy 2006;22:44-9.
|
| 19. | Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop 1990;254:64-74.
[PUBMED] |
[Table 1], [Table 2]
|