|
| Article Access Statistics | | | Viewed | 1533 | | | Printed | 56 | | | Emailed | 0 | | | PDF Downloaded | 6 | | | Comments | [Add] | | | Cited by others | 1 | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2012 | Volume
: 6
| Issue : 3 | Page : 99-100 |
|
|
|
|
|
LETTER TO THE EDITOR Latrogenic glenoid rim fracture during manipulation of a posterior dislocation
Tobias K. A. Baring, Philip M Ahrens
Department of Orthopaedic Surgery, Royal Free Hospital, Pond Street, London NW3 2QG, United Kingdom
Correspondence Address:
Tobias K. A. Baring
Department of Orthopaedic Surgery, Royal Free Hospital, Pond Street, London NW3 2QG
United Kingdom
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/0973-6042.102569

|
|
|
|
| Date of Web Publication | 17-Oct-2012 |
How to cite this article:
Baring TK, Ahrens PM. Latrogenic glenoid rim fracture during manipulation of a posterior dislocation. Int J Shoulder Surg 2012;6:99-100 |
Sir,
A 35 year old right hand dominant man fell off his mountain bike directly onto the anterior aspect of his left shoulder. Both initial and repeat adequate radiographs clearly showed a posterior dislocation of the left shoulder with a reverse Hill-Sacs lesion but no evidence of a glenoid fracture [1] [Figure 1]. Several attempts using both Kocher's technique [2] and the Hippocratic method [3] were made to reduce the joint in A + E with the use of intravenous midazolam and fentanyl, and inhaled entonox to sedate the patient. The post-reduction films showed the shoulder remained dislocated. No further attempt was made to perform a closed reduction. Computed tomography (CT) was performed later the same day, which showed the dislocated joint, a large reverse Hill-Sacs lesion, and the glenoid fracture which was displaced laterally into the defect [Figure 2]. The following day, the patient underwent open reduction and a modified MacLaughlin procedure. [4] The glenoid fracture reduced spontaneously into an anatomical position following reduction of the joint and therefore did not need surgical fixation.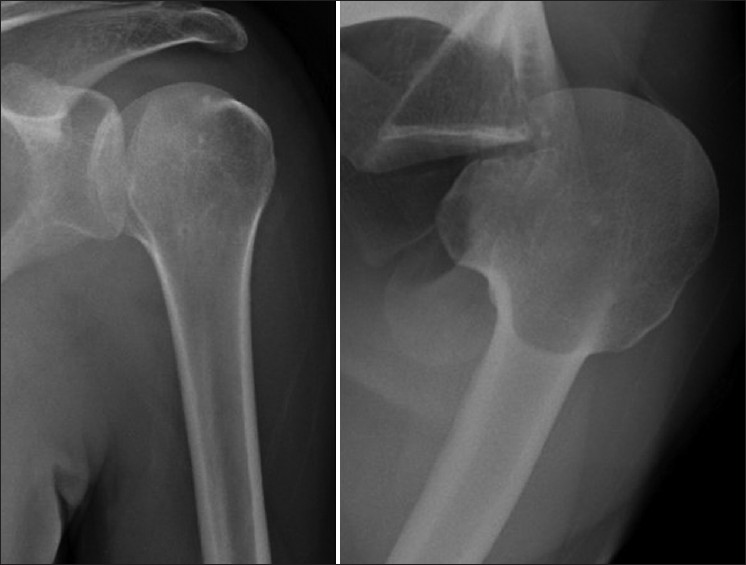 | Figure 1: Anteroposterior and axillary views of the left shoulder showing a posterior dislocation
Click here to view |
 | Figure 2: Axial CT of the left shoulder showing the dislocated shoulder with the reverse Hill-Sacs lesion (RH) and laterally displaced fracture of the posterior glenoid rim (G)
Click here to view |
We are not aware of a similar previous case where closed manipulation of a posteriorly dislocated shoulder has caused a fracture of the posterior rim of the glenoid. In this case, external rotation of the joint during incorrectly applied Kocher's technique could potentially exert enough force through the glenoid rim for it to fracture. Following the initial manipulation and iatrogenic injury, it may have been that the laterally displaced glenoid rim fracture then prevented successful reduction during closed manipulation. As the glenoid fracture was initially lateral and reduced following an open reduction, we felt that fixation was not required as this was not a typical Bankart lesion.
It would be reasonable to advise that when there is a significant delay to the diagnosis and management of a shoulder posterior dislocation, A + E staff should not attempt reduction. It would be more appropriate to seek specialist advice given that soft tissues are likely to be less pliable, and therefore there is potentially an increased risk of complication or failure to achieve reduction. We would also consider a CT scan prior to manipulation to rule out an occult fracture.
An error was made by using Kocher's technique to attempt to reduce a posterior dislocation. Furthermore, the patient was placed in a simply broad arm sling after manipulation, internally rotating the joint and in the presence of a large anterior reverse Hill-Sacs lesion. This may be another cause for failure of closed reduction. An appropriate method for reducing shoulder posterior dislocation is with abduction and external rotation or the Hippocratic technique, and once reduced, an external rotation brace should be applied.
 References References | |  |
| 1. | Connell DA, Potter HG. Magnetic resonance evaluation of the labral capsular ligamentous complex: a pictorial review. Australas Radiol 1999;43:419-26. 
[PUBMED] |
| 2. | Hussein MK. Kocher's method is 3,000 years old. J Bone Joint Surg Br 1968;50:669-71.
[PUBMED] |
| 3. | Waldron VD, Hazel D. Tips of the trade #37. Technique for reduction of shoulder dislocation. Orthop Rev 1991;20:563, 6.
[PUBMED] |
| 4. | Finkelstein JA, Waddell JP, O'Driscoll SW, Vincent G. Acute posterior fracture dislocations of the shoulder treated with the Neer modification of the McLaughlin procedure. J Orthop Trauma 1995;9:190-3.
[PUBMED] |
[Figure 1], [Figure 2]
| This article has been cited by | | 1 |
Locked posterior dislocation of the shoulder joint: Report of two cases |
|
| Sung-Chun Lin,Hsin-Pai Lee,Chih-Ju Chen,Yen-Hsuan Jean | | Formosan Journal of Musculoskeletal Disorders. 2013; | | [Pubmed] | [DOI] | |
|
|
|
|
|











