|
| Article Access Statistics | | | Viewed | 1192 | | | Printed | 54 | | | Emailed | 0 | | | PDF Downloaded | 4 | | | Comments | [Add] | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2012 | Volume
: 6
| Issue : 4 | Page : 135-136 |
|
|
|
|
|
LETTER TO THE EDITOR A peculiar periprosthetic humeral fracture managed in a simple but effective way
Abdelsalam Eid, Tarek A Elhewala
Department of Orthopaedic Surgery, Faculty of Medicine, Zagazig University, Egypt
Correspondence Address:
Abdelsalam Eid
Department of Orthopaedic Surgery, Faculty of Medicine, Zagazig University; 5 Mahfouz street, From Ahmed Ismail street, Zagazig, 44511
Egypt
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.106228

|
|
|
|
| Date of Web Publication | 18-Jan-2013 |
How to cite this article:
Eid A, Elhewala TA. A peculiar periprosthetic humeral fracture managed in a simple but effective way. Int J Shoulder Surg 2012;6:135-6 |
Sir,
Periprosthetic fractures of the humerus are rare injuries. No large series exist, with most articles reporting only a few cases. [1],[2],[3],[4] A few classification schemes exist sharing the same principles of classifying the fracture according to the site of the fracture and stability of the fixation of the prosthesis. [1],[2],[3],[4]
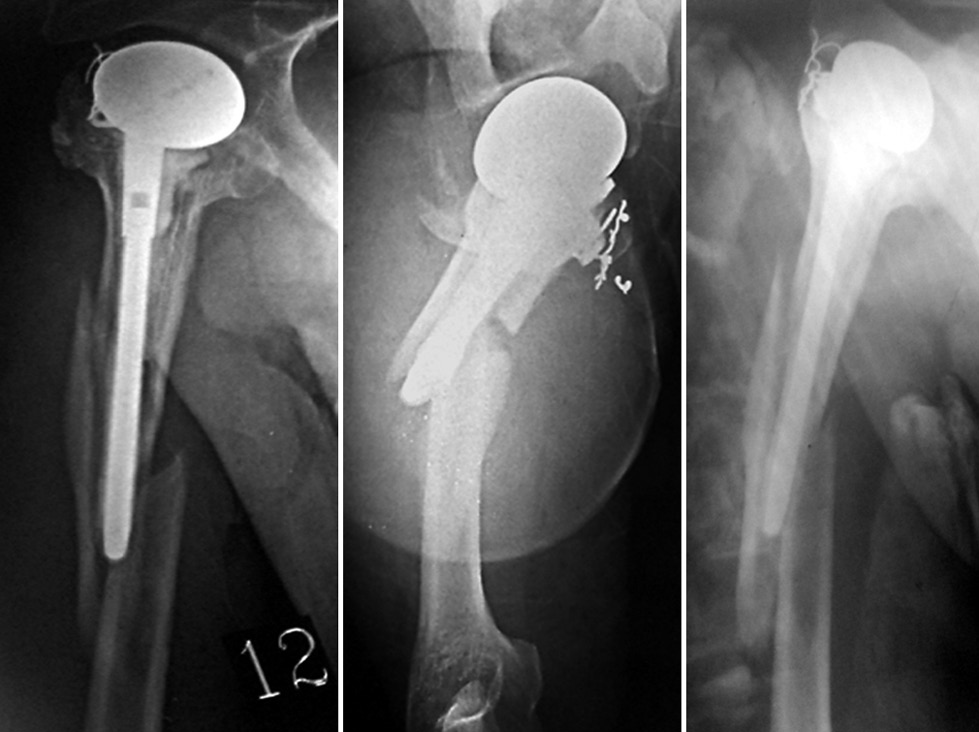
A 40-year-old male with a four-part posterior fracture dislocation of the right shoulder had been managed with a cemented shoulder hemiarthroplasty. The functional result postoperatively was excellent, with a Constant score of 95. Four years after the index operation, the patient sustained a periprosthetic humeral fracture [Figure 1]. X-ray showed the fracture to be spiral with a large butterfly and centred around the tip of the prosthesis. This pattern was not described in the different classifications of periprosthetic humeral fractures to the best of our knowledge. The closest category that fits is B1 according to the classification of Worland et al., [4] which is a spiral fracture located around the stem with a stable prosthesis. The prosthesis was judged to be stable; therefore, the decision was to keep the prosthesis and fix the fracture.
After exposing the fracture posteriorly and securing the radial nerve, the distal fixation was performed first using three 4.5 mm AO cortical screws that were applied in a compression/lag mode to fix the large butterfly to the main distal fragment, converting the fracture to a two-part fracture. Next, the butterfly was secured to the main proximal fragment using a single double-stranded cerclage loop. The wound was closed in layers and a U-shaped slab was applied.
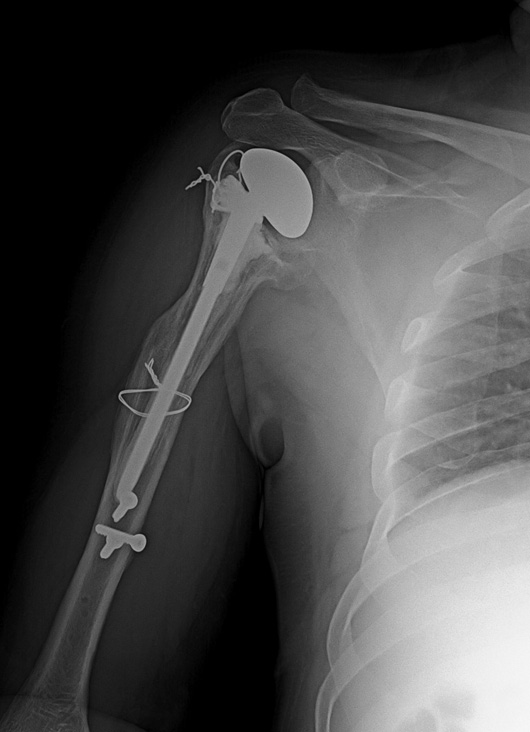
The patient was discharged the next day. At 4 weeks, the slab was removed and a control X-ray was obtained. Early callus was noted at the fracture site and the patient was instructed to perform assisted active mobilization of the elbow and shoulder. X-ray obtained at 2 months showed union at the fracture site and, clinically, there was no pain and a good range of motion of both the shoulder and the elbow as well as good muscle power. At 2 years' follow-up, the Constant score was 89 and the DASH score was 4. The patient was able to return to his work [Figure 2].
For such a fracture, it was definitely impossible to use any sort of screws around the prosthesis as the stem and cement filled the medullary cavity and the remaining cortex was too thin to provide purchase for any kind of screw. Therefore, a form of circumferential surface fixation was contemplated. This mandated the use of the posterior approach to clearly visualize and protect the radial nerve. Plates such as Mennen and cable-plate systems were not available in our setting, and were also economically not feasible. The utilized form of minimal fixation kept the fragments bound together until healing occurred. A U-shaped plaster slab and a pouch arm sling minimized elbow shoulder movement.
 References References | |  |
| 1. | Steinmann SP, Cheung EV. Treatment of periprosthetic humerus fractures associated with shoulder arthroplasty. J Am Acad Orthop Surg 2008;16:199-207. 
[PUBMED] |
| 2. | Campbell JT, Moore RS, Lannotti JP, Norris TR, Williams GR. Periprosthetic humeral fractures: Mechanisms of fracture and treatment options. J Shoulder Elbow Surg1998;7:406-13.
|
| 3. | Kumar S, Sperling JW, Haidukewych GH, Cofield RH. Periprosthetic humeral fractures after shoulder arthroplasty. J Bone Joint Surg 2004;86-A:680-9.
[PUBMED] |
| 4. | Worland RL, Kim DY, Arredondo J. Periprosthetic humeral fractures: Management and classification. J Shoulder Elbow Surg 1999;8:590-4.
[PUBMED] |
[Figure 1], [Figure 2]
|
|