| |


 |
| Year : 2014 | Volume
: 8
| Issue : 1 | Page : 27-30 |
|
|
|
|
|
CASE REPORT Combination of a floating clavicle and a posterior shoulder dislocation: An "Unhappy Triad" of the shoulder girdle
Benedikt Schliemann, Christina Theisen, Clemens Kösters, Andre Weimann
Department of Trauma, Hand and Reconstructive Surgery, University Hospital Münster, Waldeyerstraße 1, 48149 Münster, Germany
Correspondence Address:
Benedikt Schliemann
University Hospital Münster, Department of Trauma, Hand and Reconstructive Surgery, Waldeyerstraße 1, 48149 Münster
Germany
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.131853
 |
|
|
|
| Date of Web Publication | 2-May-2014 |
 Abstract Abstract | | |
We present a case of a 31-year-old man who suffered from a floating clavicle in combination with a reverse Hill-Sachs lesion of his right shoulder girdle after a bicycle accident. Operative treatment was performed using minimal-invasive and arthroscopically assisted techniques.
We strongly recommend an early CT scan with later 3-dimensional reconstruction to detect and fully understand these complex injuries.
Keywords: Floating clavicle, lateral clavicle fracture, posterior shoulder dislocation, reverse Hill-Sachs lesion
How to cite this article:
Schliemann B, Theisen C, Kösters C, Weimann A. Combination of a floating clavicle and a posterior shoulder dislocation: An "Unhappy Triad" of the shoulder girdle. Int J Shoulder Surg 2014;8:27-30 |
| Introduction | |  |
A floating clavicle or bipolar clavicle dislocations are rare injuries usually resulting from major trauma. The first description of this rare injury was by Porral in 1831. [1] Bipolar fracture dislocation of the clavicle seems to be even rare than dislocation only. To the best of our knowledge, there are only two reports on a combination of a lateral and medial clavicle fracture in combination with SC joint dislocations. [2],[3]
Traumatic posterior shoulder dislocation represents a rare injury, accounting for only about 1-5% of all glenohumeral dislocations. [4],[5] Posterior dislocation of the glenohumeral joint may result in an impression fracture of the anterior aspect of the humeral head, the so-called reverse Hill-Sachs lesion or Malgaigne fracture. The treatment depends on the size of the defect and varies from conservative treatment to surgical options such as bone grafting, subscapularis tendon transfer, and arthroplasty. [6]
We present a case of a 31-year-old man who suffered from a combination of a floating clavicle caused by a lateral clavicle fracture and a SC joint dislocation and a reverse Hill-Sachs lesion of his right shoulder girdle after a bicycle accident.
| Case Report | | |
Five days after he sustained a bicycle accident, the patient was referred to our hospital from his general practitioner with pain and loss of function of his right shoulder. Clinical examination showed a prominence of the SC joint, a massive haematoma of the shoulder and pain on pressure over both the medial and lateral aspect of the clavicle. The CT scan revealed a floating clavicle with a lateral clavicle fracture type II b according to Neer, a fracture of the medial end of the clavicle with anterior dislocation of the SC joint (type III according to Allman, [Figure 1]). In addition, a reverse Hill-Sachs lesion was apparent, affecting approximately 20% of the articular surface of the humeral head [Figure 2]. Concomitant lesions of the rotator cuff and the long head of the biceps could be excluded by ultrasound. Surgery was performed with the patient placed in a modified beach chair position. Preoperative examination under general anaesthesia confirmed the highly unstable SC joint. First, the more displaced SC joint was exposed, revealing a complete rupture of the SC ligaments. After reduction, stabilization of the joint was achieved with a figure-of-eight PDS cerclage. After SC joint reconstruction, open reduction and internal fixation of the lateral clavicle fracture were performed using a 2.4 mm T-plate designed for the distal radius (Fa. Synthes, Umkirch, Germany). 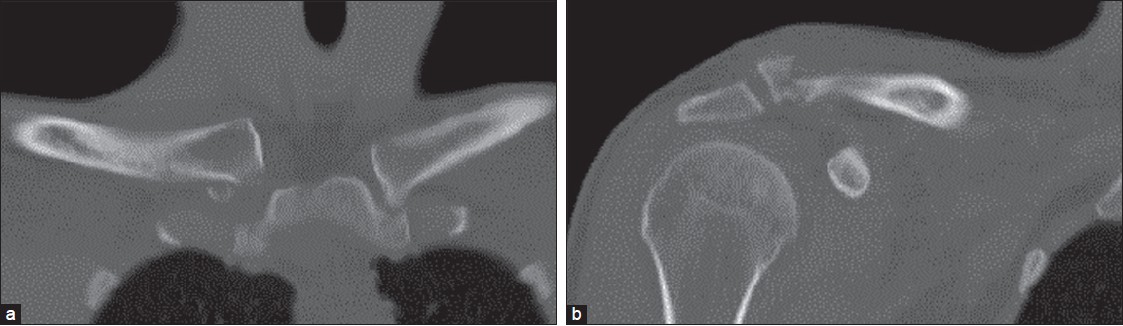 | Figure 1: Preoperative CT scan shows a fracture dislocation of the SC Joint (a) and a lateral clavicle fracture (b)
Click here to view |
 | Figure 2: Arthroscopy of the glenohumeral joint shows the reverse Hill-Sachs lesion (a). The defect was elevated indirectly using an aiming device originally designed for posterior cruciate ligament reconstruction (b, c)
Click here to view |
Subsequent arthroscopy of the glenohumeral joint confirmed the reverse Hill-Sachs lesion [Figure 2]a. Using an aiming device originally designed for posterior cruciate ligament reconstruction (Fa. Karl Storz, Tuttlingen, Germany), the defect was elevated indirectly through an additional lateral stab incision. Additional support by a bone graft was not required [Figure 2]b,c. No concomitant intra-articular lesion of the glenohumeral joint such as labral or rotator cuff injuries could be detected. The arm was immobilized in a brace with the arm at the side in 15 degrees of abduction for 6 weeks post-operatively. Early passive mobilization was allowed with abduction and forward flexion restricted to 90 degrees. After 6 weeks, the patient was allowed to start active exercise with free range of motion.
Radiographs at follow-up 8 weeks after surgery showed a bony union of the fractures and stable reduction of both the SC and AC joint [Figure 3]a,b. At follow-up 6 months postoperatively, the patient presented with free range of motion and only mild discomfort during physical activity. He did not show any signs of recurrent instability, neither at the clavicle nor at the glenohumeral side. 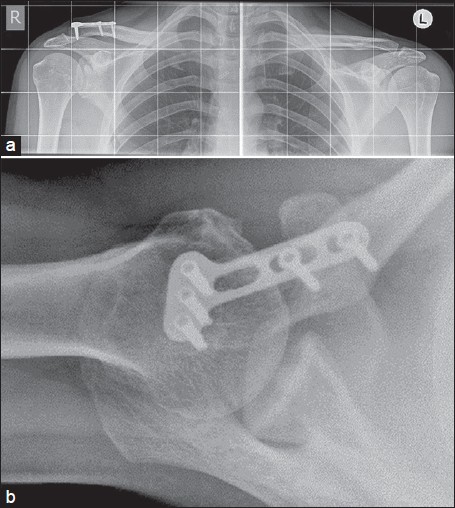 | Figure 3: Radiographs at follow-up showed a bony union of the fractures and stable reduction of both the SC and AC joint (a). The articular surface of the humeral head is reconstructed after arthroscopically assisted elevation of the defect (b)
Click here to view |
One year after trauma, the plate over the lateral clavicle was removed due to implant-related irritations. The patient did not complain about any other symptoms or complications.
The X-ray examination after 1 year showed fracture consolidation, stable AC- and SC joints and a congruency of the humeral head surface.
Ethics Committee approval was not required for this case report. However, written consent to use his data for publication was obtained from the patient before submission.
| Discussion | | |
The present case demonstrates the successful surgical treatment of a rare shoulder girdle injury. However, its rarity inhibits the development of a standardized treatment strategy. If bipolar clavicle dislocation occurs without fractures, conservative treatment may be successful. Caranfil, Jain, Cook and Horrowitz and others reported on good results after conservative treatment of these injuries. [7],[8],[9] In contrast, Sanders found superior results in his patients which were treated operatively for bipolar clavicle dislocation. [10] He presented a series of six patients with a bipolar clavicle injury. Only in two elderly patients conservative treatment was successful, whereas surgery was required in four younger men because of continuing pain. [10]
Furthermore, the applied surgical procedures vary from minimal-invasive techniques to extensive open surgery. Whereas k-wires are widely used, [11],[12],[13] other authors achieved reduction and fixation of both dislocations with a hook plate. This requires an extensive surgical approach. [14],[15] However, functional results do not differ considerably in those cases and implant removal is usually necessary in all described techniques.
In our patient, both the SC joint and the reverse Hill-Sachs lesion were surgically addressed in a minimal-invasive approach. The lateral clavicle fracture was fixed with a 2.4 mm T-plate. This plate has a very low profile. Therefore, irritations related to the implant seem less likely. In a series of 14 patients with an unstable lateral clavicle fracture, we treated 7 patients using this T-plate and 7 patients with a preshaped locking compression plate which is considerably thicker. Implant removal was only required in the latter group because of implant-related irritations over the lateral clavicle. [16] However, in this case, the plate had to be removed due to soft tissue irritations anyway.
Regarding the treatment of the reverse Hill-Sachs lesion, there is consent in literature that early treatment and anatomic reconstruction of the defect result in better outcome than delayed surgery with non-anatomic procedures. [6] In contrast to anterior instability, in which the labroligamentous lesion accounts for recurrent instability, the size of the reverse Hill-Sachs defect determines the degree of instability in posterior dislocation. A reverse Hill-Sachs lesion may lead to a locking of the humeral head behind the posterior glenoid rim. These patients present with decreased or completely nullified external rotation with the arm in elastic internal rotation. [17]
In the present case, the anterior humeral head defect was elevated arthroscopically assisted with the use of a special aiming device. Elevation of the defect has proven to be clinically and radiographically successful as it restores the normal anatomy of the joint surface of the humeral head. [16] If elevation and support of the defect alone is not possible, auto- or allograft may be used, also leading to satisfying result. [5] Diklic reported on a series of 13 patients who underwent reconstruction of a humeral head defect of 25 to 50% after posterior shoulder dislocation. The mean constant score was 86.8 at a follow-up of 54 months. No recurrent instability was observed. [18] In contrast, non-anatomic reconstructions such as the McLaughlin procedure or its modifications and arthroplasty are associated with significantly worse results. [6],[10],[19],[20] To avoid worse functional results, we therefore recommend meticulous clinical and radiographic evaluation including a CT scan.
| Conclusion | | |
Anatomic reconstruction of the AC and SC joint as well as the humeral head defect with minimal-invasive and arthroscopically assisted surgical techniques can lead to satisfying results in a patient with bipolar clavicle fracture dislocation and a reverse Hill-Sachs lesion. If the complexity of these rare injuries cannot be excluded from plain radiographs, CT scan with later 3-dimensional reconstruction is indispensable to detect and fully understand these complex injuries.
| References | | |
| 1. | Porral D. Observation d'une double luxation de la clavicule droite. J Univ Hebd Med Chir 1831;2:78-82. 
|
| 2. | Serra JT, Tomas J, Batalla L, Pedemonte J, Pacha D, Molero V, et al. Traumatic floating clavicle: A case report. J Orthop Trauma 2011;25:e98-9.
|
| 3. | Thomas CB Jr., Friedman RJ. Ipsilateral sternoclavicular dislocation and clavicle fracture. J Orthop Trauma 1989;3:355-7.
|
| 4. | Blasier RB, Burkus JK. Management of posterior fracture-dislocations of the shoulder. Clin Orthop Relat Res 1988;232:197-204.
|
| 5. | Gerber C, Lambert SM. Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-82.
|
| 6. | Schliemann B, Muder D, Gessmann J, Schildhauer TA, Seybold D. Locked posterior shoulder dislocation: treatment options and clinical outcomes. Arch Orthop Trauma Surg. 2011;131(8):1127-34.
|
| 7. | Caranfil R. [Bipolar luxation of the clavicle. A case report]. Acta Orthop Belg 1999;65:102-4.
|
| 8. | Cook F, Horowitz M. Bipolar clavicular dislocation. Report of a case. J Bone Joint Surg Am 1987;69:145-7.
|
| 9. | Jain AS. Traumatic floating clavicle. A case report. J Bone Joint Surg Br 1984;66:560-1.
|
| 10. | Sanders JO, Lyons FA, Rockwood CA Jr. Management of dislocations of both ends of the clavicle. J Bone Joint Surg Am 1990;72:399-402.
|
| 11. | Arenas AJ, Pampliega T, Iglesias J. Surgical management of bipolar clavicular dislocation. Acta Orthop Belg 1993;59:202-5.
|
| 12. | Echo BS, Donati RB, Powell CE. Bipolar clavicular dislocation treated surgically. A case report. J Bone Joint Surg Am 1988;70:1251-3.
|
| 13. | Tanlin Y. Ipsilateral sternoclavicular joint dislocation and clavicle fracture. J Orthop Trauma 1996;10:506-7.
|
| 14. | Dudda M, Kruppa C, Schildhauer TA. Post-traumatic bipolar dislocation of the clavicle: Is operative treatment reasonable? Unfallchirurg 2013;116:176-9.
|
| 15. | Schemitsch LA, Schemitsch EH, McKee MD. Bipolar clavicle injury: Posterior dislocation of the acromioclavicular joint with anterior dislocation of the sternoclavicular joint: A report of two cases. J Shoulder Elbow Surg 2011;20:e18-22.
|
| 16. | Schliemann B, Roßlenbroich SB, Schneider KN, Petersen W, Raschke MJ, Weimann A. Surgical treatment of vertically unstable lateral clavicle fractures (Neer 2b) with locked plate fixation and coracoclavicular ligament reconstruction. Arch Orthop Trauma Surg 2013;133:935-9.
|
| 17. | Cooper A. On the dislocations of the os humeri upon the dorsum scapulae, and upon fractures near the shoulder joint. Guy's Hosp Rep 1839;4:265-84.
|
| 18. | Diklic ID, Ganic ZD, Blagojevic ZD, Nho SJ, Romeo AA. Treatment of locked chronic posterior dislocation of the shoulder by reconstruction of the defect in the humeral head with an allograft. J Bone Joint Surg Br 2010;92:71-6.
|
| 19. | Gavriilidis I, Magosch P, Lichtenberg S, Habermeyer P, Kircher J. Chronic locked posterior shoulder dislocation with severe head involvement. Int Orthop 2010;34:79-84.
|
| 20. | McLaughlin H. Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;24-A-3:584-90.
|
[Figure 1], [Figure 2], [Figure 3]
|













