| |


 |
| Year : 2014 | Volume
: 8
| Issue : 1 | Page : 34-37 |
|
|
|
|
|
SURGICAL TECHNIQUE Distal humerus shear-fractures: "Built-on" surgical technique
Jose M Rapariz1, Silvia Martin2, Aina Far-Riera1, Serafin Lirola-Palmero1
1 Department of Orthopedic Surgery, Son Llatzer Hospital, Palma de Mallorca, Spain
2 Department of Radiology, Son Llatzer Hospital, Palma de Mallorca, Spain
Correspondence Address:
Jose M Rapariz
C/Vista Alegre 23, 1 D, Palma de Mallorca - 07015
Spain
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.131856
 |
|
|
|
| Date of Web Publication | 2-May-2014 |
 Abstract Abstract | | |
When treating a distal humeral shear fracture, comminution of the lateral column may preclude the reconstruction of the lateral articular fragments.
In this article a new strategy for the management lateral column comminuted shear-fractures (LCCSF) is presented, called the "built-on" surgical technique. Three goals are obtained by this technique: (1) Restoration of the lateral column bone stock; (2) Provision of a solid scaffold for the repair of the lateral ulnar collateral ligament (LUCL); and (3) Provision of a sable platform for the reconstruction and fixation of the articular fragments.
We will obtain these goals through the following surgical steps:
1/ Reconstruction of the lateral trochlea.
2/ Reconstruction of the lateral column
3/ Fixation of the Capitellum
4/ Reconstruction of the LUCL
Keywords: Capitellar and trochlear fractures, distal humerus, fractures, lateral column, shear fractures
How to cite this article:
Rapariz JM, Martin S, Far-Riera A, Lirola-Palmero S. Distal humerus shear-fractures: "Built-on" surgical technique. Int J Shoulder Surg 2014;8:34-7 |
| Introduction | |  |
Isolated coronal injuries of the distal humerus involving the capitellum and trochlea are relatively rare. This form of shear fracture (SF) may also be associated with more complex distal humeral fractures and elbow fracture-dislocations with concomitant ligamentous injuries. Coronal plane SFs are often the result of a relatively low-energy fall on an out-stretched arm. Direct axial compression transmitted to the capitellum by the radial head with the elbow in a semi-flexed position may create a shear capitellum and trochlea fracture. [1]
Several classifications for partial articular fractures of the distal humerus have been described. [2] The most commonly used classification system is that of Bryan and Morrey. [3] Nevertheless, this classification system does not consider the lateral column bone stock. A solid lateral column is essential in order to obtain a good fixation of the articular fragments. Comminution of the lateral column may preclude the reconstruction of the lateral articular fragments. This is a crucial factor to bear in mind when the surgeon is planning the reconstruction strategy.
In this article a new strategy for the management lateral column comminuted shear-fractures (LCCSF) is presented, called the "built-on" surgical technique. Three goals are obtained by this technique:
- Restoration of the lateral column bone stock;
- Provision of a solid scaffold for the repair of the lateral ulnar collateral ligament (LUCL); and
- Provision of a sable platform for the reconstruction and fixation of the articular fragments.
| Case Report | | |
A 42-year-old man was hospitalized in our institution due to pain and deformity in his right elbow after a casual stair fall. The patient did not have any distal neurovascular impairment.
An X-ray showed an LCCSF. On the AP view there was a significant comminution of the lateral column. Trochlear sulcus involvement caused a subluxation of the ulno-humeral joint [Figure 1]. Articular fragments of the trochlea and capitellum were proximally displaced on the anterior aspects of the distal humerus. There was no involvement of radius or ulna [Figure 2]. 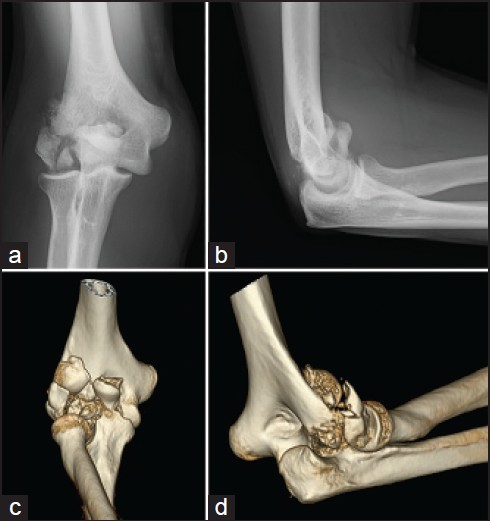 | Figure 1: Lateral column shear fracture with subluxation of the ulnohumeral joint (a) Articular fragments including trochlea and capitellum (b and c) and conminution of the lateral column (d)
Click here to view |
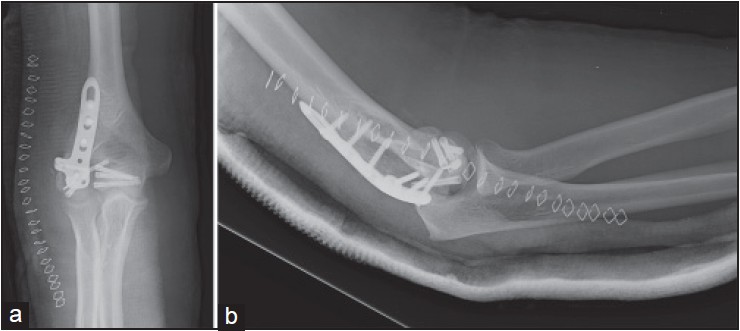 | Figure 2: Postop X-ray, after reconstruction with the "built-on" technique
Click here to view |
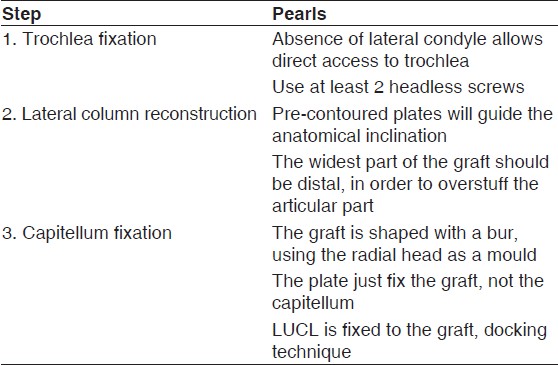
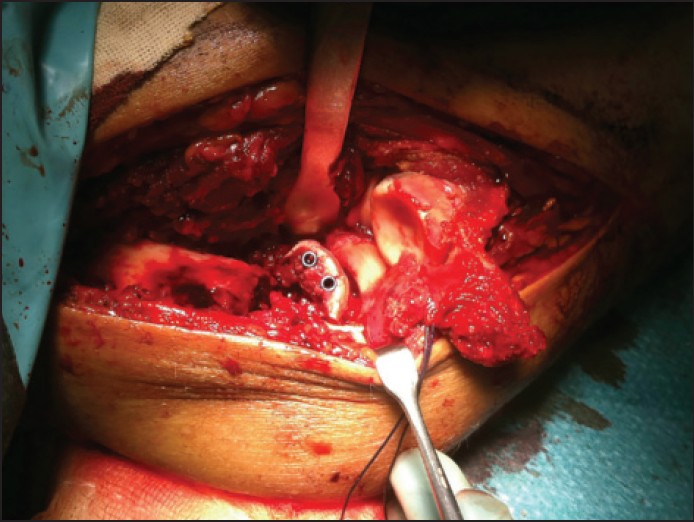
An extensile lateral approach through the avulsed epicondyle musculature was performed. The proximal insertion of the LUCL was torn. The smaller articular fragments were extracted, and the lateral trochlea fragment was fixed using 3 Acutrack® screws. The extensive comminution of the lateral column made direct fixation of the condylar fragments impossible. To bridge this defect, tricortical iliac bone graft (see surgical technique below) fixed with a posterior plate (Synthes® ) was used. This graft provides structural support not only to fix the condylar fragment but also for repair the LUCL [Table 1].
The elbow was immobilized in extension for 48 h. Two days after surgery, the patient was discharged using a dynamic splint, allowing active and passive ranges of motion between 45-100°. The brace was kept on for 12 weeks, and was only removed for physical therapy. At the 6 months follow-up appointment the patient had a flexion of -30° with an extension of 110 degrees, and pronation was complete. However, supination was limited to 50%, but the patient did not complain of any pain. The patient returned to his previous job as a technician. A second surgery for lateral column procedure [4] was proposed, but the patient refused.
| Discussion | | |
Fractures of the capitellum with extension to the medial trochlea constitute a difficult challenge for the orthopaedic surgeon. However, some of the fragments can be too small for any type of fixation, and some are impacted in the medullary canal of the distal humerus. On the other hand, anatomical reconstruction of trochlea and capitellum is crucial in order to achieve satisfactory results.
Most of these injuries are due to a shearing mechanism. Typically, the shearing forces produce an involvement of the anterior articular surface of the humerus, preserving not only the proximal end of the radius and ulna but also the columns of the distal humerus. These fractures are known as "coronal shear fractures." [1]
This report presents a coronal shear fracture with a unique feature not previously reported in the literature: Comminution of the lateral column. In this case, the lateral column was no longer a scaffold on which to fix the articular fragments. The absence of the lateral column bone stock made other surgical strategies necessary. As a result, most orthopaedic surgeons would opt for partial or total elbow arthroplasty in elderly patients. However, this option is not possible in young patients, making the reconstruction using the "built-on" technique may be the best alternative in such cases.
The "built-on" technique has the following advantages:
- It provides structural support of the tricortical graft, for the fixation of the articular fragments.
- It provides a stable scaffold on which to reconstruct the ulnar lateral collateral ligament, which is frequently injured.
- In the event of failure of the capitellum (necrosis, nonunion, or malunion) there should be sufficient bone stock in order to perform unicondylar arthroplasty.
Several classification systems have been described in the literature, but none of them have considered the lateral column comminution. [3],[2]
Ring described different patterns of distal humeral articular fractures. [2] The complexity and variability of this type of fracture makes it difficult to understand the fracture without computed tomography (CT) with three-dimensional (3D) reconstruction [Figure 2]. Computed tomography (CT) with three-dimensional (3D) reconstruction was recommended to enhance the preoperative assessment of the fracture and preoperative decision-making. [5],[2]
Most of these fractures can be exposed through an extensile lateral approach, although the antero-lateral approach has been recommended in the literature. [6] Ring recommended olecranon osteotomy for cases with medial extension, particularly when medial epicondyle is involved. [2] The "built-on" technique can be performed through the extensile lateral approach. [3] The comminution of the lateral column facilitates exposure and olecranon osteotomy is not required.
In conclusion, 3D-CT imaging is really helpful for coronal shear fractures of the distal humerus. Lateral column comminution should be recognised in the preoperative imaging, in order to perform an adequate surgical repair. The "built-on" technique is an excellent option for the reconstruction of coronal shear fractures with lateral column comminution in young patients.
First step: Reconstruction of the lateral trochlea
If there is involvement of the lateral trochlea, reconstruction of this is the first step to be performed. Reconstruction will allow a good anatomical position of the ulna, initially laterally subluxated. This step is critical for two reasons:
- Arc of motion in flexion and extension depends crucially on the humeral-ulnar joint reconstruction.
- If the lateral subluxation of the ulna is not reduced, the capitellum will remain lateralized, since the radial head is used as a template for the right situation of the capitellum [Figure 3].
 | Figure 3: Step 1: Reconstruction of the lateral trochlea with headless cannulated screws
Click here to view |
Second step: Reconstruction of the lateral column
After removal of the lateral column fragments, a tricortical iliac crest bone auto-graft is fixed with a posterior plate. Placing the tricortical graft so that its curvature recreates the anterior tilt of the lateral column is recommended. It is important to use pre-contoured plates, which serve as a guide for the anatomical inclination. The aim of the plate is tricortical graft fixation, not the capitellum fixation. The iliac crest graft must be ''overstuffed'' so that it can be shaped with a bur to fit the capitellum fragment [Figure 4]. | Figure 4: Step 2: Reconstruction of the lateral column with tricortical iliac crest bone graft
Click here to view |
Third step: Fixation of the capitellum
The bone graft is shaped with a bur in order to allow the right position of the capitellum. The radial head is used as a mould, checking the congruency along the range of motion. Fixation is obtained by headless screws introduced from the capitellum to the bone graft [Figure 5].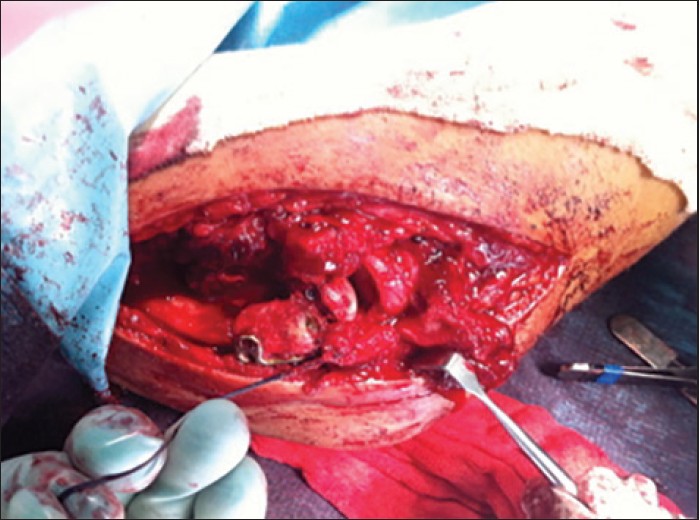 | Figure 5: Step 3: Fixation of the capitellum over the graft and ligament repair
Click here to view |
Fourth step: Reconstruction of the LUCL
The lateral ligament is repaired using the docking technique, although, once the lateral column bone stock has been restored, other techniques can be used, depending on the surgeon's preference.
| References | | |
| 1. | McKee MD, Jupiter JB, Bamberger HB. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 1996;78:49-54. 
|
| 2. | Ring D, Jupiter JB, Gulotta L. Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-8.
|
| 3. | Fractures of the distal humerus. In: Morrey BF, editors. The Elbow and Its Disorders. Philadelphia, PA: WB Saunders; 1985. p. 325-33.
|
| 4. | Mansat P, Morrey BF. The column procedure: A limited lateral approach for extrinsic contracture of the elbow. J Bone Joint Surg Am 1998;80:1603-15.
|
| 5. | Doornberg J, Lindenhovius A, Kloen P, van Dijk CN, Zurakowski D, Ring D. Two and three-dimensional computed tomography for the classification and management of distal humeral fractures. Evaluation of reliability and diagnostic accuracy. J Bone Joint Surg Am 2006;88: 1795-801.
|
| 6. | Imatani J, Morito Y, Hashizume H, Inoue H. Internal fixation for coronal shear fracture of the distal end of the humerus by the anterolateral approach. J Shoulder Elbow Surg 2001;10:554-6.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
[Table 1]
|