| |


 |
| Year : 2014 | Volume
: 8
| Issue : 2 | Page : 39-46 |
|
|
|
|
|
ORIGINAL ARTICLE Fascia lata allograft bridging of a rotator cuff tear in a rabbit animal model
Dimitrios Varvitsiotis1, Athanasios Papaspiliopoulos1, Vasiliki Vlachou2, John Feroussis1, Apostolos Papalois3, Xenofon Papacharalampous4, Panayotis N Soucacos5, Aristides Zoubos5
1 Department of Orthopedic Surgery, Asclepieion Voulas, 16673 Voula, Greece
2 Department of Pathology, General Hospital 'G. Gennimatas', 12462 Haidari, Athens, Greece
3 Department of Biomedics, laboratory of research and experiments, 12462 Haidari, Athens, Greece
4 Department of Radiology, University Hospital 'Areteion', 12462 Haidari, Athens, Greece
5 Department of Orthopedics, University Hospital 'Attikon', 12462 Haidari, Athens, Greece
Correspondence Address:
Dimitrios Varvitsiotis
5, Zosimadon Street, Egaleo 12243, Athens
Greece
 Source of Support: No external source of funding was used in the preparation of this study., Conflict of Interest: None
DOI: 10.4103/0973-6042.137526
 |
|
|
|
| Date of Web Publication | 24-Jul-2014 |
 Abstract Abstract | | |
Purpose: Despite advances in surgical treatment options, large rotator cuff (r-c) tears still represent a challenge for orthopedic surgeons. The purpose of this study was to evaluate the temporary and spatial histological incorporation of fascia lata allografts, used for bridging artificially created defects of the r-c.
Materials and Methods: Seventy-two rabbits were divided into two groups and a supraspinatus tendinous defect was created. Half of the rabbit population underwent repair only, while in the other half, the defect was bridged utilizing fascia lata allograft. The animals were euthanized at 2, 4, and 6 weeks postoperative. Half of the specimens were evaluated histologically and the other half underwent mechanical testing.
Results: There was an increased remodeling activity, fibroblastic in growth and strong presence of collagen fibers observed at 6 weeks on both groups. A gradually increasing mechanical strength was noticed by week 6 and increased toughness was also found at the same time period. There was no significant difference observed between the two groups regarding their histological and mechanical properties.
Conclusions: In the difficult scenario of a large irreparable tear where the simple suture of the remaining r-c is impossible, allograft bridging, could be used with satisfactory results.
Clinical Relevance: Treatment Study, Level 1.
Keywords: Biomechanics, fascia lata allograft patch, graft bridging, histology, massive or irreparable tears of the rotator cuff, rabbit shoulder, rotator cuff repair
How to cite this article:
Varvitsiotis D, Papaspiliopoulos A, Vlachou V, Feroussis J, Papalois A, Papacharalampous X, Soucacos PN, Zoubos A. Fascia lata allograft bridging of a rotator cuff tear in a rabbit animal model. Int J Shoulder Surg 2014;8:39-46 |
How to cite this URL:
Varvitsiotis D, Papaspiliopoulos A, Vlachou V, Feroussis J, Papalois A, Papacharalampous X, Soucacos PN, Zoubos A. Fascia lata allograft bridging of a rotator cuff tear in a rabbit animal model. Int J Shoulder Surg [serial online] 2014 [cited 2016 Aug 23];8:39-46. Available from: http://www.internationalshoulderjournal.org/text.asp?2014/8/2/39/137526 |
| Introduction | |  |
Management of massive irreparable rotator cuff (r-c) tears represent a dilemma to the orthopedic surgeon. [1],[2] Treatment of massive r-c tears have been heavily debatable. [3],[4],[5],[6],[7],[8],[9] It is important to underline that a massive r-c tear is not necessarily an irreparable tear. [10] The predominant classification of a massive tear was described by Cofield and De Orio. [11],[12] The tear is considered massive if it is >5 cm in diameter (≥5 cm). [13],[14] Other authors have described massive cuff tears as those with complete detachment of two or more tendons. [12] Regarding irreparable tears, Rockwood et al. defined them as tears that cannot be repaired primarily to the site of their insertion into the tuberosities, despite conventional techniques of mobilization and soft tissue release. [15] Restoration of this injury is very important due to the extremely uncomfortable symptoms. [16] The prevalence of r-c tears has also estimated to represent a 30% in the general population. [17] After repair surgery there is an increasing number of reported failure rates, that range from 20% to 90%, respectively. [18],[19],[20],[21]
There is a need to establish new repair strategies and new materials that would provide effective mechanical support with inherent biological properties that can influence host cell attachment, proliferation and differentiation, leading to improved rates of healing. [22],[23],[24],[25],[26]
The goal of this study was to test the hypothesis that after implantation of the fascia lata graft, the patch will act as a scaffold for fibroblast growth and subsequent incorporation with histological and biomechanical properties similar to that of the simple suture-repair of the tendon.
| Materials and methods | | |
This study was performed in the Experimental-Research Center ELPEN, as approved by the Institutional Animal Care and Use Committee and supported by the Hellenic Association of Orthopedic Surgery and Traumatology. We used rabbits as an animal model due to the existing anatomical similarities with humans and the similar healing properties of the relevant injuries. [27],[28] Seventy-two male New Zealand white rabbits, with weighing 2.3-3.5 kg were used. The animals were caged individually before and after surgery, and they had free access to standard food and water.
The rabbits were randomly assigned into two groups. Group A included 36 rabbits, where a large r-c defect measuring 6 mm × 4 mm × 1 mm was created on each animal's right forelimb. That was achieved by surgically removing the major part of the supraspinatus tendon at the footprint on its humeral head insertion, followed by direct repair of the tendon to bone (surgical control group). Group B included 36 rabbits that underwent a 6 mm × 4 mm × 1 mm artificial gapping of the supraspinatus tendon identical of that in Group A, but the repair was indirect requiring bridging with a fascia lata patch, harvested from the ipsilateral right hindleg of the rabbits from Group A, as an allograft. These two groups were subdivided into three subgroups. Group A was subdivided into Groups A1, A2, and A3 including 18 rabbits euthanized at 2, 4, and 6 weeks correspondingly, whereas Group B was subdivided in the same way into Groups B1, B2, and B3. Half of the samples of each subgroup after euthanasia were sent to histological analysis and the other half underwent biomechanical testing.
Surgical steps
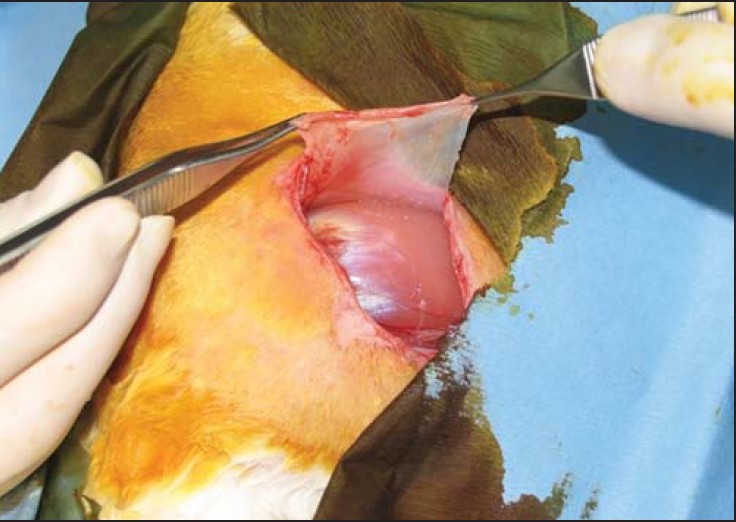
Harvest of the fascia lata and preparation of the patch allograft [Figure 1]
Each animal was anesthetized by intramuscular injection containing a mixture of 15 mg xylazine (rompun 20 mg/mL-bayer) and 50 mg ketamine chlorhydrate (imalgene 10mg/ml-merial). A dose of 150 mg cefamandole (Mandocef-Lilly) was given as chemoprophylaxis. The first step of our surgical procedure was to harvest the fascia lata necessary to augment the artificial gap in Group B [Figure 1]. A 2 cm × 2 cm wide strip of fascia lata was obtained through a 4 cm incision over the lateral aspect of the ipsilateral right hindleg. The next step was manufacturing of the graft in order to produce an isotropic configuration of sufficient mechanical strength and to comprise continuity of the tear tendon as a scaffold. The graft in its final form measured 6 mm × 4 mm × 1 mm after reduplication in seven layers thickness. We stabilized the final form of the patch inserting sutures at each corner of the patch on the free end of the last sheet.
Shoulder's surgical procedure
The first rabbit, from which we harvested the fascia lata, had its ipsilateral right shoulder prepared with simply suturing the artificial defect. The graft was used in Group B rabbit to bridge the gap. The same procedure applied on each couple of rabbits. A longitudinal, anterolateral 3 cm skin incision at the right shoulder was made. A deltoid - splitting approach was utilized. The supraspinatus tendon was identified, and a tendinous defect of 6 mm × 4 mm was made close to the tendon's insertion to the humeral head involving the full-thickness of the tendon (1 mm). In Group A, the tendon was repaired to bone with two nonabsorbable transosseous sutures, after retracting the medial tendinous stump. In Group B, the fascia was sutured to the lateral stump of the supraspinatus tendon with two nonabsorbable sutures and standard knots. The allograft patch was then laid down over the artificial defect and was tensioned so that the lateral end of the fascia was attached on the footprint of the supraspinatus insertion to the humerus and fixated with two nonabsorbable transosseous sutures [Figure 2]. The remaining deltoid (anterior and posterior margin) was sutured side-to-side in order to cover the reconstructed r-c. Following wound irrigation and closure, the rabbit's forelimb was immobilized on its chest by means of a Dessault immobilization.
Postoperative care
Analgesia was achieved through the administration of two doses of 60 mg acetaminophen (Apotel - Uni-Pharma), one at the end of the operation and the second 12 h later. [29] The animals were allowed to move freely within their cages and were evaluated daily during the 1 st postoperative week for appetite, activity, temperature, weight-bearing, local infection, and wound dehiscence.
Euthanasia and sample preparation
The animals were euthanized at 2, 4, and 6 weeks according to their groups as described, using an intracardiac injection of 2.5 ml pentobarbital sodium (dolethal 200 mg/mL - vetoquinol). The supraspinatus muscle repaired tendon construction and the proximal part of the humerus were harvested for analysis. The supraspinatus muscle was detached from the scapula, and the tendon was released from the surrounding tissues and dissected all the way to its insertion to the greater tuberosity. The glenohumeral joint capsule was divided circumferentially to isolate the repaired tendon prior to testing.
Biomechanical characterization
Biomechanical testing was done on 36 specimens. Tensile strength tests were conducted by means of Hounsfield HK20-W (Tinius Olsen, Surrey, England) desktop machine, equipped with a 20 kN load cell at a crosshead speed of 5 mm/min. Tendon cross-section area was evaluated by measuring the diameter of each specimen by means of digital caliper. The fixation of the sample was achieved by stitching both ends onto the clamps. The humerus was sutured on the clamp using a double Ethibon No. 5 suture. The other end (free soft tissue) was sutured on the other clamp with the same suture type using the modified Kessler technique. [30] The suture was fixed up the musculotendinous end of the r-c [Figure 3]. In this way, the tendon was always in line with the loading direction [Figure 4]. Statistical significance between allograft and suture group was determined by means of Student's t-test in Microsoft Excel (Microsoft Excel - Ver. 2011; Microsoft Corporation, Redmond, Wash, USA).
Histological evaluation
The samples were fixed in 10% buffered formalin solution for 24 h. Longitudinal sections of 0.3 and 0.4 cm in thickness were obtained from the site of the repair and put on cassettes following dehydration and embedding in paraffin at 62°C for 120 min. The specimens were sectioned into 5 μm sections, stained with H and E, examined under light and polarized light microscopy, and photos of the most representing area were obtained.
| Results | | |
Of a total 72 rabbits, 71 were examined, because one rabbit of the Group B, subgroup B3 died in 4 weeks, and 36 pieces were sent for mechanical analysis and 35 for histological analysis.
Histological analysis
In subgroup A1 (nonpatch subgroup, euthanasia in 2 weeks), there was noted high fibroblastic reaction around the area of tendon repair with the presence of abundant fibroblasts. Few foreign body granulomas were present directed against foreign substance (suture). In subgroup A2 (nonpatch subgroup, euthanasia at 4 weeks), at the site of the tendon repair, there were reparative changes with the presence of abundant multinucleated giant cells against a foreign substance (suture). Furthermore in the repaired area, histological analysis revealed moderately dense chronic inflammatory infiltrates consisting mainly of lymphocytes and a moderate number of vascular structures. In subgroup A3 (nonpatch subgroup, euthanasia at 6 weeks), isolated fibroblastic reaction was recognized at the repair site with the presence of many fibroblasts, fibrosis, and local inflammatory granulation tissue with mild presence of newly formed capillaries (thin wall vessels, which are part of inflammatory granulation tissue) [Figure 5]. In the same subgroup, advanced healing was seen proved by the presence of focal fibers of collagen, whereas the vascularity was milder than in Group A2. The subgroup B1 (patch subgroup, euthanasia at 2 weeks) revealed the presence of intense fibroblastic reaction along with inflammatory granulation tissue and absorbent granulomas related to a foreign body (suture) and partly to bone. The presence of a moderate to a sufficient number of newly formed capillaries was also evident. In subgroup B2 (patch subgroup, euthanasia at 4 weeks) in the region where the fascia lata was grafted, the main histological observation was consistent fibrosis and chronic inflammatory infiltration accompanied by the presence of lymphocytes and abundant absorbent granulomas. We have also identified fibers of collagen, while the number of newly formed capillaries was small. Finally, in subgroup B3 (patch subgroup, euthanasia at 6 weeks), there was marked fibrosis, fibroblastic reaction with a strong presence of collagen fibers, moderate reparative changes with the presence of granulomas against foreign body and chronic inflammatory infiltration. Of note was the presence of slit spaces filled by fibrin, whereas neovascularization was mild [Figure 6]. | Figure 5: Nonpatch group 6 weeks. Giant cells, inflammatory granulation tissue, fibers of collagen, fibroblasts
Click here to view |
 | Figure 6: Patch group 6 weeks. Bone, collagen fibers, chronic inflammatory infi ltration, slit spaces, filled by fi brin
Click here to view |
Biomechanical analysis
A representative stress - strain curve of a tendon and the three characteristic regions, which appear during the elongation of the collagenous tissues are noted in [Figure 7]. The results of the postoperational biomechanical characterization of the tissues are presented in [Figure 8],[Figure 9] and [Figure 10]. In these graphs, each feature (i.e., modulus, toughness, and strength) is presented as a function of healing time; that is, the time past after the operation. As it can be seen in [Figure 8], the mean tensile strength exhibits increasing trends between the second and the 4 th postoperation week while after the 6 th week, the mean tensile strength increases drastically, in both groups. On the other hand, Young's modulus [Figure 9] exhibits different behavior. In the allograft's group, the modulus increases gradually up to the 6 th week, while on the sutured group, the increasing trend is smaller. Interestingly, no sharp increment of the modulus was noted at the 6 th postoperation week. Finally, the toughness [Figure 10] of the tissues is following similar behavior patterns with the mean tensile strength. That is, an initial increase during the first 2 weeks followed by a stepwise increase at week number six. Interestingly, for a given healing time (i.e., 2-4-6 weeks) the modulus, toughness, and strength of both groups exhibited similar behavior. For example, the 4 weeks postoperational moduli of both allograft-and suture-group show no significant difference (P < 0.05) and as it can be seen in [Figure 8],[Figure 9] and [Figure 10], the same was true for all the other time points and features with P < 0.05. All values measured during our experiments, are now presented in [Table 1].
| Discussion | | |
Irreparable large or massive r-c tears, lead to weakness, chronic pain and severe functional impairment. [21] Tension on the repair site is perhaps the greatest causative factor of eventual failure and poor outcomes. [3],[31] Therefore, McLaughlin emphasized that the goal of operative repair is to reattach the vascularized tissues of the r-c to their original site of insertion without tension [14] and the weak link (the point of the tendon that is the most susceptible to rupture) is the site between tendon and bone. [19],[24] Many procedures have been described for massive irreparable tears including simple arthroscopic debridement. [5],[7],[25],[32] However, new techniques propose bridging the repair with a patch material that theoretically provides immediate stability and acts as a scaffold. Such a scaffold would allow ingrowth of tissue in order to fill in the defect over time and thus improving the biology of the repair healing. [4],[5],[16] There are a few studies regarding augmentation or bridging the r-c defect with varying degrees of success. [31] One of the earlier reports is from Neviaser et al. in which a freeze-dried cadaveric allograft was used to bridge the defect created by a massive tear. [32] The results were poor with 100% failure of the graft on postoperative magnetic resonance imaging. Intense inflammatory reactions in the early postoperative period have been reported using a cross-linked acellular porcine dermal patch in an ovine model. [24] Porcine small intestine submucosa graft was lost owing to early resorption, leading to mechanical weakening and failure, while porcine dermal collagen patch showed mechanical and histological advantages. [4],[6] The graft jacket matrix (regenerative tissue matrix is processed from donated human skin) provides a suitable material to reinforce the primary r-c repair. [26] The polytetrafluoroethylene felt graft is very effective for pain relief, but Kimura et al. have reported resorption of bone at the insertion of the graft. [34] In our study, we used a fascia lata patch because of a number of advantages. First, its surgical use is well-established in reconstructions by ophthalmologists and urogynecologists. It can provide early structural integrity and strength within weeks because of its mechanical, chemical, and ultrastructural similarity to the natural tendon. [23] In addition, the tension at the reconstruction site is reducible, and it does not provoke any immune response. [23],[26] Our initial findings are encouraging, suggesting that our proposal is equivalent to simple suture-repair. Regarding tissue healing and its mechanical properties, it can give us a solution to the difficult problem of irreparable r-c rupture, where the simple suture-repair is impossible. Specifically, as far as histology is concerned, the patch was associated with scaffolding of fibrovascular collagenous tissue and did not elicit an adverse immunogenic response beyond that noted in relation to suture. Collagen fibers and reparative changes suggest an ongoing healing process. The time between surgery and euthanasia was not enough for maturation of the connective tissue produced; nevertheless, a similar time interval is required for healing in humans and the healing level was satisfactory. The collagen fibers, the cellular repopulation and a vascular network offer valuable information regarding graft incorporation, host cellular response and graft functional viability that ultimately will lead to the formation of a tendon-like material. Furthermore, the fibroblastic cells appearing at the healing site and slit spaces filled by fibrin serve as a scaffold with regenerative potential that promotes host tissue ingrowth. [16],[20],[26] Biomechanical analysis shows that the healing process is slower in the allograft group. Of notice are increasing trends of the allograft modulus, which is in sound contrast to sutured ones that reach a plateau after the 4 th postoperating week. This could reflect different healing procedures between the two groups.
In conclusion, both groups show equivalent histological results and mechanical properties and specifically, the tensile strength seems to have equally good results on both groups during the whole period of 6 weeks. However, the allograft appears superior at 6 weeks compared with the simple suture on Young's Modulus and outmatches the simple suture-repair again in the first 4 weeks, in terms of toughness. Finally, this tension-free repair provide less mechanoreceptor stimulation and therefore, potentially less pain and less likelihood of re-tear as Burkhart et al. published. [33]
We acknowledge the potential limitations of our study, namely, the acute tear we describe lacks some of the characteristics of a chronic r-c tear. Our thought was to study the graft's response and to compare it with a simple suture at a higher tension point, in order to test the hypothesis of a satisfactory healing. It is our intension to evaluate chronic tears in a subsequent experiment. In addition, the graft we are using is a fresh allograft, in contrast to the freezed grafts that are available for commercial use that are also found to retain some incorporating properties. [5] Finally, it should be highlighted that this study was conducted on animal subjects with very similar but still different anatomical and histological properties compared to human shoulders. Further animal and clinical studies are needed to elucidate the role of fascia lata graft as a therapeutic option on large r-c defects. [5],[9]
| Conclusion | | |
Based on the results of our study, we believe that this technique provided a tendon to bone bridge for host tissue deposition and ingrowth resulting in improved biomechanical function applied in a similar manner, and that might offer a functional benefit to patients undergoing r-c repair. Therefore, the described procedure provides a potentially new avenue of treatment in this complex and technically challenging group of patients by its minimal host inflammatory response, similar mechanical strength to that of the native tendon and similar strength to that of the simple suture-repair of the tendon.
| Acknowledgments | | |
We would like to express our thanks to the Hellenic Association of Orthopedic Surgery and Traumatology that fostered this experimental work and provided valuable support by means of secretarial assistance and manpower. We are grateful to Dr. O.L. Katsamenis of the Materials Science Department at the University of Patras, Hellas, for his valuable contribution in the biomechanical characterization.
| References | | |
| 1. | Adams JE, Zobitz ME, Reach JS Jr, An KN, Steinmann SP. Rotator cuff repair using an acellular dermal matrix graft: An in vivo study in a canine model. Arthroscopy 2006;22:700-9. 
|
| 2. | Audenaert E, Van Nuffel J, Schepens A, Verhelst M, Verdonk R. Reconstruction of massive rotator cuff lesions with a synthetic interposition graft: A prospective study of 41 patients. Knee Surg Sports Traumatol Arthrosc 2006;14:360-4.
|
| 3. | Sclamberg SG, Tibone JE, Itamura JM, Kasraeian S. Six-month magnetic resonance imaging follow-up of large and massive rotator cuff repairs reinforced with porcine small intestinal submucosa. J Shoulder Elbow Surg 2004;13:538-41.
|
| 4. | Badhe SP, Lawrence TM, Smith FD, Lunn PG. An assessment of porcine dermal xenograft as an augmentation graft in the treatment of extensive rotator cuff tears. J Shoulder Elbow Surg 2008;17 1 Suppl:35S-9.
|
| 5. | Derwin KA, Badylak SF, Steinmann SP, Iannotti JP. Extracellular matrix scaffold devices for rotator cuff repair. J Shoulder Elbow Surg 2010;19:467-76.
|
| 6. | Derwin KA, Codsi MJ, Milks RA, Baker AR, McCarron JA, Iannotti JP. Rotator cuff repair augmentation in a canine model with use of a woven poly-L-lactide device. J Bone Joint Surg Am 2009;91:1159-71.
|
| 7. | Domb BG, Glousman RE, Brooks A, Hansen M, Lee TQ, ElAttrache NS. High-tension double-row footprint repair compared with reduced-tension single-row repair for massive rotator cuff tears. J Bone Joint Surg Am 2008;90 Suppl 4:35-9.
|
| 8. | Sano H, Kumagai J, Sawai T. Experimental fascial autografting for the supraspinatus tendon defect: Remodeling process of the grafted fascia and the insertion into bone. J Shoulder Elbow Surg 2002;11:166-73.
|
| 9. | Zalavras CG, Gardocki R, Huang E, Stevanovic M, Hedman T, Tibone J. Reconstruction of large rotator cuff tendon defects with porcine small intestinal submucosa in an animal model. J Shoulder Elbow Surg 2006;15:224-31.
|
| 10. | Bedi A, Dines J, Warren RF, Dines DM. Massive tears of the rotator cuff. J Bone Joint Surg Am 2010;92:1894-908.
|
| 11. | Cofield, RH, Current concepts review. Rotator cuff disease of the shoulder. J. Bone and Joint Surg 67-A: 974-979, July 1985.
|
| 12. | DeOrio JK, Cofield RH. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
|
| 13. | Hansen ML, Otis JC, Johnson JS, Cordasco FA, Craig EV, Warren RF. Biomechanics of massive rotator cuff tears: Implications for treatment. J Bone Joint Surg Am 2008;90:316-25.
|
| 14. | Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr. Débridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-66.
|
| 15. | Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr. Débridement of degenerative irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-66.
|
| 16. | Iannotti JP, Codsi MJ, Kwon YW, Derwin K, Ciccone J, Brems JJ. Porcine small intestine submucosa augmentation of surgical repair of chronic two-tendon rotator cuff tears. A randomized, controlled trial. J Bone Joint Surg Am 2006;88:1238-44.
|
| 17. | Derwin KA, Baker AR, Codsi MJ, Iannotti JP. Assessment of the canine model of rotator cuff injury and repair. J Shoulder Elbow Surg 2007;16 5 Suppl:S140-8.
|
| 18. | Dejardin LM, Arnoczky SP, Ewers BJ, Haut RC, Clarke RB. Tissue-engineered rotator cuff tendon using porcine small intestine submucosa. Histologic and mechanical evaluation in dogs. Am J Sports Med 2001;29:175-84.
|
| 19. | MacGillivray JD, Fealy S, Terry MA, Koh JL, Nixon AJ, Warren RF. Biomechanical evaluation of a rotator cuff defect model augmented with a bioresorbable scaffold in goats. J Shoulder Elbow Surg 2006;15:639-44.
|
| 20. | Schlegel TF, Hawkins RJ, Lewis CW, Motta T, Turner AS. The effects of augmentation with Swine small intestine submucosa on tendon healing under tension: Histologic and mechanical evaluations in sheep. Am J Sports Med 2006;34:275-80.
|
| 21. | Sener M, Altay MA, Baki C, Turhan AU, Cobanoglu U. The comparison of patellar tendon-bone autografting and free flexor-tendon autografting in infraspinatus defect of the shoulder: Biomechanical and histological evaluation in a sheep model. Knee Surg Sports Traumatol Arthrosc 2004;12:235-40.
|
| 22. | Barber FA, Aziz-Jacobo J. Biomechanical testing of commercially available soft-tissue augmentation materials. Arthroscopy 2009;25:1233-9.
|
| 23. | Derwin KA, Aurora A, Iannotti JP. Allograft fascia lata as an augmentation device for musculoskeletal repairs. Conference Paper. Cleveland Clinic, Cleveland, OH. Google-Article; Dec 2008.
|
| 24. | Nicholson GP, Breur GJ, VanGalatz LM, Connor PM, Calfee RP, Hsu JC, Yamaguchi K. Pectoralis major transfer for anterior-superior subluxation in massive rotator cuff insufficiency. J Shoulder Elbow Surg 2003;12 5 Suppl:1-5.
|
| 25. | Galatz LM, Connor PM, Calfee RP, Hsu JC, Yamaguchi K. Pectoralis major transfer for anterior-superior subluxation in massive rotator cuff insufficiency. J Shoulder Elbow Surg 2003;12:1-5.
|
| 26. | Snyder SJ, Arnoczky SP, Bond JL, Dopirak R. Histologic evaluation of a biopsy specimen obtained 3 months after rotator cuff augmentation with GraftJacket Matrix. Arthroscopy 2009;25:329-33.
|
| 27. | Grumet RC, Hadley S, Diltz MV, Lee TQ, Gupta R. Development of a new model for rotator cuff pathology: The rabbit subscapularis muscle. Acta Orthop 2009;80:97-103.
|
| 28. | Gupta R, Lee TQ. Contributions of the different rabbit models to our understanding of rotator cuff pathology. J Shoulder Elbow Surg 2007;16:S149-57.
|
| 29. | Papaspiliopoulos A, Papaparaskeva K, Papadopoulou E, Feroussis J, Papalois A, Zoubos A. The effect of local use of nandrolone decanoate on rotator cuff repair in rabbits. J Invest Surg 2010;23:204-7.
|
| 30. | Barmakian JT, Lin H, Green SM, Posner MA, Casar RS. Comparison of a suture technique with the modified Kessler method: Resistance to gap formation. J Hand Surg Am 1994;19:777-81.
|
| 31. | Davidson PA, Rivenburgh DW. Rotator cuff repair tension as a determinant of functional outcome. J Shoulder Elbow Surg 2000;9:502-6.
|
| 32. | Burkhart SS. Arthroscopic treatment of massive rotator cuff tears. Clinical results and biomechanical rationale. Clin Orthop. 1991;267:45-56.
|
| 33. | Neviaser JS. Ruptures of the rotator cuff of the shoulder. New concepts in the diagnosis and operative treatment of chronic ruptures. Arch Surg 1971;102:483-5.
|
| 34. | Kimura A, Aoki M, Fukushima S, Ishii S, Yamakoshi K. Reconstruction of a defect of the rotator cuff with polytetrafluoroethylene felt graft. Recovery of tensile strength and histocompatibility in an animal model. J Bone Joint Surg Br 2003;85:282-7.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10]
[Table 1]
|