| |


 |
| Year : 2014 | Volume
: 8
| Issue : 2 | Page : 55-57 |
|
|
|
|
|
CASE REPORT Osteochondral humeral head fracture after posterior shoulder subluxation: A case report
Emmanouil Fandridis, Spiros Stavropoulos, Leonidas Dimou, Sarantis Spyridonos
Department of Hand Surgery-Upper Limb-Microsurgery, KAT General Hospital and Trauma Centre, Athens, Greece
Correspondence Address:
Emmanouil Fandridis
Gravias 126, Argiroupolis 16451, Athens
Greece
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.137529
 |
|
|
|
| Date of Web Publication | 24-Jul-2014 |
 Abstract Abstract | | |
Traumatic posterior shoulder subluxations are rare entities which require clinical suspicion upon presentation. Although literature presents many sequels of posterior shoulder subluxations, we have not come across any shearing type osteochondral fracture in the literature. In this case report we present diagnosis, treatment and follow-up results of this rare fracture in a 26-year-old male following a fall from a motorcycle.
Keywords: Dislocation, humeral head, osteochondral, posterior, shoulder
How to cite this article:
Fandridis E, Stavropoulos S, Dimou L, Spyridonos S. Osteochondral humeral head fracture after posterior shoulder subluxation: A case report. Int J Shoulder Surg 2014;8:55-7 |
| Introduction | |  |
This case refers to a shearing type osteochondral humeral head fracture following a traumatic posterior shoulder subluxation. The spectrum of the pathoanatomical findings after posterior shoulder subluxations or dislocations have already been described in the literature. [1],[2],[3],[4] This is the first reported case to our knowledge where an osteochondral fracture is associated with posterior labral lesion after a traumatic posterior subluxation. This important case presents a trauma of the shoulder which has potential to be misdiagnosed.
Posterior glenohumeral dislocations represent only 2% of all shoulder dislocations, and their initial diagnosis is missed in more than 60% of cases. [3] Posterior shoulder dislocations result from axial loading of the adducted and internally rotated shoulder, violent muscle contractions resulting from seizers or electrocution, or a direct posterior force applied to the anterior shoulder. [3]
| Case report | | |
A 26-year-old male patient was referred to our hospital presenting with a traumatic posterior subluxation on his left shoulder. He reported a motor-vehicular accident in which he fell from a motorcycle. The patient reported that he sustained a direct impact injury on his left shoulder in which he felt severe shoulder pain and a "popping" sensation.
After clinical and radiological work-up he was diagnosed with an osteochondral shearing type fracture of the humeral head [Figure 1]. The patient suffered no other injuries. Also, the patient reported no history of shoulder dislocation or subluxation or any other chronic or acute diseases. The patient was also not on any medication.  | Figure 1: Preoperative anteroposterior X-ray of the shoulder showing the osteochondral fracture in the axillary pouch
Click here to view |
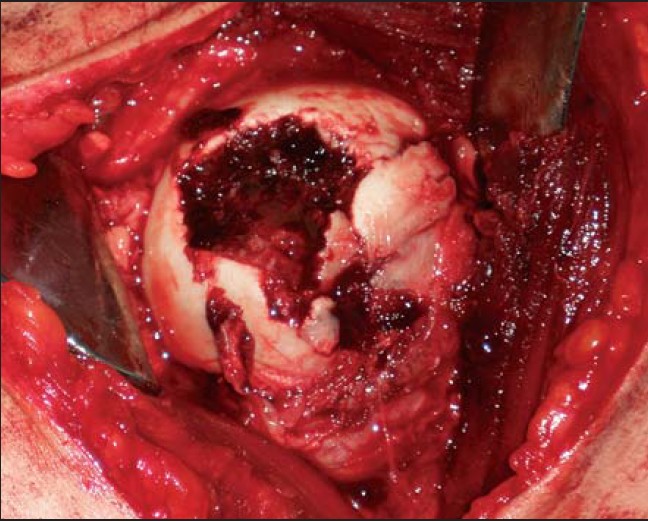
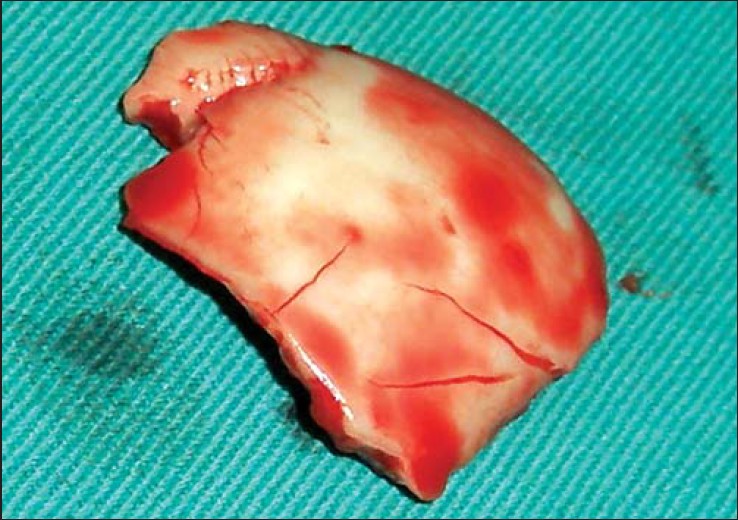
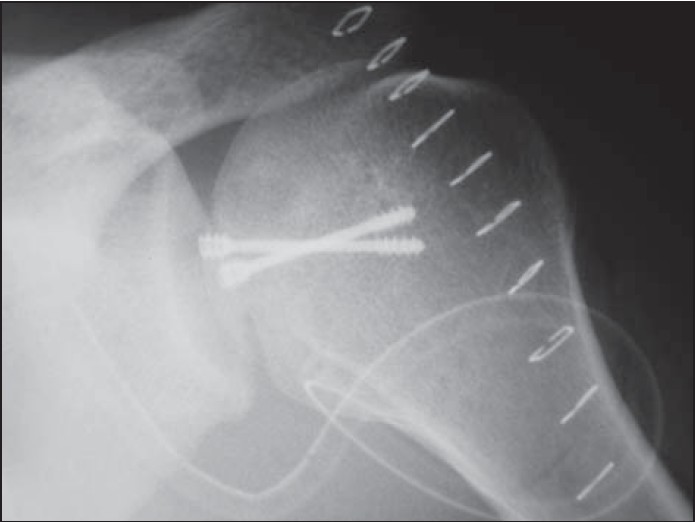
The patient was managed operatively under general anesthesia in a beach chair position. The delto-pectoral approach was performed with maximum deltoid muscle preservation and tenotomy of the upper third of the subscapularis. With the arm in abduction and external rotation the osteochondral defect was evident at the antero-medial aspect of the humeral head [Figure 2]. The osteochondral fragment missing from the humeral head was "fished out" of the posterior-inferior axillary pouch [Figure 3]. Its size was 3.5 cm × 4 cm. Following inspection of the glenohumeral joint, a posterior SLAP (Superior Labral Anteroposterior) type II lesion with a posterior extension till the 1.00 o'clock position was found. Posterior labrocapsular detachment was also found at the 8.00 o'clock position. The osteochondral fragment was anatomically reduced using two k-wires and finally fixed in place with two headless 16 mm screws (Herbert, Wemmel, Belgium). The screws were counter-sinked approximately 1 mm [Figure 4]. Final radiograph is shown in [Figure 5]. The SLAP lesion and the posterior labral capsular detachment were repaired with two absorbable suture-anchors (Panalock, DePuy Mitek, Inc., a Johnson & Johnson Co, MA). The subscapularis tendon was anatomically repaired with non-absorbable ultra-braided sutures (Orthocord, DePuy Mitek, Inc., a Johnson & Johnson Co, MA). The patient was fitted with a 15° abduction sling with the arm in neutral rotation for 5 weeks. The patient was discharged 2 days postoperatively. The immediate postoperative period was free of complications. One year postoperatively the patients' range of motion was comparable to the non-affected shoulder. However, the patient has not returned to his pre-injury activities. The radiological work-up showed full fragment integration, without any absorption or necrosis. 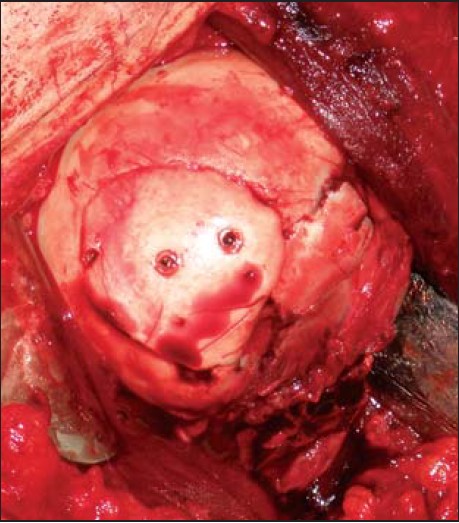 | Figure 4: Anatomical provisional reduction of osteochondral fragment with k-wires and final with Herbert screws
Click here to view |
| Discussion | | |
A traumatic posterior subluxation or dislocation are relatively rare injuries and account for approximately 2% of all shoulder dislocations. [4] In the literature, lesions commonly associated with traumatic posterior subluxation/dislocation are the reverse Hill-Sachs (or McLaughlin Lesion [4] ), a posterior labral detachment, glenohumeral ligament lesions, [2] rotator cuff tears or posterior bony fractures. [3] After such an accident and type of blunt force trauma on the shoulder we would expect to see a reverse Hill-Sachs lesion, an impression fracture on the anteromedial humeral articular surface as first described by McLaughlin. [4] This is the first case to our knowledge in which a shearing type osteochondral fracture was observed in a traumatic posterior subluxation. The intraoperative pathoanatomic findings of the posterior labrocapsular detachment, the anteromedial aspect of the fracture of the humeral head, the patient's description with the direct impact of the shoulder toward posterior direction and the sensation of his shoulder 'popping" enforces our diagnosis for the posterior shoulder subluxation.
Yun Sun Choi et al. (2005) reported a shearing osteochondral fracture of the humeral head in a 12-year-old right-handed-dominant boy injured while playing football following an anterior dislocation. [5] The fracture was diagnosed by plain radiographs and MRI. This patient was treated conservatively with good results.
| Conclusion | | |
To the best of our knowledge, our patient represents the first reported case of an osteochondral shearing fracture of the humeral head. This fracture resulted from a traumatic posterior subluxation of the shoulder. Because imaging techniques may be unreliable in such fractures, one must be aware of their existence.
| References | | |
| 1. | Abrams JS. Arthroscopic repair of posterior instability and reverse humeral glenohumeral ligament avulsion lesions. Orthop Clin North Am 2003;34:475-83. 
|
| 2. | Ames JB, Millett PJ. Combined posterior osseous Bankart lesion and posterior humeral avulsion of the glenohumeral ligaments: A case report and pathoanatomic subtyping of "floating" posterior inferior glenohumeral ligament lesions. J Bone Joint Surg Am 2011;93:e118(1)-(4).
|
| 3. | Rouleau DM, Hebert-Davies J. Incidence of associated injury in posterior shoulder dislocation: Systematic review of the literature. J Orthop Trauma 2012;26:246-51.
|
| 4. | McLaughlin HL. Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;24-A-3:584-90.
|
| 5. | Choi YS, Potter HG, Scher DM. A shearing osteochondral fracture of the humeral head following an anterior shoulder dislocation in a child. HSS J 2005;1:100-2.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|