| |


 |
| Year : 2016 | Volume
: 10
| Issue : 1 | Page : 15-20 |
|
|
|
|
|
ORIGINAL ARTICLE Biomechanical evaluation of the Nice knot
Shannon W Hill1, Christopher R Chapman2, Samer Adeeb3, Kajsa Duke1, Lauren Beaupre2, Martin J Bouliane2
1 Department of Mechanical Engineering, University of Alberta, Edmonton, Alberta, Canada
2 Division of Orthopaedic Surgery, University of Alberta, Edmonton, Alberta, Canada
3 Department of Civil and Environmental Engineering, University of Alberta, Edmonton, Alberta, Canada
Correspondence Address:
Samer Adeeb
Department of Civil and Environmental Engineering, University of Alberta, 3-025 NREF, Edmonton, Alberta T6G 2W2
Canada
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/0973-6042.174513
 |
|
|
|
| Date of Web Publication | 20-Jan-2016 |
 Abstract Abstract | | |
Background: The Nice knot is a bulky double-stranded knot. Biomechanical data supporting its use as well as the number of half hitches required to ensure knot security is lacking.
Materials and Methods: Nice knots with, one, two, or three half-hitches were compared with the surgeon's and Tennessee slider knots with three half hitches. Each knot was tied 10 times around a fixed diameter using four different sutures: FiberWire (Arthrex, Naples, FL), Ultrabraid (Smith and Nephew, Andover, MA), Hi-Fi (ConMed Linvatec, Largo, FL) and Force Fiber (Teleflex Medical OEM, Gurnee, IL). Cyclic testing was performed for 10 min between 10N and 45N, resulting in approximately 1000 cycles. Displacement from an initial 10N load was recorded. Knots surviving cyclic testing were subjected to a load to failure test at a rate of 60 mm/min. Load at clinical failure: 3 mm slippage or opening of the suture loop was recorded. Bulk, mode of ultimate failure, opening of the loop past clinical failure, was also recorded.
Results: During cyclic testing, the Nice knots with one or more half-hitches performed the best, slipping significantly less than the surgeon's and Tennessee Slider (P < 0.002). After one half-hitch, the addition of half-hitches did not significantly improve Nice knot performance during cyclic testing (P > 0.06). The addition of half-hitches improved the strength of the Nice knot during the force to failure test, however after two half-hitches, increase of strength was not significant (P = 0.59). While FiberWire was the most bulky of the sutures tested, it also performed the best, slipping the least.
Conclusion: The Nice knot, especially using FiberWire, is biomechanically superior to the surgeon's and Tennessee slider knots. Two half hitches are recommended to ensure adequate knot security.
The level of Evidence: 2, prospective comparative study.
Keywords: Biomechanics, cyclic loading, half-hitches, knot security, load to failure, Nice knot
How to cite this article:
Hill SW, Chapman CR, Adeeb S, Duke K, Beaupre L, Bouliane MJ. Biomechanical evaluation of the Nice knot. Int J Shoulder Surg 2016;10:15-20 |
| Introduction | |  |
The Nice knot is a double stranded knot that has been recently proposed for tuberosity osteosynthesis in the management of proximal humerus fractures. Arthroscopic transosseous rotator cuff repair is also proposed as a novel application of the Nice knot. Biomechanical data supporting the use of the Nice knot in either open or arthroscopic applications, however, is lacking.
Numerous studies have been performed that test the properties of commonly used knots. Since the suture material used can affect the knot's properties, studies have often tested knots using more than one material to assess knot performance characteristics. [1],[2],[3] Knot security is one performance characteristic, defined as a knot's resistance to monotonic loading or cyclic loading. [4] Previously, cyclic testing followed by a load to failure test has been performed to assess a knot's security. [2],[3],[5],[6] Knot security is required to ensure a suture construct will not fail. Half-hitches can provide additional knot security to a construct, but will increase the bulk of the knot with the addition of more suture material. Determining the minimum number of half-hitches required to produce sufficient knot security and strength will reduce bulk and foreign material.
The surgeon's knot is the standard knot used in open surgical approaches while the Tennessee slider is an arthroscopic knot that has performed well in previous studies. [1] While the surgeon's and Tennessee slider knot are single stranded knots, the Nice knot is double stranded.
The purpose of this study is to compare the Nice knot with one, two and three half-hitches to the Tennessee slider and surgeon's knots, using four different suture materials. It was hypothesized that the Nice knot with three half-hitches would have superior knot security and strength when compared with the Tennessee slider or surgeon's knots.
| Materials and methods | | |
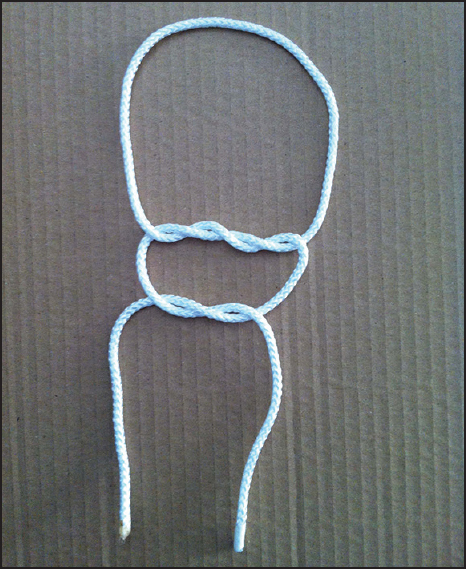
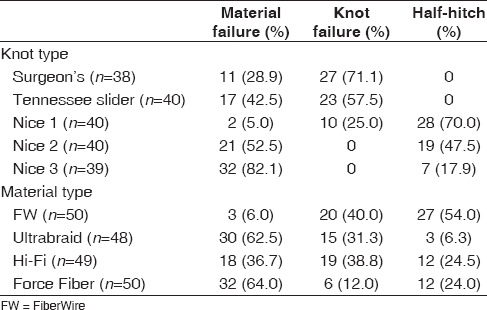
Five different knots were tested using four different suture materials. The knots consisted of: Surgeon's knot with four alternating half-hitches; Tennessee Slider with three alternating posthalf-hitches, and three variations of the Nice knot. The knots used in this study were selected based upon performance characteristics as determined by the previous investigation. [1],[2],[4],[7] Although the knots are of differing types; the surgeon's knot is nonsliding, and the Tennessee slider and Nice knot are sliding nonlocking knots, this should not affect testing or results. All knots tested were completed and locked with alternating half hitches prior to loading, thus all knots tested were "locked" at the time of testing. The Nice knots were tied with one, two, and three alternating posthalf-hitches, designated as: Nice 1, Nice 2, and Nice 3 respectively. The two single strand knots, the surgeon's and Tennessee slider knots, and the double stranded Nice knot are shown in [Figure 1] [Figure 2] [Figure 3]. These knots were tied using FiberWire (Arthrex, Naples, FL), Ultrabraid (Smith and Nephew, Andover, MA), Hi-Fi (ConMed Linvatec, Largo, FL) and Force Fiber (Teleflex Medical OEM, Gurnee, IL). A surgical resident (critical care) tied all five-knot types around a fixed diameter 10 times each for each of the four materials, for a total of 200 knots. [1],[2],[7],[8] The knots were not tied in order of suture type or knot type - two knots of the same type were not tied using the same material in a row. There was a short training period with a fellowship certified surgeon to ensure that the knots were tied correctly. Two Ultrabraid surgeon's knots and one Hi-Fi Nice knot with three half-hitches were compromised during testing, resulting in 197 knots included in the analysis.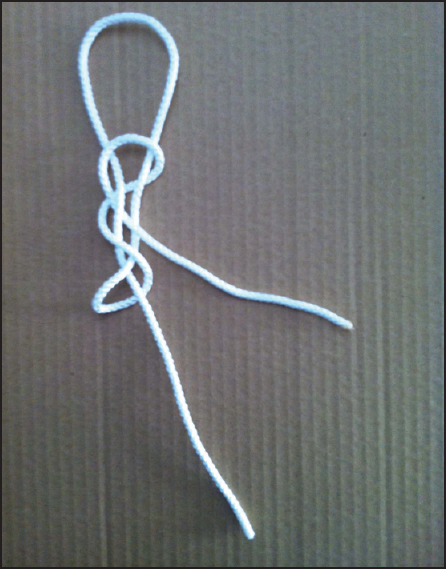 | Figure 2: The Tennessee Slider knot is commonly used in arthroscopic applications and has performed well in previous studies
Click here to view |
 | Figure 3: The Nice knot is a double-stranded knot, which increases bulk. It was tested with 0, 1, 2, and 3 half-hitches. Shown without half-hitches
Click here to view |
Knots were mounted on a 4443 Instron machine and first subjected to cyclic testing. The machine cycled between 10N and 45N for 10 min at approximately 1.8 Hz, resulting in approximately 1000 cycles. [1],[2] After cycling, the knot was pulled to failure at a rate of 60 mm/min. [5] The rates and loads selected are reported as being comparable to normal physiological loads and speeds occurring in daily life. [1],[9]
Data were recorded by the knot and by material type. The amount of slippage, in millimeters that occurred during cyclic testing was recorded from a 10N reference load at the beginning and end of the test. The load at clinical failure was recorded from the load to failure test with clinical failure being defined as opening of the suture loop or 3 mm displacement from 10N initial load. [1],[5],[6] This increase in loop diameter is accepted in previous studies as being a clinical failure. However it is unknown specifically how much of an increase in diameter will be clinically relevant. The mode of absolute failure, when the loop opened, was also recorded. [2],[3],[6] Breakage of the suture material in any location, within or outside of the knot, was recorded as material failure rather than knot failure. If the loop opened due to knot unraveling, this was defined as knot failure.
Three instances of each knot per suture material were weighed to determine bulk. [7],[8] The suture material was cut as close to the knot base as possible to ensure only material used in the knot was weighed. Bulk was used as an analog to volume, on the principle that more of a given suture material used in a knot construct would translate into a larger volume. This could be compared between suture materials and knots within our study.
Data were first analyzed by grouping all the knot types and then the material types together. Independent two-tailed t-tests were performed on the data with P < 0.05 set as the level of significance. A surface design using Statistica (StatSoft, Inc., www.statsoft.com) determined if there was a significant interaction between the knot type and material tested.
| Results | | |
Cyclic testing
The average displacement experienced by the loop constructs through cyclic testing was recorded [Table 1]. The Nice knots slipped significantly less than the surgeon's and Tennessee slider knot (P < 0.002). The addition of half hitches did improve the performance of the Nice knot though not significantly (P > 0.06). The interaction between knot and material was significant (P = 0.006). A contour plot [Figure 4] shows that the least cyclic displacement is found with the Nice 2 or Nice 3 knot with the FiberWire material. The combination of the surgeon's knot with Ultrabraid performed the worst as these constructs experienced >3 mm displacement prior to the load to failure tests.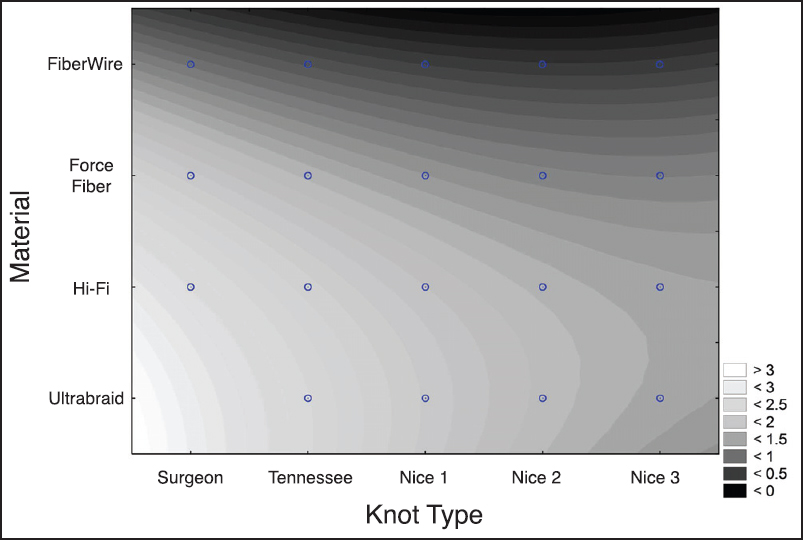 | Figure 4: Contour plot of cyclic displacement (mm). The knot type is listed on the horizontal axis while the suture material is on the vertical axis. The least amount of displacement is shown in white
Click here to view |
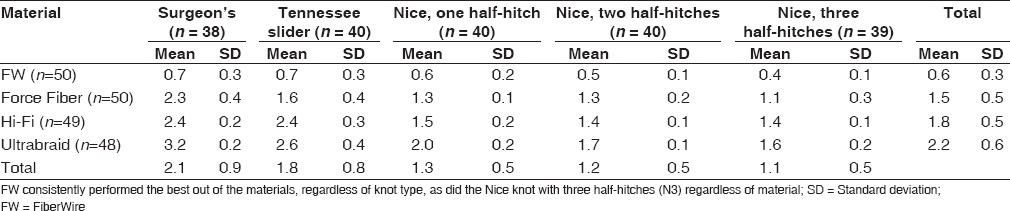 | Table 1: Displacement (mm) experienced during cyclic testing by knot and material type
Click here to view |
Each material performed significantly differently during cyclic testing, with FiberWire slipping the least. Ten out of 58 (17.2%) Ultrabraid knots experienced a clinical failure during cyclic testing. Of these knots, eight were Surgeon's knots, and two were Tennessee slider knots.
Load at clinical failure
Knots surviving cyclic testing (n = 187) were subjected to a load to failure test [Table 2]. The Nice knots were significantly stronger than the surgeon's and Tennessee slider knot (P < 0.04). The addition of half hitches increased the load at failure for the Nice knots. Nice 2 and Nice 3 knots were significantly stronger than Nice 1 (P < 0.04). The interaction between knot and material was again significant (P < 0.000001). A contour plot [Figure 5] shows that the strongest knot is the Nice 3 knot tied with FiberWire.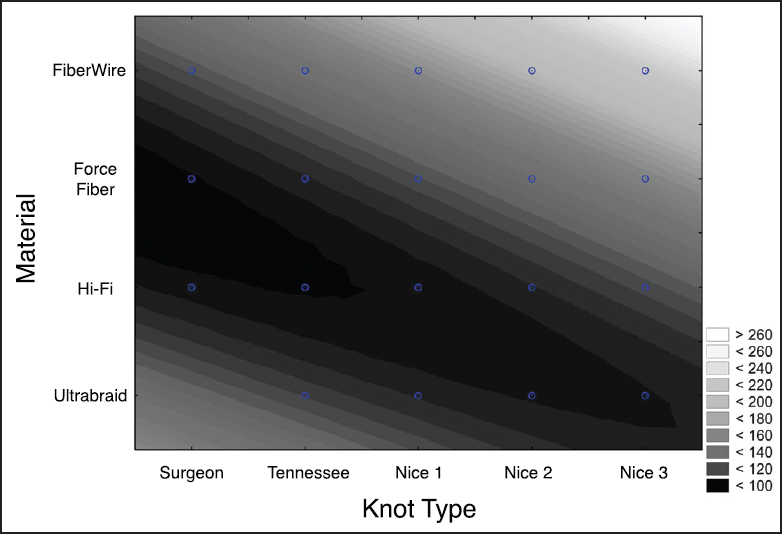 | Figure 5: Contour plot of load at clinical failure (N). The knot type is listed on the horizontal axis while the suture material is on the vertical axis. The strongest failure load is shown in white
Click here to view |
Mode of absolute failure
The Nice 2 and Nice 3 knots were the only knots to experience material failure as the main mode of absolute failure [Table 3]. Out of 119 Nice knots, 54 (45%) had the half-hitch(es) pulled through the loop of the Nice knot as a means of absolute failure. As the number of half hitches increases the occurrence of the half-hitch(es) being pulled through the loop decreased, as did the occurrence of knot failure.
FiberWire and Hi-Fi experienced more knot failure than material failure as the absolute failure mode [Table 3].
Knot bulk
The Nice 3 knot weighed significantly more than any of the other knots tested (P < 0.04) [Table 4]. Although the Nice 2 knot weighed more than the Tennessee slider knot and the Nice 1 knot, the difference was not significant (P > 0.1). FiberWire significantly outweighed any other material (P < 4×10−8 ).
| Discussion | | |
This study confirms that the Nice knot has desirable biomechanical properties making it acceptable for clinical use. We identified that the Nice knot with two or three half-hitches using FiberWire was the most favorable in terms of knot security and strength.
In terms of knot security, the Nice knot with only one half hitch slipped significantly less than the Tennessee slider, and surgeon's knots. Additional half hitches did improve knot security but only trended toward significance (P = 0.06). The least slippage occurred using FiberWire. Similarly, the Nice knot with at least two half hitches was the strongest of knots tested, again with FiberWire performing the best of the sutures tested. Kim et al. in previous work demonstrated that while additional half hitches improved strength and security of a knot, there was a point where this effect plateaued. [6] In contrast to knot security where all materials performed significantly differently from each other, three of the four materials performed similarly in the load to failure test. Only FiberWire performed differently and was significantly stronger than the other three materials. Barber et al. examined load to failure strength of various knots with several suture materials and also found that FiberWire was significantly stronger than Force Fiber, Ultrabraid, and Hi-Fi. [1] As with Barber et al., the present study found that FiberWire's strength varied more than other material. Kim et al. found the addition of half-hitches caused the higher occurrence of a material failure as opposed to knot failure. [6] The Nice knot with two and three half-hitches was the only knots to experience material failure as the primary mode of ultimate failure, indicating the knot is not the weak link in the overall construct. The occurrence of material failure increased as the number of half hitches on the Nice knot increased.
The surface analysis showed that interaction between the knots and material used is also significant. This was an unexpected finding. However, it is unknown how much displacement is clinically acceptable. As seen in [Figure 4], to achieve an average displacement of <1.5 mm, any knot tied using FiberWire or the Nice knot with two or three half hitches using Hi-Fi or Force Fiber could be employed. The interaction of knot and material type had a significant effect on failure strength. [Figure 5] shows that the most desirable region is in the top right corner (Nice 3 knot in combination with FiberWire). Again a suitable combination can be found depending on the desired average failure load. Recently published literature regarding abrasion wear of polybraid sutures demonstrates that there is an effect of material and knot interaction. [1] All materials used were comprised of an ultrahigh molecular weight polyethylene braid (UHMWPE) except FiberWire, which has a polyester braid surrounding a UHMWPE core. [10] It was determined that this had a definite effect on breakage within a construct, with a UHMWPE core conveying a greater resistance to abrasion - however all polybraid sutures demonstrated poor abrasion resistance. [10] This could be relevant to the outcomes of our investigations given the different knots tied will have a different number of bends required in the suture and so will wear differently. [10] In addition, in vivo this will likely have an effect secondary to the physiological response to wear debris. [10] Within this study, no other specific interactions between knot-type and material type were examined. The authors of this study feel that these areas require further investigation, in agreement with recently published literature.
To our knowledge, there has yet to be a biomechanical evaluation of the Nice knot determining its clinical suitability. Proposed by Boileau and Rumian for tuberosity synthesis in proximal humerus fractures, [11] it has also been used by the senior author (MB) for transosseous arthroscopic rotator cuff repair. Being very easy to tie as well as a sliding knot, it is ideally suited for arthroscopic applications. However, a bulky, nonabsorbable knot is theoretically not ideal for arthroscopic rotator cuff repair. This can lead to ongoing mechanical symptoms and pain secondary to large knots in the subacromial and/or subdeltoid space, especially if the knot is tied directly on top of the rotator cuff. To avoid this, the surgeon should make every attempt to keep the knot on the lateral part of the proximal humerus as opposed to on the surface of the cuff itself. Having the strongest, most secure, yet least bulky knot is ideal. The Nice knot using FiberWire with three half hitches was significantly bulkier than the other knots tested. However with only two half hitches, the Nice knot demonstrated similar bulk to the Tennessee slider and surgeon's knots.
This study does have some limitations. The knots tied for the study were tied under very different conditions than knots tied during surgery given the practicality and expense of replicating an in vivo environment - the authors are unable to comment on the effect this may have on knot characteristics given the focus of this study on comparison of performance characteristics of knot constructs rather than clinical performance of the knot constructs. The material was exposed to a very different environment in its clinical application than its experimental testing. The suture material was tested in a nonaqueous environment, anchored to smooth metal rather than in clinical application where knots are exposed to very different conditions for prolonged periods of time and anchored to tendon and bone. [1] Further, not all materials available on the market were tested, and these results may not be transferable to all materials. Finally, the mass of suture material required to tie the knots was used to determine knot bulk, as opposed to volume of the knot, thus introducing bias in favor of less dense materials.
| Conclusion | | |
The Nice knot with two half-hitches demonstrates suitable biomechanical characteristics for clinical and arthroscopic use. FiberWire is the most secure and strongest suture of the materials tested. We found significant interactions between knot and materials. In combination, the Nice knot with two half-hitches with FiberWire approaches twice the knot security and strength of the other knots.
Financial support and sponsorship
This study was partially supported by funding from NSERC.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Barber FA, Herbert MA, Beavis RC. Cyclic load and failure behavior of arthroscopic knots and high strength sutures. Arthroscopy 2009;25:192-9.  |
| 2. | Mahar AT, Moezzi DM, Serra-Hsu F, Pedowitz RA. Comparison and performance characteristics of 3 different knots when tied with 2 suture materials used for shoulder arthroscopy. Arthroscopy 2006;22:614.e1-2. |
| 3. | Mahar A, Odell T, Thomas W, Pedowitz R. A biomechanical analysis of a novel arthroscopic suture method compared to standard suture knots and materials for rotator cuff repair. Arthroscopy 2007;23:1162-6. |
| 4. | Elkousy HA, Sekiya JK, Stabile KJ, McMahon PJ. A biomechanical comparison of arthroscopic sliding and sliding-locking knots. Arthroscopy 2005;21:204-10. |
| 5. | Ilahi OA, Younas SA, Alexander J, Noble PC. Cyclic testing of arthroscopic knot security. Arthroscopy 2004;20:62-8. |
| 6. | Kim SH, Yoo JC, Wang JH, Choi KW, Bae TS, Lee CY. Arthroscopic sliding knot: How many additional half-hitches are really needed? Arthroscopy 2005;21:405-11. |
| 7. | Hassinger SM, Wongworawat MD, Hechanova JW. Biomechanical characteristics of 10 arthroscopic knots. Arthroscopy 2006;22: 827-32. |
| 8. | Dahl KA, Patton DJ, Dai Q, Wongworawat MD. Biomechanical characteristics of 9 arthroscopic knots. Arthroscopy 2010; 26:813-8. |
| 9. | Burkhart SS, Johnson TC, Wirth MA, Athanasiou KA. Cyclic loading of transosseous rotator cuff repairs: Tension overload as a possible cause of failure. Arthroscopy 1997;13:172-6. |
| 10. | Savage E, Hurren CJ, Slader S, Khan LA, Sutti A, Page RS. Bending and abrasion fatigue of common suture materials used in arthroscopic and open orthopedic surgery. J Orthop Res 2013;31:132-8. |
| 11. | Boileau P, Rumian A. The doubled-suture Nice knot: A non-slipping and secure fixation of bone fragments and soft tissues usable in open and arthroscopic surgery. In: Boileau P, editor. Shoulder Concepts 2010: Arthroscopy and Arthroplasty. Montpellier: Sauramps Medical; 2010. p. 245-50. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
[Table 1], [Table 2], [Table 3], [Table 4]
|