|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 1
| Issue : 3 | Page : 63-66 |
|
X syndrome prevalence among infertile women need reproductive technology In vitro fertilisation and intracytoplasmic sperm injection
Maryam Kianpour1, Mina Fazlollahi Mohammadi2, Ashraf Kazami1, Seyed Mehdi Ahmadi3
1 Department of Midwifery, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran
2 Department of Health Education and Health Promotion, School of Health, Isfahan University of Medical Sciences, Isfahan, Iran
3 Isfahan Fertility and Infertility Center, Isfahan, Iran
| Date of Web Publication | 21-Sep-2016 |
Correspondence Address:
Mina Fazlollahi Mohammadi
Department of Health Education and Health Promotion, School of Health, Isfahan University of Medical Sciences, Isfahan
Iran
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2468-6565.190978

Introduction: The different prevalence of metabolic syndrome in numerous populations justifies its determination in order to assist design strategies for screening programs to prevent long-term complications. Then, the current survey was aimed to determine the prevalence of metabolic syndrome in infertile women referring to an infertility clinic in Isfahan city.
Materials and Methods: Prevalence of metabolic syndrome was determined in a cross-sectional survey conducted on 149 women require reproductive techniques in infertility clinics in Isfahan. These samples were selected using convenient sampling through patients referring in the clinic during January 2013 to June 2014. Metabolic syndrome was diagnosed according to National Cholesterol Education Programme Adult Treatment Panel III criteria.
Results: The mean age of women was 32.2 ± 5.3 years. Prevalence of metabolic syndrome was 33.4% (49 women). With regards to the findings, the most frequent feature of metabolic syndrome was abdominal circumference by 70% (103 women) and the lowest one was about blood sugar by 18.2% (12 patients).
Conclusion: The current results revealed that the prevalence of metabolic syndrome in infertile women was 33.4%, then screening of infertile women in terms of indicators of syndrome before entering the costly process of reproductive technology recommended due to its adverse effect on fertility. Keywords: Infertility, metabolic syndrome, prevalence
How to cite this article:
Kianpour M, Mohammadi MF, Kazami A, Ahmadi SM. X syndrome prevalence among infertile women need reproductive technology In vitro fertilisation and intracytoplasmic sperm injection. J Hum Health 2015;1:63-6 |
How to cite this URL:
Kianpour M, Mohammadi MF, Kazami A, Ahmadi SM. X syndrome prevalence among infertile women need reproductive technology In vitro fertilisation and intracytoplasmic sperm injection. J Hum Health [serial online] 2015 [cited 2018 Aug 21];1:63-6. Available from: http://www.jhhjournal.org/text.asp?2015/1/3/63/190978 |
| Introduction | |  |
Infertility is the couple inability to achieve pregnancy after 12 months regular and unprotected sexual relationship.[1],[2] Infertility imposes a huge burden on families. It might be followed by the consequences including the conflict in the family, violence, stigma, isolation and divorce.[3],[4] Infertility is in both primary and secondary form with the prevalence of 15% in both forms.[5] Infertility occurs nearly 37% in all infertile couples [6] and primary and secondary infertility have been reported 0.6–3.4% and 8.7–32.6%, respectively.[7] Vahidi et al. study (during 2004–2005) exploring the prevalence of infertility in all provinces of Iran showed that the history of primary infertility and infertility during the survey were 24.9% and 3.4%, respectively.[8] Infertility is associated with geographic and environmental conditions. In some West African communities, infertility rate is about 50% while it is reported 12% in some communities of West Europe. In addition, there are differences in developed countries in the way that infertility rate in this countries is 5.3–16.7% while fertility rates in less developed countries are 3.9–9.6%.[9],[10] Infertility might be caused by numerous male and female related factors. The reasons for female infertility include ovulation disorders, pelvic inflammatory disease, endometriosis, polycystic ovary syndrome (PCOS), a hormonal imbalance to cause spontaneous pregnancy and environmental factors such as exposure to chemicals and radiation, age over 30 years, poor weight (high decrease or weight gain), sports (excessive exercise, more than 60 min a day), stress and other factors such as alcohol and tobacco consumption.[11] Treatment of infertility depends on its cause. One of the factors affecting the success of reproductive techniques is mother weight. Obesity is a major concern for women's health and is one of the main symptoms of metabolic syndrome.[12],[13] Syndrome X or metabolic syndrome is defined to identify the at risk population of cardiovascular disease. This syndrome consisted of factors including visceral obesity, insulin resistance, hyperglycaemia, hypertension and dyslipidaemia.[14] Syndrome X is a complex multi-organ dysfunction that produced by several factors such as physical inactivity, eating habits and dysfunction of the hypothalamic-pituitary and adrenal.[15],[16] There are evidence of metabolic syndrome effects on fertility such as PCOS that is one of the causes of infertility.[17] The prevalence of metabolic syndrome in women with PCOS in different populations was explored. Its prevalence in America, Brazil, Hong Kong and Czech is 43, 28.4, 24.9 and only 1.6% in women.[17],[18],[19],[20] In a survey, the prevalence of this syndrome was 10–15% among men and women aged 30–39 years.[20] It seems that aforementioned age group included couples who are expecting to get pregnant. The difference in the prevalence of this syndrome in numerous populations justifies its necessity to help for designing preventing screening strategies and preventing long-term effects. So far, studies usually executed in prevalence of this syndrome in women with PCOS and then this study was aimed to estimate the prevalence of syndrome X in infertile women referring to infertility clinic in Isfahan city because of the limited number of studies on the consequences of the disorder and its prevalence in the population of infertile women.
| Materials and Methods | | |
Prevalence of metabolic syndrome was determined in a cross-sectional survey conducted on 149 women require reproductive techniques in infertility clinics in Isfahan. This centre is one of the infertility treatment centres that accepts patients referred from different provinces of the country. These samples were selected using convenient sampling through patients referring in the clinic during January 2013 to June 2014. Inclusion criteria were as follow: (1) Being eligible to treat by the reproductive technique diagnosed by a physician, (2) incline to participate in the study and (3) being Iranian. After selecting subjects at last visit of the doctor, researcher ask all women to test triglyceride (TG), high-density lipoprotein (HDL) and fasting blood sugar and abdominal circumference, height, weight, blood pressure (BP) and body mass index (BMI) were also measured by attending in the clinic of fertility and infertility of Isfahan city. Metabolic syndrome was diagnosed according to National Cholesterol Education Programme Adult Treatment Panel III (NCEP-ATP III) criteria.[21] Abdominal obesity equal to or more than 89 cm, levels of serum TGs equal to or more than 150 mg/dL, low serum levels of HDL cholesterol ≤50 mg/dL, high fasting blood glucose equal to or more than 110 mg/dL and high BP more than 130/85 mm Hg were accepted. Existences of three above criteria were considered as metabolic syndrome.[22] Seca fixed scale was used to determine the weight and cloth meter was applied to measure the height. Waist and hip circumferences were measured using a cloth meter with an accuracy of 0.1 cm. To ensure the accuracy of data, the measurement was performed twice and if there were differences in size, a third measurement was performed and the close average of two measurements was considered. The pressure gauge was used for measuring the BP after 5 min of rest. All anthropometric assessment was done by a person in Isfahan fertility and infertility centre. Blood biochemical tests were conducted by a laboratory in fertility and infertility centre to obtain fasting blood glucose, TGs and HDL.
To analyse data, SPSS IBM (version 19) statistical software and descriptive methods (mean, standard deviation and frequency table) and Chi-square and independent t-test were used. P value was taken 0.05 significant.
| Results | | |
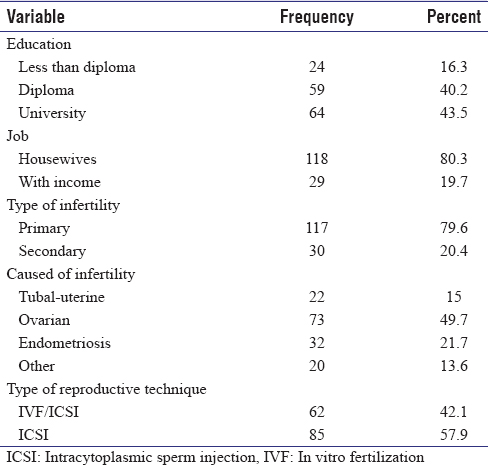
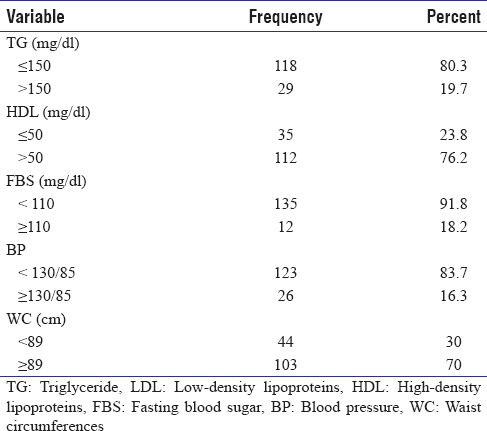
In this survey, 149 of eligible infertile women need reproductive techniques were included in the study. Two women were excluded due to the lack of testing for metabolic and in final the data collected from 147 infertile women were analysed. The mean age of women was 32.2 with a standard deviation of 5.3 years. In total, 43.5% had a university education and 80.3% were housewives. 79.6% had primary infertility and the ovarian problem was the most common causes of infertility 49.7%. Intracytoplasmic sperm injection (ICSI) was used by 57.9% of women as reproductive method [Table 1]. The prevalence of metabolic syndrome estimated 33.4% (49 women) according to the NCEP-ATP III. With regards to the current findings, the most frequent features of metabolic syndrome was associated with abdominal circumference by 70% (103 women) and the lowest was about blood sugar by 18.2% (12 patients) [Table 2]. The results suggest that 50 women (68.5%) were overweight (BMI 25–29.9) and obese (BMI 30 and above) from 73 infertile women with ovarian causes. While, 33 (44.6%) were overweight and obese from 74 infertile women caused by other factors that were statistically significant (P = 0.002). The results recommended that the group with metabolic syndrome, 36.2% required by ICSI/in vitro fertilisation and in the group without the syndrome, 44% used this technique for fertility. ICSI was conducted by 63.8 and 56% of women in groups with and without the syndrome, respectively.
| Discussion | | |
Prevalence of metabolic syndrome was 33.4% (49 patients) according to the NCEP-ATP III. The prevalence of this syndrome in women with PCOS was 43–46% in Ramezanali. study,[23] this prevalence is lower in the current study compare to Ramezanali that might be resulted by exploring women with all causes of infertility in the current study, while, in a study conducted by Ramezanali, women only with PCOS were studied. Hahn et al. reported that the prevalence of metabolic syndrome was 33.8% according to the International Diabetes Federation criteria for German women with PCOS, also revealed that this syndrome prevalence increased along with the rise in obesity and age.[24] Our study showed that the majority infertile women with ovarian causes were categorised in the overweight and obese groups. In a study in Brazilian women with PCOS, the prevalence of metabolic syndrome was 3.2, 19.2 and 52.3% according to normal, overweight and obese, respectively.[18] The current results inconsistent with the above findings showed that infertile women with ovarian factor had a significant increase in BMI compared to other causes of infertility. It seems that the increase of insulin and androgens in obese women may play an important role in developing PCOS and metabolic syndrome.[25] In our study, the frequency of abdominal circumference more than 89 cm by 70% had the most frequency compared to other indicators of this syndrome. The lowest frequency was about BP equal to or higher than 130/85 (16.3). Igosheva et al., study (2010) believed that despite the fat accumulation in the central region, often in obese women, waist-to-hip ratio increased and the chance of natural pregnancy decreased due to reducing this ratio <0.85.[26] Obesity can reduce the number and quality of oocytes, a decrease of the embryo, follicles and follicular atresia growth and an increase of abortion. To describe, The researchers suggest that central obesity is associated with a significant increase in intracellular lipid that accumulate (overtopping) fatty acids and the influence of the electrons from mitochondrial membrane and create an lipo-toxic condition in the genital tract of women and insulin resistance.[27] The prevalence of metabolic syndrome in women with PCOS had a higher prevalence in Sharpless study.[28] Other studies also reported the risk of this syndrome in women with PCOS 11 times higher compared to the control group.[29],[30] In our study, almost half of women (73 women, 49.7%) had infertility with ovarian factor which 29 women (20%), had metabolic syndrome, while from 74 infertile women with tubal causes, endometriosis and other causes, 20 women (14%) had metabolic syndrome. Although the prevalence of this syndrome among infertile women with ovarian causes was more than other causes, however, was not statistically significant. Studies also suggest that the prevalence of metabolic syndrome in women with the polycystic ovarian syndrome is more prevalent.[28] Then, it seems likely reasonable to achieve this result. In our study, infertile women were examined with all causes of infertility that can effect on the prevalence of X syndrome compared to other studies focused on women with PCOS.
| Conclusion | | |
According to the results of this study, the prevalence of metabolic syndrome in infertile women was 33.4%, then it recommend to screen infertile women by considering this syndrome criteria before engaging in costly process of reproductive technology.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Vayena E, World Health Organization. Current Practices and Controversies in Assisted Reproduction. Geneva: World Health Organization; 2002.  |
| 2. | Aflatoonian A, Baghianimoghadam B, Partovi P, Abdoli A, Hemmati P, Tabibnejad N, et al. A new classification for female infertility. Clin Exp Obstet Gynecol 2011;38:379-81. |
| 3. | Wiwanitkit V. Difference in physiogenomics between male and female infertility. Andrologia 2008;40:158-60. |
| 4. | Direkvand-Moghadam A, Delpisheh A, Khosravi A. Epidemiology of female infertility; A review of literature. Biosci Biotechnol Res Asia 2013;10:559-67. |
| 5. | Kumar D. Prevalence of female infertility and its socio-economic factors in tribal communities of Central India. Rural Remote Health 2007;7:456. |
| 6. | Unuane D, Tournaye H, Velkeniers B, Poppe K. Endocrine disorders and female infertility. Best Pract Res Clin Endocrinol Metab 2011;25:861-73. |
| 7. | Mascarenhas MN, Cheung H, Mathers CD, Stevens GA. Measuring infertility in populations: Constructing a standard definition for use with demographic and reproductive health surveys. Popul Health Metr 2012;10:17. |
| 8. | Vahidi S, Ardalan A, Mohammad K. Prevalence of primary infertility in the Islamic Republic of Iran in 2004-2005. Asia Pac J Public Health 2009;21:287-93. |
| 9. | Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of infertility prevalence and treatment-seeking: Potential need and demand for infertility medical care. Hum Reprod 2007;22:1506-12. |
| 10. | Gnoth C, Godehardt E, Frank-Herrmann P, Friol K, Tigges J, Freundl G. Definition and prevalence of subfertility and infertility. Hum Reprod 2005;20:1144-7. |
| 11. | Branch CP, Norris S. Reproductive Infertility: Prevalence, Causes, Trends and Treatments. Canada: Parliamentary Research Branch; 2001. |
| 12. | Pandey S, Bhattacharya S. Impact of obesity on gynecology. Womens Health 2010;6:107-17. |
| 13. | Kasturi SS, Tannir J, Brannigan RE. The metabolic syndrome and male infertility. J Androl 2008;29:251-9. |
| 14. | Dane B, Dane C, Kiray M, Koldas M, Cetin A. A new metabolic scoring system for analyzing the risk of hypertensive disorders of pregnancy. Arch Gynecol Obstet 2009;280:921-4. |
| 15. | Reaven G. Metabolic syndrome: Pathophysiology and implications for management of cardiovascular disease. Circulation 2002;106:286-8. |
| 16. | Jakovljevic M. Editorial: Treating the whole patient: Selective serotonin reuptake inhibitors and metabolic syndrome. Psychiatr Danub 2004;16:258-61. |
| 17. | Essah PA, Nestler JE. Metabolic syndrome in women with polycystic ovary syndrome. Fertil Steril 2006;86 Suppl 1:S18-9. |
| 18. | Soares EM, Azevedo GD, Gadelha RG, Lemos TM, Maranhão TM. Prevalence of the metabolic syndrome and its components in Brazilian women with polycystic ovary syndrome. Fertil Steril 2008;89:649-55. |
| 19. | Cheung LP, Ma RC, Lam PM, Lok IH, Haines CJ, So WY, et al. Cardiovascular risks and metabolic syndrome in Hong Kong Chinese women with polycystic ovary syndrome. Hum Reprod 2008;23:1431-8. |
| 20. | Vrbíková J, Vondra K, Cibula D, Dvoráková K, Stanická S, Srámková D, et al. Metabolic syndrome in young Czech women with polycystic ovary syndrome. Hum Reprod 2005;20:3328-32. |
| 21. | Royer M, Castelo-Branco C, Blümel J, Chedraui P, Danckers L, Bencosme A, et al. The US National Cholesterol Education Programme Adult Treatment Panel III (NCEP ATP III): Prevalence of the metabolic syndrome in postmenopausal Latin American women. Climacteric 2007;10:164-70. |
| 22. | Apridonidze T, Essah PA, Iuorno MJ, Nestler JE. Prevalence and characteristics of the metabolic syndrome in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2005;90:1929-35. |
| 23. | Ramezanali F. Prevalence of metabolic syndrome in women with polycystic ovary syndrome (Female Infertility). Int J Fertil Steril 2013;7:22-9. |
| 24. | Hahn S, Tan S, Sack S, Kimmig R, Quadbeck B, Mann K, et al. Prevalence of the metabolic syndrome in German women with polycystic ovary syndrome. Exp Clin Endocrinol Diabetes 2007;115:130-5. |
| 25. | Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet 2005;365:1415-28. |
| 26. | Igosheva N, Abramov AY, Poston L, Eckert JJ, Fleming TP, Duchen MR, et al. Maternal diet-induced obesity alters mitochondrial activity and redox status in mouse oocytes and zygotes. PLoS One 2010;5:e10074. |
| 27. | Robker RL. Evidence that obesity alters the quality of oocytes and embryos. Pathophysiology 2008;15:115-21. |
| 28. | Sharpless JL. Polycystic ovary syndrome and the metabolic syndrome. Clin Diabetes 2003;21:154. |
| 29. | Dokras A, Bochner M, Hollinrake E, Markham S, Vanvoorhis B, Jagasia DH. Screening women with polycystic ovary syndrome for metabolic syndrome. Obstet Gynecol 2005;106:131-7. |
| 30. | Azziz R. How prevalent is metabolic syndrome in women with polycystic ovary syndrome? Nat Clin Pract Endocrinol Metab 2006;2:132-3. |
[Table 1], [Table 2]
|









 Search Pubmed for
Search Pubmed for