|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 1
| Issue : 3 | Page : 72-76 |
|
Increasing physical activity for osteoporosis prevention among female students of Isfahan: A theory-based interventional study
Elaheh Tavassoli1, Mohtasham Ghaffari2
1 Department of Public Health, Faculty of Health, Shahrekord University of Medical Sciences, Shahrekord, Iran
2 Environmental and Occupational Hazards Control Research Center; School of Public Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran
| Date of Web Publication | 21-Sep-2016 |
Correspondence Address:
Mohtasham Ghaffari
Department of Public Health, Faculty of Health, Shahid Beheshti University of Medical Sciences, Tabnak Ave., Daneshjou Blvd., Velenjak, P. O. Box: 19835.35511, Tehran
Iran
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2468-6565.190972

Background: Undoubtedly regular physical activity has a crucial role in the prevention of many diseases, especially osteoporosis and also increasing mental and physical efficiency. Considering the importance of physical activity education for school age children, this study was performed to determine effect of health education on knowledge, perceptions and practice of the second grade middle schools' girl students in Isfahan related to osteoporosis preventive physical activity. Methodology: This is a quasi-experimental interventional study was conducted in Isfahan (2010). The research population encompasses 130 students that were randomly divided to groups, experimental (n = 66) and control (n = 64). The instruments for data collection were standard health belief model (HBM)-based scale and physical activity questionnaire. The standard scale was completed 3 times (before, immediately and 2 months after education) and physical activity questionnaire was completed 2 times (before and 2 months after education) by students of both groups. After pre-test, 4 educational sessions were performed in an experimental group. Finally, data collected and analysed by SPSS 16 software. Participation of individuals in this research was voluntary and with informed consent. Results: Findings showed that demographic characteristics of studied population in two groups were similar before intervention (P > 0.05). Before intervention, there were no significant differences between the scores of HBM structures in two groups (P> 0.001). After the intervention, it was observed significant differences in the levels of knowledge, perceived susceptibility, perceived severity, perceived benefits, perceived barriers and behaviour between experimental and control groups (P < 0.001). Conclusion: According results, intervention has a positive impact on the pattern of physical activity and it can be concluded that intervention is effective in increasing/improving the knowledge, individual perceptions and practice of the students. Keywords: Education, health belief model, osteoporosis, physical activity
How to cite this article:
Tavassoli E, Ghaffari M. Increasing physical activity for osteoporosis prevention among female students of Isfahan: A theory-based interventional study. J Hum Health 2015;1:72-6 |
How to cite this URL:
Tavassoli E, Ghaffari M. Increasing physical activity for osteoporosis prevention among female students of Isfahan: A theory-based interventional study. J Hum Health [serial online] 2015 [cited 2018 Aug 21];1:72-6. Available from: http://www.jhhjournal.org/text.asp?2015/1/3/72/190972 |
| Introduction | |  |
Osteoporosis is a skeletal disorder characterised by low bone mass and micro-architectural deterioration of bone tissue with a consequent increase in bone fragility and vulnerability to fracture.[1],[2],[3],[4],[5] A gradual reduction of bone density as a result of aging is normal. When a person basically has a low bone mass, or loses bone faster than normal, the risk of developing osteoporosis increases.[6] There are no specific statistics in Iran about the prevalence of osteopenia, osteoporosis and related fractures. However, Larijani in a study of osteoporosis rates in Iran (2005), reported an estimated 7 million of the 70 million people in Iran were at risk for fractures. In addition, the Research Centre for Endocrinology and Metabolism in Tehran University of Medical Sciences reported that in the subgroup of people who are more than 50 years old, 70% of the women and 50% of the men are suffering from osteoporosis or osteopenia.[7] Fortunately, osteoporosis is preventable by the adoption of certain health behaviours which could enhance bone mineral density, especially adequate (high-intensity/impact) weight-bearing physical activity and calcium intake.[8] Although, osteoporosis typically does not occur under 50 years of age, prevention programs must were began by engaging in both adequate weight-bearing physical activity and calcium consumption at early ages of life that the skeleton is growing, especially during childhood and adolescence - the time in the lifespan that bone is most efficiently built.[8] In general, regular physical activity started early in life is the safest and most available way to improve bone strength and reduce the propensity for falling. Early exercise builds greater amounts of bone so that it takes longer to deplete bone later in life.[9] Osteoporosis prevention educational interventions are given with the aim to provide education and to increase osteoporosis-related knowledge to lead to increased osteoporosis preventive behaviours, such as weight-bearing physical activity.[8] In a studies done to assess awareness, attitude and performance of different age and gender groups regarding osteoporosis in Iran and around the world, the study results showed that; people do not have suitable awareness, attitude and performance in this regard.[10],[11],[12],[13] The health belief model (HBM) is presented as the organizing theoretical framework for this research, which is also one of the oldest theories of health behaviour.
Despite the recommendation to provide an education on prevention and training throughout the life span, many programs focus on women who are approaching menopause or who are postmenopausal and therefore considered to be at higher risk for osteoporosis. Thus, despite extensive literature on treatment and diagnosis of osteoporosis, the numbers of studies of programs geared toward primary or secondary prevention are limited, especially those including younger adult women. This paper describes the results of a study that examines whether the application of the HBM can be used effectively to change the perception of middle school girls about their risk for developing osteoporosis and lead to a change in behaviour for prevention of this disease later in life.
Objective
Considering the importance of physical activity and its outcomes, especially in adolescents and also considering the important and determinant role of education in improving the level of regular physical activity, the present study aimed at investigating effect of health education based on HBM on the improvement of physical activity aimed at the prevention of osteoporosis in girl students in Isfahan.
| Methodology | | |
Participants
A total of 130 grade two students of female middle schools (aged 13–14 years) constituted the research population. After obtaining permission from the Isfahan University of Medical Sciences and presentation to the provincial education, the researcher entered the schools.
To begin with, the needed explanation was provided about the research goals, its advantages and completion of the questionnaires by the respondents. In addition, research subjects were informed about privacy and then those who consented were included in the study. They were aware of the confidentiality and gave their approval to participate in the study. Then, with giving the necessary explanations, the questionnaires were provided to students to be completed. Subsequently, all of the scales were given to subjects for responding. It was also requested that none of the questions be left blank and careful attention had to be provided to the answers. In the end, some gifts were given to each subject in order to appreciate their cooperation. The students were permitted to leave if they were not interested in participating in this study.
Inclusion criteria
School girls in the age range of 13–14 years.
Exclusion criteria
School girls with over 15 years are old, suffering from chronic diseases, difficult diseases, disability and student's reluctance in continuing the participation in the study.
Study design
This is an experimental interventional study was conducted in Isfahan (2010). The participants were recruited randomly from these two schools; this means that using attendance list, each student was given a code. Then, the samples were randomly selected from the code. 66 students were enrolled in the intervention group, and 64 students were enrolled in the control group.
Sampling was multistage as: Total number of districts in Isfahan was 5; district 3 was selected by simple random sampling for study. Then, the samples were selected from 2 schools by random sampling.
Data collection
Data gathering instrument was a 3-part questionnaire; the first part was used to obtain the demographic characteristics of the participants included items on age of parents, level of education and job of parents and the second one was a standard HBM-based questionnaire [14] that included: Knowledge regarding the importance of physical activity and understanding what is the appropriate level of physical activity? (α = 0.55), perceived susceptibility (for example: My chances of getting osteoporosis are great, because I have an especial body form, I think the probability of osteoporosis is high for me, within the next year I will get osteoporosis), (α = 0.78), perceived severity (I am afraid to even think about osteoporosis, if I get osteoporosis, I will be unable to do many things, if I get osteoporosis, my feeling about myself will be changed) (α = 0.80), perceived benefits of physical activity (physical activity prevents osteoporosis, if I do physical activity, I will have less concern about osteoporosis, when I do physical activity to prevent osteoporosis, I feel better) (α = 0.87), perceived barriers to physical activity (I don't like physical activity) (α = 0.71) (Baheiraei, 2005) and healthy behaviour action for osteoporosis prevention. Physical activity was assessed using the third part of the questionnaire (α = 0.78). 420 min a week, lower than 200 min a week and between 320 and 200 min a week were considered as desirable, undesirable and relatively desirable activity, respectively. The scoring method of the questionnaire in the knowledge part was each correct answer to the knowledge questions was given one point and 'I don't know' or incorrect answer was given zero points.
Perceptions questions including HBM constructs were designed by use of Lickert scale (from 'completely agree' to 'completely disagree') and each answer was given zero to four points: So that 'totally disagree' scored 0, 'disagree' 1, 'I have no idea' 2, 'agree' 3 and 'completely agree' scored 4. The scale scores of knowledge and attitude were calculated out of 100.
The questions of parts of the validity were confirmed by face validity and content validity. Knowledge and perceptions questionnaires were given to 30 students that were similar to the studied students in terms of demographic characteristics and 10 days later, only knowledge questions were given to the same 30 people again. After filling them out, the reliability of knowledge questions was confirmed by r = 0.84. Alpha of perceptions questions was estimated ≤0.7 and confirmed.
Study intervention
After completion of the questionnaire by both groups, the educational program was designed based on pre-test results and structures of HBM. Educational intervention in the experimental group was directly conducted through lecture, collaborative methods combined with questioning and answering, group discussion and brain storming in four sessions (45 min per each session).
HBM is one of the intrapersonal health education models (derived from behaviour science theory) which are administered for nutrition education in various subjects. The philosophy of this model that educators can result in creation or behaviour change include three characteristics; first is that; behaviour has benefits for health, economy, social, family and cultural, second; health educators know the barriers related to choosing behaviours and consider them for planning. Finally; the educational program should induce appropriate susceptibility among people that lack of health behaviour can result in side effects and complications including health hazards, economic, social and family hazards.
HBM constructs (perceived susceptibility, perceived severity, perceived benefits of physical activity and perceived barriers to physical activity) were utilised to formulate the strategies for the education. To evaluate the effectiveness of the educational interventional program, the data related to subjects' knowledge and attitudes (HBM structures) were collected by the same questionnaire immediately and 2 months after the program. This was carried out just 1-time (2 months follow-up) for physical activity. The students were informed that all data obtained were used without personal identifiers and were, therefore, confidential.
Statistical analysis
After confirming normal distribution of data with the Kolmogorov–Smirnov (k–s) test, to compare the difference of variables in pre- and post-exercise, repeated measured ANOVA, paired and independent sample t-test and Chi-square (with the level of 95% confidence) was used, and P < 0.05 was considered as criterion of statistical significance. SPSS-16, Inc., Chicago, IL, USA was employed to perform the statistical analysis. SPSS 16 software was used to analyse the data executing.
| Results | | |
The outcomes of the investigation of determining the normative data based on the k–s test results presented that values followed a normal distribution. In this study, 130 middle school female students from Isfahan fully cooperated with the researchers. The situation of experimental and control groups had been equal in their priority of the students in the family and their total number, the job and education of mother and father and economical situation of the family. In the first phase, there was no significant difference between two groups regarding: Individual perceptions about sensitivity, severity, benefits and barriers of osteoporosis. [Table 1] compares two groups' mean scores of knowledge and HBM constructs of perceived susceptibility, severity, barriers and benefits, in three phases as before intervention, immediately and 2 months after the program. For each of HBM constructs, R.M. ANOVA test indicated that the differences between groups were significant at before, immediately after and 2 months after intervention (P < 0.001). [Figure 1] shows health behaviour (Physical activity) of 2 groups before and 2 months after the intervention. As it presents, after educational program in experimental group and passing of 2 months, there was significant difference in the mean of perceptions and behaviour between before and after intervention in this group (P < 0.05). However, no significant differences observed in the mean of these variables in the control group between two stages (P > 0.05).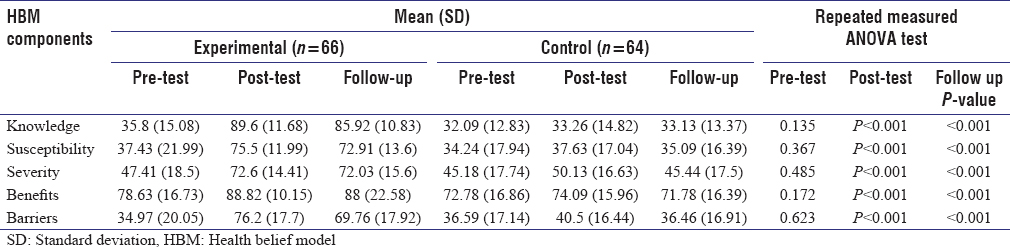 | Table 1: Comparing mean scorers of the students' knowledge and perceived susceptibility, severity, barriers and benefits about osteoporosis in 2 groups-pre, post and follow-up phases
Click here to view |
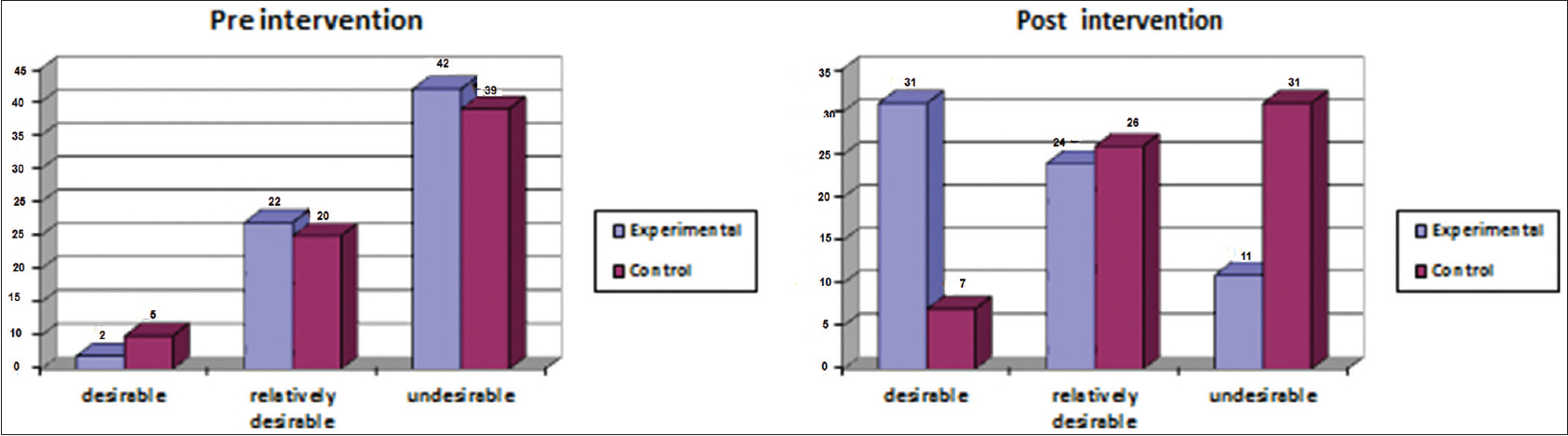 | Figure 1: Comparison of the students' physical activity in two groups during pre, post and follow-up phases
Click here to view |
| Discussion | | |
Osteoporosis is a serious public health problem that affects 20 million US women.[15] Health objectives indicate an urgent need and necessity to increase the number of women educated about osteoporosis.[15] The most effective osteoporosis reduction strategies include prevention through health education and health promotion. The results of present study showed that prior to intervention; all elements of HBM (perceived susceptibility, perceived severity, perceived benefits and perceived barriers) were below average in two groups. After intervention, participants in experimental group had significant improvement for behaviour assessed; while students of control group showed a slight change, this supports our hypothesis that a health education program based on HBM can be effective in promoting the adoption of behaviours by adolescent girls to prevent osteoporosis. Studies have identified several basic educational needs in participants, which increase their knowledge and change their intention to promoting preventive behaviours about osteoporosis. Knowledge of individuals about osteoporosis significantly increased after intervention in the experimental group. The findings of this study are consistent with the researches' results of Gammage et al., who carried out on osteoporosis health beliefs and knowledge in college students,[16] Brecher et al.,[9] Hazavehei et al.,[17] Giti and Nadia [18] and Sedlak et al.[19] Other findings of the present study indicated that perceived susceptibility, severity, barriers and benefits scores of participants were significantly enhanced after intervention in the experimental group. These results are similar and consistent with the findings of studies conducted by Brecher et al.,[9] Hazavehei et al.,[17] and Tussing and Chapman-Novakofski.[20] Given the prevalence of osteoporosis and the associated morbidity and mortality, it is important to increase knowledge of osteoporosis and encourage adoption of behaviours that help to prevent this condition, as opposed to waiting until the onset of the disease. The results of the study showed educational intervention focused on osteoporosis prevention is ideally suited to reach these goals of increased knowledge, perceived susceptibility, severity, barriers and benefits and adoption of prevention-oriented behaviour; based on findings about the performance of students related to physical activity, just 2 individuals (28.6%) from all of 66 students in experimental group had a desirable physical activity. Two months after education this reached the 31 cases (86.1%). The increase in performance of students in this study is also consistent with the findings of Giti and Nadia,[18] Hazavehei et al.,[17] Winzenberg et al.,[21] and Brecher's [9] researches who reported the change and improvement in behaviour of women. Childhood and adolescence are critical periods for the skeleton. Mechanical load has been shown during this period to be one of the best stimuli to enhance, not only bone mass, but also structural skeletal adaptations, both contributing to bone strength. Exercise prescription also includes a window of opportunity to improve bone strength in the late pre- and early pubertal period.[22]
| Conclusion | | |
The results of this study showed that applying constructs of the HBM can be valuable to enhance the effectiveness of an osteoporosis education program, and therefore, with regard to the important role of girls and women in foundation of families and the cost effectiveness of educational programs compared to treatment services, utilizing health education theories and models by the experts in schools is highly recommended to promote public health and well-being. Clearly, health system policy-makers must prepare educational programs based on HBM and there is a vital need to establish a national strategy for integrating preventive measures including lifestyle modification.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Lane NE. Epidemiology, etiology, and diagnosis of osteoporosis. Am J Obstet Gynecol 2006;194 2 Suppl: S3-11.  |
| 2. | Cooper C, Harvey N, Javaid K, Hanson M, Dennison E. Growth and bone development. Nestle Nutr Workshop Ser Pediatr Program 2008;61:53-68. |
| 3. | Ondrak KS, Morgan DW. Physical activity, calcium intake and bone health in children and adolescents. Sports Med 2007;37:587-600. |
| 4. | Bailey CA, Brooke-Wavell K. Exercise for optimising peak bone mass in women. Proc Nutr Soc 2008;67:9-18. |
| 5. | Hingorjo MR, Syed S, Qureshi MA. Role of exercise in osteoporosis prevention – Current concepts. J Pak Med Assoc 2008;58:78-81. |
| 6. | Kohrt WM, Bloomfield SA, Little KD, Nelson ME, Yingling VR; American College of Sports Medicine. American College of Sports Medicine Position Stand: Physical activity and bone health. Med Sci Sports Exerc 2004;36:1985-96. |
| 7. | Ghaffari M, Tavassoli E, Esmaillzadeh A, Hassanzadeh A. Effect of health belief model based intervention on promoting nutritional behaviors about osteoporosis prevention among students of female middle schools in Isfahan, Iran. J Educ Health Promot 2012;1:1-4. |
| 8. | Nguyen VU, Wang H, Waigandt ZE, Alexander C. The development of an osteoporosis prevention education intervention: Its effectiveness, conclusions, and recommendations. Am J Health Educ 2012;43:34-40. |
| 9. | Brecher LS, Pomerantz SC, Snyder BA, Janora DM, Klotzbach-Shimomura KM, Cavalieri TA. Osteoporosis prevention project: A model multidisciplinary educational intervention. J Am Osteopath Assoc 2002;102:327-35. |
| 10. | Keramat A, Patwardhan B, Larijani B, Chopra A, Mithal A, Chakravarty D, et al. The assessment of osteoporosis risk factors in Iranian women compared with Indian women. BMC Musculoskelet Disord 2008;9:28. |
| 11. | Thomas EA, Charles JC, Carpenter CR, Griggs LJ. Cecil Essentials of Medicine. 8 th ed. United States: WB Saunders; 2004. p. 502-30. |
| 12. | Bayat N, Einollahi B, Pourfarzian V, Alishiri G, Nemati E, Bagheri N, et al. Bone mineral density changes within 11 months of renal transplantation in Iranian patients. Transplant Proc 2007;39:1039-43. |
| 13. | Berarducci A. Senior nursing students' knowledge of osteoporosis. Orthop Nurs 2004;23:121-7. |
| 14. | Baheiraei A, Ritchie JE, Eisman JA, Nguyen TV. Psychometric properties of the Persian version of the osteoporosis knowledge and health belief questionnaires. Maturitas 2005;50:134-9. |
| 15. | Turner Lori W, Hunt Sharon B, DiBrezzo RO, Ches J. Design and implementation of an osteoporosis prevention program using the health belief model. Am J Health Stud 2004;19:115-25. |
| 16. | Gammage KL, Francoeur C, Mack DE, Klentrou P. Osteoporosis health beliefs and knowledge in college students: The role of dietary restraint. Eat Behav 2009;10:65-7. |
| 17. | Hazavehei SM, Taghdisi MH, Saidi M. Application of the Health Belief Model for osteoporosis prevention among middle school girl students, Garmsar, Iran. Educ Health (Abingdon) 2007;20:23. |
| 18. | Giti A, Nadia H. The effects of education on knowledge: View and function of women aged 45-65 regarding menopause and osteoporosis. Health Issues Adult Women 2006;2:56-62. |
| 19. | Sedlak CA, Doheny MO, Jones SL. Osteoporosis prevention in young women. Orthop Nurs 2000;17:53-60. |
| 20. | Tussing L, Chapman-Novakofski K. Osteoporosis prevention education: Behavior theories and calcium intake. J Am Diet Assoc 2005;105:92-7. |
| 21. | Winzenberg TM, Oldenburg B, Frendin S, De Wit L, Jones G. A mother-based intervention trial for osteoporosis prevention in children. Prev Med 2006;42:21-6. |
| 22. | Karl Karlsson M, Erik Rosengren B. Physical activity as a strategy to reduce the risk of osteoporosis and fragility fractures. Int J Endocrinol Metab 2012;10:527-36. |
[Figure 1]
[Table 1]
|









 Search Pubmed for
Search Pubmed for