|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 1 | Page : 8-11 |
|
Pattern of suicide in Nigeria: The Niger Delta Experience
SAU Offiah1, CC Obiorah2
1 Department of Anatomic Pathology, Abia State University Teaching Hospital, Aba, Abia State, Nigeria
2 Department of Anatomic Pathology, University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
| Date of Web Publication | 15-May-2014 |
Correspondence Address:
SAU Offiah
Department of Anatomic Pathology, Abia State University Teaching Hospital, PMB. 7004, Aba, Abia State
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.132550

Background: Suicide is becoming a major public health problem. Objective: To determine the pattern of suicide cases with respect to age, sex, and methods employed. Design: A 10-year retrospective study of suicide cases reported to the Coroner in Rivers and Abia states of Nigeria. Materials and Methods: Data on the age, sex, circumstances, and methods of all suicide cases handled by the authors were extracted and analyzed. Results: There were 32 cases (0.9%) of suicides out of a total of 3,555 medico-legal autopsies reviewed over the period. Of the 32 cases, 28 (87.5%) were males and 4 (12.5%) were females, giving a male to female ratio of 7:1. The age distribution showed a peak incidence in the third decade. The commonest method of committing suicide in this environment is by hanging. The range and mean of the ages is 16 - 64 yrs and 31 yrs, respectively. Conclusion: This review shows that the choice of how to die often depends on the most available and most convenient means at hand. Women chose less violent means of suicide such as drowning or poisoning, while males often chose violent methods such as hanging or firearms. Keywords: Autopsy, Coroner, Euthanasia, Suicide attacks, Suicide pact
How to cite this article:
Offiah S, Obiorah C C. Pattern of suicide in Nigeria: The Niger Delta Experience. J Med Investig Pract 2014;9:8-11 |
How to cite this URL:
Offiah S, Obiorah C C. Pattern of suicide in Nigeria: The Niger Delta Experience. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:8-11. Available from: http://www.jomip.org/text.asp?2014/9/1/8/132550 |
| Introduction | |  |
Suicide (Latin: Suicidium.) is the act of intentionally ending one's own life. Suicide is a common event in the Western world but is becoming a major public health problem even in Nigeria. It is often committed out of despair. In the United States, about 80 suicides occur per day, with more than 32,000 suicides per year, and 1500 unsuccessful suicide attempts per day, and it is the 4 th leading cause of death among the 18-65 year age group in the US. [1],[2]
Risk factors for suicide include among others, family history of suicide, access to guns, romantic break up, history of neglect or abuse, and history of hurting oneself on purpose. Certain symptoms or behaviors may often be shown by a person before suicide attempts, these include: Talking about feeling hopeless or guilty, pulling away from friends or not wanting to go out, giving away belongings, change in sleep and eating habits, losing interest in activities that had hitherto been of interest, including at school or work and having difficulty concentrating or thinking clearly, etc.
Suicide occurs in all ages and backgrounds, but certain groups of people are at increased risk for suicide attempts. [3 ] Suicide and suicide attempts often occur in people with mental disorders such as schizophrenia, autism, bipolar disorder, depression, and drug and alcohol abuse. Stressful life issues such as financial difficulties or relationship problems also play a major role in suicide behaviors. Suicide attempts are frequently prompted by quest for relief from guilt, shame, rejection, loneliness or loss. [3],[4]
Suicide offers a means of escape from harsh condition to some people in certain circumstances where living becomes unbearable. Some inmates in the infamous Nazi camps were said to have deliberately killed themselves by touching the electrified fences. [5],[6] In India, some debt-ridden farmers were known to have committed suicide as a means of escape from their excruciating debt. [7],[8] Males are more likely than females to commit suicide, but attempts are more common among females. [9],[10]
Some behavior are said to be suicidal, and they include actions such as self drug overdose or purposefully crashing a car. A situation whereby a person unleashes an act of violence against others to achieve a political or military goal, which simultaneously results in his or her own death, is referred to as suicide attack. Suicide bombings are regarded as an act of terrorism by the targeted community. Examples include "September 11 th attack" in the United States, attacks on the United Nations buildings at Abuja in Nigeria, and the Christmas day church attack in Niger State, Nigeria.
Mass suicides are performed under social pressure and are coordinated among a group of individuals. It can take place with as few as two people, in which case it is referred to as suicide pact. Mass suicide can also involve a larger group of people, such as occurred in cult suicide of "Jones Town," in which 918 members of the "Peoples Temple", an American cult led by Jim Jones, ended their lives by drinking Grape juice laced with cyanide, in 1978.
The ways societies view suicide vary widely according to religion and culture. The major religious groups - Judaism, Christianity, and Islam - as well as many African cultures, tend to view killing oneself as absurd. This is because suicide is considered to be the result of a mental illness. [11],[12],[13],[14] In some societies, suicide attempt is considered a criminal act.
The outlook of suicide is always grim. About 1/3rd of people, who attempted to commit suicide, will try it again within one year. About 10% of people, who threaten or attempted to commit suicide, will eventually kill themselves.[15] A suicide threat or attempted suicide should, therefore, never be ignored.
Although suicides are uncommon in Nigeria, cases are occasionally reported and autopsied, but there is paucity of publications in the literature. This work documents and analyzes suicide cases with a view to presenting the pattern and demographic features, which will avail tool for heightening preventive strategies.
| Materials and Methods | | |
The University of Port Harcourt Teaching Hospital (UPTH) and the Abia State University Teaching Hospital (ABSUTH) are located in the cities of Port Harcourt and Aba respectively, in the Niger Delta region of Nigeria. These hospitals serve as primary, secondary, and tertiary health care centers for Port Harcourt, Aba, and the rest of the adjourning states of Niger Delta region of Nigeria.
The coroner laws of both Rivers and Abia States require that bodies of individuals, who died suddenly, including suicide cases, should be reported to the police for investigation. This law is largely obeyed, especially in suicide cases, and autopsies are routinely carried out for each case. Usually, duplicate copies of the autopsy reports are archived by the pathologist, while the main copy is issued to the police.
This is a study of suicide autopsies referred to the pathologist and performed at the UPTH and ABSUTH over a 10-year period (1/1/2001 - 31/12/2010). Standard autopsy procedures were followed and histology done at the discretion of the pathologist. Personal data with brief summary of circumstances surrounding death were obtained from the coroner forms.
This work involved extracting and reviewing the data of the suicide autopsies between January 2001 and December 2010. The age, sex, and methods employed in committing suicides were analyzed, using descriptive methods such as tables and numerical indices to elucidate salient features.
| Results | | |
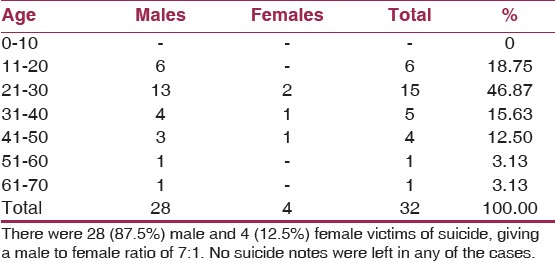
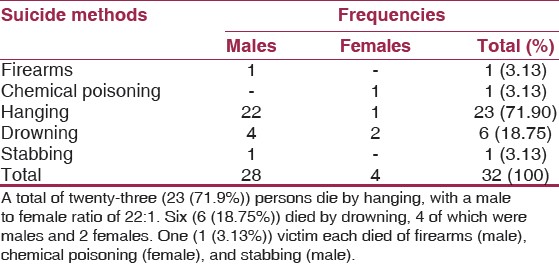
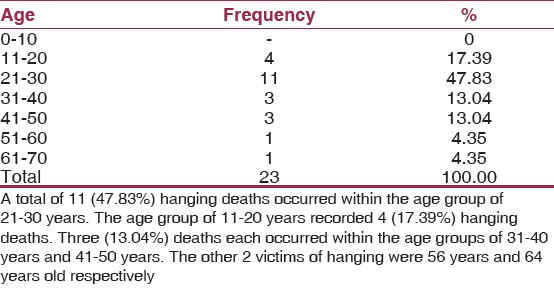
Three thousand,five hundred and fifty five(3,555) coroner autopsies were studied during the period. Out of this number,there were 32(0.9%) cases that died in circumstances consistent with suicide.[Table 1] shows that there were 28(87.5%) male and 4 (12.5%) female victims of suicide,giving a male to female ratio of 7:1.A total of 23(71.9%) persons died by hanging with a male to female ratio of 22:1 as shown in [Table 2]. [Table 3] shows that a total of 11 (47.83%) deaths by hanging occurred within the age group of 21-30 years.
| Discussion | | |
Suicide is a leading cause of death in the world. [1],[3],[6],[9] However, incidence of suicide in our environment is low, as shown by this study. Religious, cultural, and social influences militate against suicide in our environment.
The rate of suicide in our country is lower than that of countries like USA, China, UK, New Zealand, Japan, Spain, and Singapore, but it is near to that of Bahrain, Pakistan, and South Africa.
One reason for this difference may be the industrial development and degree of urbanization in the developed nations, whereby there is increased detachment of an individual from his social setup and a weakening of the individual's identification with his social group. Conversely, in our underdeveloped and rural environment, individuals are still avidly attached to their social milieu and there is, therefore, a strong individual identification with his social group, which controls and defines his actions.
The role of religion in one's life could be another important reason, especially the belief in the "world hereafter," which prevents the feeling of hopelessness - a feeling that has been described as an important predisposing factor for suicide. [12],[16 ] Africans in general, and Nigerians in particular, are highly religious people. Christianity and Islam respectively draw a major followership from our people. Every other person that is not a follower of any of these two religions would certainly be an adherent of the traditional African religion. The belief of these three religious groups is strongly rooted in the doctrine of "the world hereafter." Our people are, therefore, virtually devoid of the feeling of hopelessness; they are the easy-going type, and this may have also accounted for the low suicide rate in our country.
Male to female ratio of suicide in Niger Delta is 7:1. This gender ratio is similar to the accepted view of male dominance, [17],[18] and has also been reported in many other countries. [4],[19],[20] Some medical professionals believe this dominance stems from the fact that males are more likely to end their lives through effective violent means. This observation confirms the general view of the male sex being more aggressive and violent. The aggressive and violent attribute of males have been ascribed to the male sex hormone - testosterone.
About 66% of the suicides in our study occurred between the ages of 10 - 29 years. Only about 6% cases occurred above 50 years. This finding is contrary to the concept of increasing rate of suicide with advancing age in Western countries, and as revealed by studies in Japan, [21] Spain, [22] Denmark, [23] and US; [10],[24],[25] but it is closer to the age predilection reported in other less developed countries like Australia, Bahrain, Pakistan, and India. [20],[26],[27],[28] The reason for suicide at an early age in our study could be the social pressures of growing up, marital and domestic issues in cases of females (age 10-19 years), and the economic pressures and failure to achieve goals in cases of males (age 20-29 years) in their early years of economically independent existence.
In our study, the incidence of suicide decreased with advancing age and no cases were reported above 50 years in females and above 70 years in males. The reason for this could be our family system, which is close-nit. The elders usually relax and enjoy their advancing years with their grand children, because they are properly taken care of by their offspring. This is in addition to the increasing inclination towards religion with advancing age, usually noted in our setup.
Hanging, firearms, and poisoning, in that order, was the three most common methods of suicide in our study. This reasonably agrees with other studies conducted in different countries of the world. Hanging is the most common method of suicide in many countries. [2],[7],[8],[19],[20],[22],[27],[30]
The reason for the predilection for hanging and not others in our environment may be the ready availability of ropes and cords and the ease with which they are procured, because they cost little or nothing. Another reason may be the relative ease and swiftness with which hanging deaths occur, and the little or no attention the method attracts to a nearby person.
Poisoning is also amongst the common methods of suicide reported in many studies, [18],[26],[30],[31],[32] but only one victim of poisoning (a female) was recorded in our study; suicide was by ingestion of a locally concocted chemical "Otapiapia" used as rat poison and insecticide. This chemical is readily available and accessible in our environment.
Firearms have been reported as the method of choice in studies in USA, [2],[24],[33] amongst whites in South Africa, [6],[9] and among men in Italy, New Zealand, and Singapore. [19],[34],[35] In our study, only one victim (a male) died of firearms. The rarity of suicide commission by firearm is due to the fact that gun possession by individuals is unlawful in Nigeria and so is not readily available to all.
| Conclusion | | |
Incidence of suicide remains low in our environment, and like in other manners of death, males are more affected. Involvement of the productive age is a cause for concern as it has deleterious economic and social consequences for the nation. Availability and accessibility rather than lethality appear to be the major determining factors in the choice of suicide, with marked preponderance of death by hanging due to ready availability of ligature material. Prevention of suicide is a national imperative, and the approach has to be multidisciplinary.
| References | | |
| 1. | O′Connor RC, Platt S, Gordon J. International Handbook of Suicide Prevention: Research, Policy and Practice. p. 34-8. 
|
| 2. | "Center for Disease Control and Prevention": US Suicide Statistics 2005. Retrieved 2008. p. 646-53.
|
| 3. | Hawton K, van Heeringen K. Suicide. Lancet 2009;373:1372-81.
|
| 4. | O′Connor R, Sheehy N. Understanding suicidal behavior. Leicester: BPS Books; 2000. p. 33-7.
|
| 5. | Holt G. When suicide was illegal. Br J Psychiatry 2010;197:234-43.
|
| 6. | Ajdacic-Gross V, Weiss MG, Ring M. Methods of suicide: International suicide patterns derived from the WHO mortality database. Bull World Health Organ 2008;86:726-32.
|
| 7. | Khalid N. Pattern of suicide, causes and methods employed. J Comp Physicians Surg Pak 2001;11:759-61.
|
| 8. | Kanchan T, Menon A, Menezes RG. Methods of choice in completed suicide: Gender differences and review of literature. J Forensic Sci 2009;54:938-42.
|
| 9. | Voracek M. National intelligence and suicide rate: An ecological study of 85 countries. Pers Individ Dif 2004;37:543-53.
|
| 10. | Goldsmith SK. Reducing suicide: A national imperative. Washington D.C: National Academies Press; 2002. p. 141.
|
| 11. | Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: A national register-based study of all suicides in Denmark, 1981-1997. Am J Psychiatry 2003;160:765-72.
|
| 12. | Beck AT, Steer RA, Kovacs M, Garrison B. Hopelessness and eventual suicide: A 10-year prospective study of patients hospitalized with suicidal ideation. Am J Psychiatry 2008;142:559-63.
|
| 13. | Roberto T, Maurizio P, Paolo G. Suicide in psychiatric disorders. USA: Nova Science Publishers Inc; 2007. p. 266.
|
| 14. | Lee HC, Lin HC, Liu TC, Lin SY. Contact of mental and nonmental health care providers prior to suicide in Taiwan: A population-based study. Can J Psychiatry 2008;53:377-83.
|
| 15. | Ambade VN, Godbole HV, Kukde HG. Suicidal and homicidal deaths: A comparative circumstantial approach. J Forensic Leg Med 2007;14:253-60.
|
| 16. | Michael M. Religious Affiliation and Suicide Attempt. Cambridge: Cambridge University Press; 2010. p. 250-4.
|
| 17. | Brendel RW, Lagomasino IT, Perlis RH, Stern TA. The Suicidal Patient. In: Stern TA, Rosenbaum JF, Fava M, Biedrman J, Rauch SL, editors. Massachusetts General Hospital Comprehensive Clinical Psychiatry. Chap. 53. 1st ed. Philadelphia, Pa: Mosby Elsevier; 2008.
|
| 18. | Akhiwu WO, Nwosu SO, Aligbe JU. Homicide and suicide in Benin City, Nigeria. Anil Aggrawal′s Internet J Forensic Med Toxicol 2000;1:7-9.
|
| 19. | Solarino B, Nicolette EM, Di Vella G. Fatal firearm wounds: A retrospective study in Bari (Italy) between 1988and 2003. Forensic Sci Int 2007;168:95-101.
|
| 20. | Large MM, Nielssen OB. Suicide in Australia: Meta-analysis of rates and methods of suicide between 1988 and 2007. Med J Aust 2007;192:432-7.
|
| 21. | Ozawa-de Silva C. Too lonely to die alone: Internet suicide pacts and existential suffering in Japan. Cult Med Psychiatry 2008;32:516-51.
|
| 22. | Gac S. Suicide in Spain today. J R Soc Med 2006;1:25-31.
|
| 23. | Nordentoft M. Prevention of suicide and attempted suicide in Denmark. Epidemiological studies of suicide and intervention studies in selected risk groups. Dan Med Bull 2007;54:306-59.
|
| 24. | Way BB, Miraglia R, Sawyer DA, Beer R, Eddy J. Factors related to suicide in New York state prisons. Int J Law Psychiatry 2005;28:207-21.
|
| 25. | Gliatto MF, Rai AK. Evaluation and treatment of patients with suicidal ideation. Am Fam Physician 1999;5:1500-6.
|
| 26. | Al Ansari A, Hamadeh RR, Ali MK, El Offi A. Suicide in Bahrain in the last decade. J Forensic Sci 2007;28: 11-5.
|
| 27. | Khan MM, Hyder AA. Suicides in the developing world- A case study from Pakistan. Suicide Life Threat Behav 2006;36:76-81.
|
| 28. | Joseph A, Abraham S, Muliyil JP, George K, Prasad J, Minz S, et al. Evaluation of suicide rates in rural India using verbal autopsies, 1994-99. Br Med J 2003;326:1121-3.
|
| 29. | Wyatt JP, Wyatt PW, Squires TJ, Busuttil A. Hanging death in children. Am J Forensic Med Pathol 1998;19:343-6.
|
| 30. | Gunnell D, Hawton K, Kapur N. Coroner′s verdicts and suicide statistics in England and Wales. BMJ 2011;343:6030.
|
| 31. | Philips MR, Li X, Zang Y. Suicide rates in China, 1995-99. Lancet 2002;359:835-40.
|
| 32. | Nwosu SO, Odesami WO. Pattern of suicide in Ile Ife, Nigeria. West Afr J Med 2001;20:259-62.
|
| 33. | Cole JC, Walter HJ, DeMaso DR. Suicide and attempted suicide. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, editors. Nelson Textbook of Paediatrics. Chap. 25. 19 th ed. Philadelphia, Pa: Saunders Elsevier; 2011.
|
| 34. | Beautrais AL. Suicide in New Zealand II - A review of risk factors and prevention. N Z Med J 2003;116:400-1.
|
| 35. | Parker G, Yap HL. Suicide in Singapore: A changing sex ratio over the last decade. Singapore Med J 2001;42:11-4.
|
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for