|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 1
| Issue : 2 | Page : 52-56 |
|
Cranial base features between sagittal skeletal malocclusions in Anatolian Turkish adults: Is there a difference?
Hasan Kamak, Bülent Çatalbas, Burcu Senel
Department of Orthodontics, Faculty of Dentistry, Kirikkale University, Kirikkale, Turkey
| Date of Web Publication | 7-Aug-2013 |
Correspondence Address:
Hasan Kamak
Department of Orthodontics, Faculty of Dentistry, Kirikkale University, Kurtulus Mahallesi, 692. Sokak, No: 31, 71100 Merkez, Kirikkale
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.116287

Aim : The aim of this study to examine the differences between cranial base measurements and different skeletal malocclusion patterns in patients with Turkish cephalometric norms, data that will be useful in diagnosis and orthodontic and jaw surgery treatment planning. Materials and Methods : Cranial base measurements were made on lateral cephalometric radiographs of 90 healthy orthodontic patients with different skeletal malocclusions (Class I: 30 subjects, Class II: 30 subjects, Class III: 30 subjects) with a normal vertical growth pattern. Cranial base flexure measurements, anterior and posterior cranial base inclinations, and linear measurements for the assessment of cranial base dimensions were analyzed. For statistical evaluation, one-way analysis of variance test was performed. Least significant differences test was used to determine the individual differences. Results : Both anterior (SN) and posterior (SBa) cranial base lengths, N-SBa cranial base flexure angle and posterior cranial base inclination angle (SBa-FH) did not show statistically significant differences between the three groups studied. Anterior cranial base inclination (SN-FH) was increased significantly in the Class II group compared to Class I and Class III groups. N-S-Ar cranial base flexure angle was also increased significantly in the Class II group compared to Class III. Conclusions : Cranial base morphology differences among skeletal malocclusions were observed for the N-S-Ar and SN-FH angles in Class II group. Keywords: Cephalometric analysis, cranial base, skeletal malocclusions
How to cite this article:
Kamak H, Çatalbas B, Senel B. Cranial base features between sagittal skeletal malocclusions in Anatolian Turkish adults: Is there a difference?. J Orthod Res 2013;1:52-6 |
How to cite this URL:
Kamak H, Çatalbas B, Senel B. Cranial base features between sagittal skeletal malocclusions in Anatolian Turkish adults: Is there a difference?. J Orthod Res [serial online] 2013 [cited 2017 Apr 5];1:52-6. Available from: http://www.jorthodr.org/text.asp?2013/1/2/52/116287 |
| Introduction | |  |
The cranial base can affect the development of both the face and the cranium, because it plays a key role in craniofacial growth, assisting to unite different patterns of growth in various adjacent regions of the skull such as components of the pharynx, the oral cavity, the nasal cavity, and the brain. [1] Any changes in flexion due to variations in shape and size of this region would alter the sagittal skeletal relationship of the jaws since the cranial base consists of two segments articulating with the maxilla and mandible. [2],[3],[4] Therefore, the cranial base area has long been of interest to orthodontists. [3]
Although the cranial base angle is relatively stable and it shows large individual variations. [2] Cranial base features for different ethnic and racial groups have been established previously in many studies. Most researchers have concluded that there are significant differences among these groups and many cranial base standards have been developed for the different groups. [1],[2],[3],[4],[5],[6] These studies indicate that normal measurements for each group should not be considered normal for every other race or ethnic group. Therefore, it is important to develop individual standards for each population. Different racial groups must be treated according to their own characteristics. [7]
A limited number of studies have been carried out to evaluate the differences between cranial base measurements and different skeletal malocclusions. However, we have not found any published study evaluating the differences between cranial base measurements and different skeletal malocclusions in Turkish patients with Turkish cephalometric norms. [8],[9] Therefore, knowledge of the differences between the cranial base morphology and different skeletal malocclusions in Turkish patients is a new contribution to the current orthodontic literature in this field.
On the basis of these facts, the aim of this study was to examine the differences between cranial base measurements and different skeletal malocclusion patterns in patients with Turkish cephalometric norms, data that will be useful in diagnosis and orthodontic and jaw surgery treatment planning.
| Materials and Methods | | |
The present study was carried out on the lateral cephalometric radiographs of three groups selected from the archives of the Orthodontic Department of Kirikkale University. Because this study was a retrospective archive study, no ethical approval was needed.
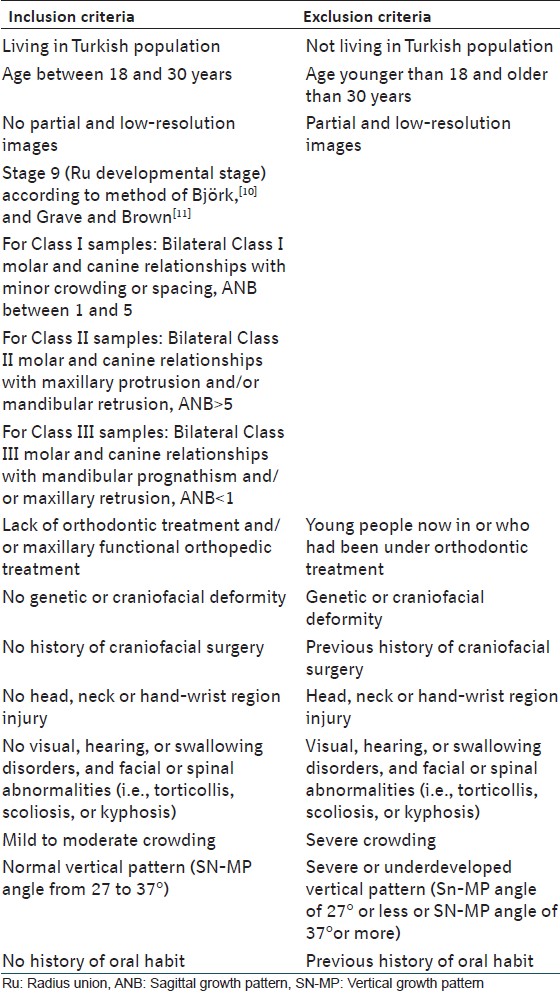
The lateral cephalometric radiographs of 500 patients were analyzed and the criteria presented in [Table 1] were followed for sample selection. All of the patients were at the stage 9 (Ru developmental stage [Complete union of epiphysis and diaphysis of radius]) according to the hand-wrist maturation method described by Björk, [10] and Grave and Brown. [11] A power analysis established by G*Power, version 3.1.3 (Franz Faul, Universität Kiel, Kiel, Germany) software, based on 1:1 ratio between groups, with sample size of 30 patients, would give more than 70% power to detect significant differences with 0.40 effect size and at the α = 0.05 significance level. And thus, of 500 radiographs, 90 radiographs including the criteria were randomly selected and included in the present study.
The radiographs were classified into three groups on the basis of different skeletal malocclusions with the normal vertical relationship (SN-MP angle, 32 ± 5° [8],[9] ) The Class I malocclusion group (bilateral Class I molar and canine relationships with minor crowding or spacing, ANB = 1-5° [8],[9] ) comprised 30 patients-14 girls and 16 boys (mean age, 16.71 ± 2,7 years), the Class II malocclusion group (bilateral Class II molar and canine relationships with maxillary protrusion and/or mandibular retrusion, ANB > 5° [8],[9] ) comprised 30 patients - 15 girls and 15 boys (mean age, 16.58 ± 2.6 years), and the Class III malocclusion group (bilateral Class III molar and canine relationships with mandibular prognathism and/or maxillary retrusion, ANB < 1° [8],[9] ) comprised 30 subjects - 16 girls and 14 boys (mean age, 16.74 ± 3.0 years). A total of 90 radiographs were evaluated. [Table 2] shows sample characteristics according to malocclusion. Dental plaster models were used in the determination of dental malocclusions.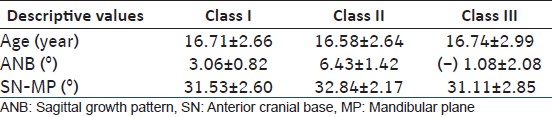 | Table 2: Mean values (±standard deviati ons) for age, ANB, and SN-MP in patients with Class I, Class II, and Class III malocclusions
Click here to view |
All assessments were performed by the same investigator (B.S) in a darkened room with a radiographic illuminator to ensure contrast enhancement of landmarks. The following anthropological landmarks were plotted: [1] A point (A), B point (B), sella (S), nasion (N), articulare (Ar), basion (Ba), gonion intersection (Go), menton (Me), porion (Po), orbitale (Or). The following measurements were used: [1] a0 ngular measurements for the assessment of sagittal growth pattern (ANB), vertical growth pattern (SN-MP), cranial base flexures (N-S-Ar, N-S-Ba), anterior and posterior cranial base inclinations (SN-FH, SBa-FH), and linear measurements for the assessment of cranial base dimensions (S-N, S-Ba) [Figure 1]. | Figure 1: The measurement points and reference lines used in the study: A point (A), B point (B), sella (S), nasion (N), articulare (Ar), basion (Ba), gonion intersection (Go), menton (Me), porion (Po), orbitale (Or), anterior cranial base (SN), sagittal growth pattern (ANB), vertical growth pattern (SN-MP), Frankfort horizontal plane (FH), cranial base flexures (N-S-Ar, N-S-Ba), anterior and posterior cranial base inclinations (SN-FH, SBa-FH), and cranial base dimensions (S-N, S-Ba)
Click here to view |
Statistical Analysis
The Kolmogorov-Smirnov test was applied to the data and it showed that the data were normally distributed. Thus, statistical evaluation was performed using parametric tests. Descriptive data and standard deviation values were calculated for each measurement. Statistical comparisons of each parameter in subjects in different malocclusion groups were compared to one-way analysis of variance (ANOVA) and least significant differences (LSD) test.
To determine the presence of any errors typically associated with digitizing and measurements, 30 radiographs were selected randomly for examination. All procedures such as landmark identification, tracing, and measurement were repeated on these 30 radiographs 3 weeks after the first examination, by the same investigator. A paired t-test was applied to both the 1 st set and 2 nd set of measurements and no significant difference was found between the two settings. Intra-class correlation coefficients were performed to assess the reliability of the measurements as described by Houston, [12] and the coefficients of reliability for the measurements were above 0.90. All statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS), version 16.0 (SPSS Inc., Chicago, Ill). When the P value was less than 0.05, the statistical test was determined to be significant.
| Results | | |
[Table 2] and [Table 3] show the mean and standard deviations for ages, ANB and SN-MP, and linear and angular measurement of the cranial base morphology of the subjects in each skeletal class, respectively. Both ages and SN-MP measurements showed no significant differences between the groups.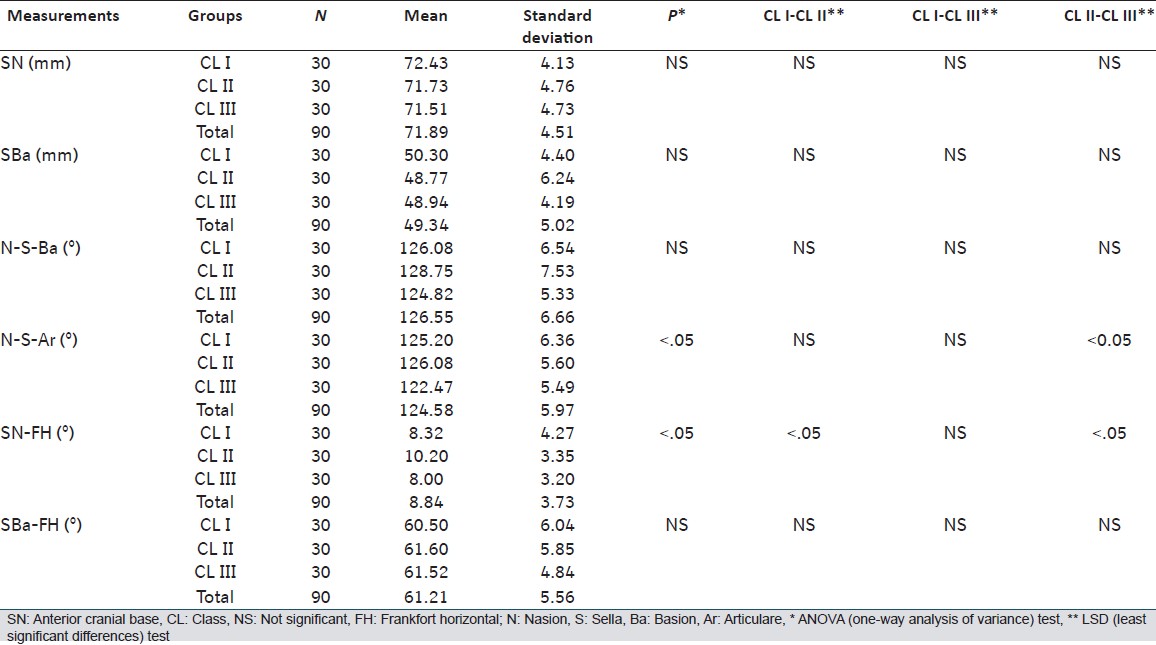 | Table 3: Mean and standard deviati ons of the measurements and comparison of groups with ANOVA* and LSD** tests
Click here to view |
The linear measurements for the assessment of cranial base dimensions were evaluated according to both anterior cranial base length (SN) and posterior cranial base length (SBa) measurements. Both SN and SBa measurements showed no significant differences between the groups.
The angular measurements for the assessment of cranial base flexure were evaluated according to N-S-Ba and N-S-Ar measurements. N-S-Ba angle was the lowest in Class III, the greatest in Class II, and intermediate in Class I. However, no significant differences were found between the groups for N-S-Ba parameter. Similarly, N-S-Ar angle was also the lowest in Class III, the greatest in Class II, and intermediate in Class I. Significant differences were only found between Class II and Class III groups according to the results of the LSD test (P < 0.05). The N-S-Ar angle was significantly increased in Class II compared to Class III (P < 0.05).
The SN-FH angle, measured for the assessment of anterior cranial base inclination, showed significant differences between the groups (P < 0.05). The SN-FH angle was significantly increased in Class II group compared to Class I and Class III groups (P < 0.05).
The SBa-FH angle, measured for the assessment of posterior cranial base inclination, showed no significant differences between the groups.
| Discussion | | |
Previous studies have tried to find a correlation between cranial base features and sagittal malocclusions; however, most of these have paid attention to vertical height and differences in the samples studied. As is known, at the 13 th year of life, the cranial base reaches 90% of its adult size. [1] Therefore, this study aimed to eliminate possible changes in facial divergence and individual growth and development, and the SN-MP angle and Ru development stage were similar in all three groups. In addition, the most possible factors that influence the occurrences of a skeletal anomaly, that is small or big jaws, any oral habit were excluded in choosing the samples.
In previous studies, SN and SBa, and N-S-Ba and N-S-Ar were widely used to measure of anterior and posterior cranial base lengths and cranial base angles, respectively. However, the differences between these measurements and sagittal malocclusions are still debated. Therefore, these measurements were used in this study.
In this study, Frankfort horizontal plane was selected as the reference plane because of physiologic relation between the ear and the eye as represented by Po and orbital. [13],[14] The variation of the Frankfort horizontal plane, which represents a horizontal to the earth's surface, has been shown to vary around 0°. [14],[15]
Although the maxilla is connected with the cranial base's anterior part and the mandible's rotation is influenced by the maxilla, a relationship can be found between the cranial base morphology and sagittal malposition of the jaws. [1] In this study, the anterior and posterior cranial base lengths and cranial base angle measured from Ba except for Ar showed no significant differences between the sagittal malocclusions. In agreement with our findings, Polat and Kaya, [1] Ildwein et al., [16] Kasai et al. [17] and Wilhelm et al. [18] reported similar findings. On the other hand, Hopkin et al. [3] reported that the cranial base length and angle increase from Angle Class III through Class I to Class II division 1 malocclusion. SN and SBa were significantly larger in Class II malocclusion than in Class I subjects, but the measurements were very similar in Class I and Class III. Kerr and Adams, [19] found a higher BaSN angle in Class II patients than Class I patients. Dibbets, [20] also found smaller N-S-Ba angle and shorter SN and SBa from Angle Class II, through Class I, to Class III subjects. Järvinen, [21] reported that Class II patients showed a higher N-S-Ar angle than Class III patients; this was in agreement with our results.
Although the SN-FH angle was significantly increased in Class II group compared to Class I and Class III groups (P < 0.05), the SBa-FH angle showed no significant differences between the groups in this study. Contrary to our findings, Polat and Kaya, [1] found that both anterior and posterior cranial base inclinations were significantly increased in Class III group compared to Class I and Class II groups. The Class II group showed increased cranial base inclinations and flexures that might have resulted in backward positioning of the jaw.
The whole disagreements between our findings and these author's findings might be due to the racial differences and case selection procedures (i.e., age, ANB, SN-MP angle, number of person and developmental stage). In our study, cases were Turkish patients with Turkish cephalometric norms. As has been shown in numerous studies, the cranial base angles (flexures and inclinations) alone do not appear to play a significant role in the determination of malocclusion.
As a result;
- The differences among different skeletal malocclusions may be taken into account in patients undergoing orthodontics or corrective jaw surgery, both during diagnosis and treatment planning.
- The N-S-Ar angle was significantly increased in Class II group compared to Class III group (P < 0.05).
- The SN-FH angle was also significantly increased in Class II group compared to Class I and III groups (P < 0.05).
| References | | |
| 1. | Polat OO, Kaya B. Changes in cranial base morphology in different malocclusions. Orthod Craniofac Res 2007;10:216-21. 
[PUBMED] |
| 2. | Proff P, Will F, Bokan I, Fanghänel J, Gedrange T. Cranial base features in skeletal Class III patients. Angle Orthod 2008;78:433-9.
|
| 3. | Hopkin GB, Houston WJ, James GA. The cranial base as an aetiological factor in malocclusion. Angle Orthod 1968;38:250-5.
[PUBMED] |
| 4. | Dhopatkar A, Bhatia S, Rock P. An investigation into the relationship between the cranial base angle and malocclusion. Angle Orthod 2002;72:456-63.
[PUBMED] |
| 5. | Klocke A, Nanda RS, Kahl-Nieke B. Role of cranial base flexure in developing sagittal jaw discrepancies. Am J Orthod Dentofacial Orthop 2002;122:386-91.
[PUBMED] |
| 6. | Siriwat PP, Jarabak JR. Malocclusion and facial morphology is there a relationship? An epidemiologic study. Angle Orthod 1985;55:127-38.
[PUBMED] |
| 7. | Basciftci FA, Uysal T, Buyukerkmen A. Determination of Holdaway soft tissue norms in Anatolian Turkish adults. Am J Orthod Dentofacial Orthop 2003;123:395-400.
[PUBMED] |
| 8. | Gazilerli U. The Steiner norms between 13-16 years old Turkish children with the normal occlusion on the region of Ankara (master thesis). Turkey: Ankara University; 1976.
|
| 9. | Celikoglu M, Kazanci F, Miloglu O, Oztek O, Kamak H, Ceylan I. Frequency and characteristics of tooth agenesis among an orthodontic patient population. Med Oral Patol Oral Cir Bucal 2010;15:e797-801.
[PUBMED] |
| 10. | Björk A. Timing of interceptive orthodontic measures based on stages of maturation. Trans Eur Orthod Soc 1972;:61-74.
|
| 11. | Grave KC, Brown T. Skeletal ossification and the adolescent growth spurt. Am J Orthod 1976;69:611-9.
[PUBMED] |
| 12. | Houston WJ. The analysis of errors in orthodontic measurements. Am J Orthod 1983;83:382-90.
[PUBMED] |
| 13. | Ricketts RM, Schulhof RJ, Bagha L. Orientation-sella-nasion or Frankfort horizontal. Am J Orthod 1976;69:648-54.
[PUBMED] |
| 14. | Andria LM, Leite LP, Prevatte TM, King LB. Correlation of the cranial base angle and its components with other dental/skeletal variables and treatment time. Angle Orthod 2004;74:361-6.
[PUBMED] |
| 15. | Downs WB. Variations in facial relationships; their significance in treatment and prognosis. Am J Orthod 1948;34:812-40.
[PUBMED] |
| 16. | Ildwein M, Bacon W, Turlot JC, Kuntz M. Specifications and major discriminants in a Class II division 1 population. Rev Orthop Dento Faciale 1986;20:197-208.
[PUBMED] |
| 17. | Kasai K, Moro T, Kanazawa E, Iwasawa T. Relationship between cranial base and maxillofacial morphology. Eur J Orthod 1995;17:403-10.
[PUBMED] |
| 18. | Wilhelm BM, Beck FM, Lidral AC, Vig KW. A comparison of cranial base growth in Class I and Class II skeletal patterns. Am J Orthod Dentofacial Orthop 2001;119:401-5.
[PUBMED] |
| 19. | Kerr WJ, Adams CP. Cranial base and jaw relationship. Am J Phys Anthropol 1988;77:213-20.
[PUBMED] |
| 20. | Dibbets JM. Morphological associations between the Angle classes. Eur J Orthod 1996;18:111-8.
[PUBMED] |
| 21. | Järvinen S. Saddle angle and maxillary prognathism: A radiological analysis of the association between the NSAr and SNA angles. Br J Orthod 1984;11:209-13.
|
[Figure 1]
[Table 1], [Table 2], [Table 3]
|










 Search Pubmed for
Search Pubmed for