|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 27-31 |
|
Skeletal class III treatment with mini-screw-assisted memory screw-facemask combination: A pilot study
Bayram Çörekçi, Koray Halicioilu, Celal Irgin, Saffet Dursun
Abant Izzet Baysal University, Faculty of Dentistry, Department of Orthodontics, Bolu, Turkey
| Date of Web Publication | 29-Jan-2014 |
Correspondence Address:
Bayram Çörekçi
Abant Izzet Baysal University, Faculty of Dentistry, Department of Orthodontics, Bolu
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.125920

Background: The aim of this study was the evaluation of treatment outcomes after using mini-screw-assisted memory screw-facemask combination in early permanent dentition Class III malocclusion. Materials and Methods: Treatment of six subjects (mean age 11.5 ± 1.1 years) was investigated clinically and by using pre- and post-treatment cephalograms. An anchorage unit was prepared by placing two mini-screws just behind a line connecting the first premolars at the mesial contact point. With the memory expansion screw (500 g), two mini-screws were placed parallel to the occlusal plane to provide stable, four-point support for the appliance. Wire segments were added along the palatal surfaces of the buccal teeth, annealing the terminal ends and then bending the ends into hooks for attachment of reverse-pull facemask elastics. The memory screw was activated twice a day and the facemask was prescribed for 16 h wear, using ¼ inch, 400 g elastics (in total 800 g) extending crosswise from the lingual arms on the expander. Pre- and post-treatment differences were tested for statistical significance using paired t-test. Results: All appliances remained stable during treatment. Mean treatment was for 4.8 ± 1.5 months. There was a significant improvement in skeletal sagittal values: SNA, +2.6°; SNB, −1.4°; ANB, +4.0°; WITS appraisal, +4.6 mm; and overjet, +2.9 mm. In relation to A point, the upper first molars moved mesially about 0.9 mm. Conclusions: The mini-screw-assisted memory screw-facemask combination seems to be effective for skeletal Class III treatment in early permanent dentition. Keywords: Class III malocclusion, face mask, hybrid memory hyrax, rapid maxillary expansion
How to cite this article:
Çörekçi B, Halicioilu K, Irgin C, Dursun S. Skeletal class III treatment with mini-screw-assisted memory screw-facemask combination: A pilot study. J Orthod Res 2014;2:27-31 |
How to cite this URL:
Çörekçi B, Halicioilu K, Irgin C, Dursun S. Skeletal class III treatment with mini-screw-assisted memory screw-facemask combination: A pilot study. J Orthod Res [serial online] 2014 [cited 2018 Mar 27];2:27-31. Available from: http://www.jorthodr.org/text.asp?2014/2/1/27/125920 |
| Introduction | |  |
Class III malocclusions are characterized by no or negative overjet and concave profile and result from maxillary hypoplasia, mandibular hyperplasia, or a combination of them. [1] They may also be skeletal or dental in origin. [2] Traditionally, prognathic mandible inevitably needs surgical correction after the completion of growth and retrognathic maxilla treatments involve the use of a protraction facemask (FM) with or without rapid maxillary expansion (RME), especially at early ages. [1] The orthopedic correction of Class III malocclusion is accomplished by anterior and inferior movement of the maxilla and downward-backward rotation of mandible before adolescence. [1]
The RME/FM therapy is a combined single-phase treatment and produces some favorable skeletal and dentoalveolar modifications in both the maxilla and the mandible. Nowadays, RME is assumed as a kind of midpalatal suture distraction osteogenesis and stimulates midfacial sutures. [3],[4] The possible advantages of RME for this combined therapy are:
- It enhances protraction procedures by releasing surrounding sutures;
- It increases total nasal cavity volume;
- It enlarges pharyngeal airway space by increasing palatal diameter; and
- It also leads to improvement in respiratory function. [4],[5]
The RME can be done in the following ways: tooth-borne, tooth-/tissue-borne, or bone-borne. Tooth-borne and tooth-/tissue-borne appliances have some well-known disadvantages such as dental or alveolar buccal tipping, gingival recessions, mucosal inflammation, and root damage. Moreover, bone-borne RME needs highly invasive surgical insertion procedures and may also produce root lesions and some infections. [6],[7] Combining the advantages of tooth-borne and bone-borne expanders, Wilmes et al. presented the hybrid hyrax, a tooth- and bone-borne expander. [8] They placed two mini-screw paramedian to midpalatal suture in the anterior palate and two bands to the first molar. Afterward, a bended hyrax expansion screw was soldered to the bands and mini-screws. At the same time, Ludwig et al. used this new device for treatment of Class III malocclusion as an anchorage and expansion unit. [9] They concluded that FM and hybrid hyrax appliance combination can treat moderate Class III malocclusions. [9]
The expansion screw of the RME appliance is generally hyrax screw. Recently, a memory-type expansion screw was introduced to produce continuous, stable, and physiological force during treatment. [10] As an alternative approach, a memory expansion screw can be used with mini-screws and molar bands; thus, maxillary expansion and protraction can be achieved for the treatment of Class III malocclusion. The aim of this prospective study was to investigate the treatment effects produced by the hybrid memory hyrax FM combination in growing Class III patients.
| Materials and Methods | | |
The sample consisted of patients with a mild to severe skeletal Class III malocclusion (WITS appraisal ≤2.0 mm) treated with a hybrid memory hyrax, FM, and heavy extraoral elastics. A pilot sample consisted of six patients (two males and four females; mean age of 11.5 ± 1.1 years) treated by a single operator (B. C.). This prospective study was approved by the ethics committee of the Abant Izzet Baysal University. An informed consent was signed by the parents of the patients before treatment.
Treatment began with the placement of orthodontic bands to the maxillary first molars. Then, local anesthesia was applied palatinally in the anterior palate. For insertion of mini-screws, palatal mucosa was punched just behind a line connecting the first premolars at the mesial contact point, about 6 mm behind the incisal papillae. The mini-screws should be less than 3 mm away from the midpalatal suture to ensure adequate bone thickness. [8],[9] A drill (1 mm in diameter) was used for opening a guidance road about 4 mm from punch holes. Tomas mini-implants (Tomas Anchorage System; Dentaurum, Ispringen, Germany) of size 2 × 8 mm (1.6 mm in diameter) were inserted at approximately parallel angulations manually. Abutments (Trimed, Ankara, Turkey) [stainless steel (SS)], which allow direct silver soldering of the mini-memory expansion screw arms, were placed to take silicon impression and were also used to transfer the mini-implant location to the plaster cast. To produce identical mouth as that of patient, molar bands and transfer mini-screws fitted in abutments in silicon and a high-strength dental stone cast were made.
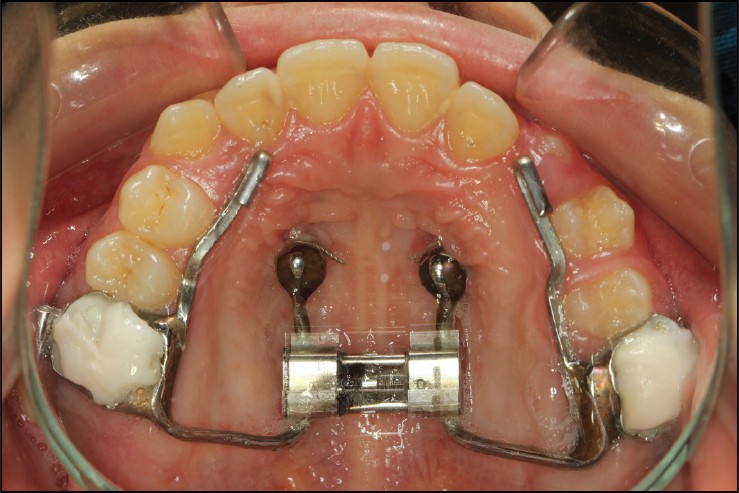
The abutments were placed over the mini-screw heads, and then a split memory screw (500 g Memory Expander Type S; Forestadent, Pforzheim, Germany) was bent and adapted to the abutments and the molar bands. For attachment of FM elastics, an additional SS wire segment (1.5 mm in diameter) was bent as hooks along the palatal surfaces of the buccal teeth. The hooks were positioned at the palatal canine region to enable a line of force anterior to the center of resistance of the maxilla. Fabrication of hybrid memory expansion unit was made by silver soldering between the abutments, memory expansion screw, molar bands, and SS wire hook segments [Figure 1]. It luted with light curing glass ionomer cement (Ultra Band Lock, Reliance, IL, USA). With two mini-screws and two molar bands, hybrid memory expansion unit was placed parallel to the occlusal plane to provide stable and four-point support for the appliance.
After delivery of the device, the sagittal split screw was activated twice a day by a 90° turn (0.2 × 2 = 0.8 mm) for 8-10 days, with the results evaluated weekly. A maxillary midline diastema appeared after about 10 days; overexpansion is advisable due to extremely narrow maxilla. Deactivation of the split screw was not needed because of the nature of memory expansion screw.
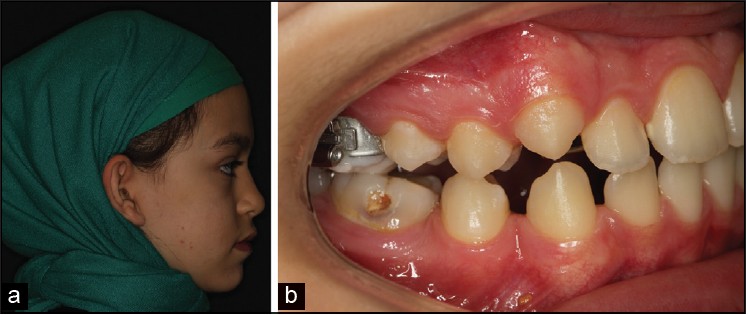
Protraction FM lasted for 4.8 ± 1.5 months immediately after RME activation [Figure 2], [Figure 3]a and b. The applied elastics were instructed for 16 h wear [¼ inch, 400 g (in total 800 g); Rocky Mountain Orthodontics, Denver, USA] extending crosswise from the lingual arms of the expander unit to FM to produce a caudal vector of force [Figure 4]. All Class III malocclusions were corrected by mini-screw-supported protraction and hybrid expansion units were left in situ for retention [Figure 5].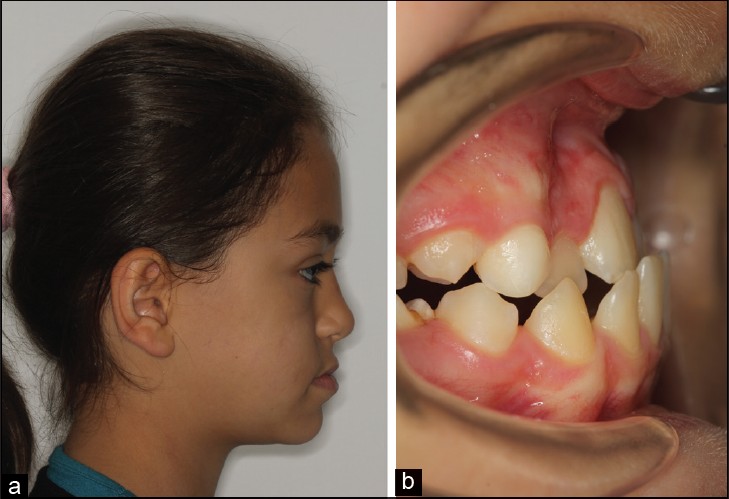 | Figure 3: A female patient with skeletal and dentoalveolar Class III malocclusion before treatment (a) face and (b) dentition
Click here to view |
Pre- and post-treatment lateral cephalograms of six patients were evaluated to assess changes in SNA and SNB angles, WITS appraisal, and overjet. To evaluate vertical effects, PP-MP and overbite changes were observed. Maxillary tooth movements were investigated to relate upper incisor inclination changes and changes in the distance between the upper first molar and A point. Pre- and post-treatment differences were tested for statistical significance using Wilcoxon test. The levels of significance used were P < 0.05 and P < 0.001. All analyses were performed using SPSS version 17 (SPSS Inc., Chicago, IL, USA).
| Results | | |
All mini-screws remained stable during treatment. Residual overexpansion was observed after the expansion phase in two patients by memory expansion screw. Treatment was associated with highly significant increases in SNA and ANB angles (P < 0.001) and significant decreases in SNB angle (P < 0.05). WITS appraisal and overjet (P < 0.001) showed highly significant improvement.
There were no significant vertical dimension differences regarding PP-MP and overbite changes, and also, any significant maxillary tooth movement was not found regarding upper incisor angle and distance between the upper first molar and A point [Table 1].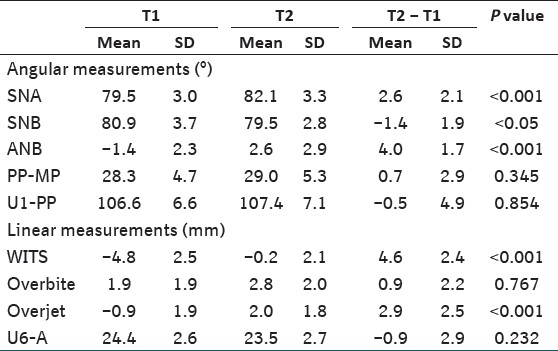 | Table 1: Comparison of cephalometric changes before (T1) and after treatment (T2)
Click here to view |
| Discussion | | |
The hybrid memory hyrax-FM combination was an effective treatment approach for orthopedic treatment of Class III malocclusion in early permanent dentition patients. Generally, maxillary protraction treatments with tooth-borne RME showed that Class III malocclusion problems were solved by more anterior tooth movement than the skeletal movement. [11] Anterior tooth movement, especially maxillary dental camouflage, can be avoided by employing temporary anchorage device in this Class III treatment combination. Mini-screw insertion sites in the anterior palate seem to be preferable because this area has enough bone for skeletal support of hybrid memory hyrax protraction unit. [12]
Moreover, it is proved those hybrid hyrax units have some positive skeletal effects regarding RME. [8] The memory screws could produce a continuous force ranging from 1.225 to 1.425 g, [13] and it is hypothesized that if the maxillary expansion has to become physiologically stable, the treatment time must be shorter and lower forces must be applied. [14] In the present situation, a memory expansion screw (500 g) with relatively low forces was employed to accomplish adequate maxillary expansion and these results are in accordance with the hypothesis for RME. [14]
When the sagittal dimension was evaluated, any possible changes could be determined using SNA angle and WITS appraisal in Class III treatment. In the present hybrid memory hyrax RME and FM treatment, the maxilla showed a significant increase and anterior movement in the measurements, which is parallel to the findings of a meta-analysis study. [15] Also, 2.6° increments of SNA were found in the current RME/FM therapy and it was than the meta-analysis study. [15] So, the current treatment approach could produce higher effectiveness on maxillary protraction than the conventional RME/FM treatment.
The nature of conventional RME/FM treatment generally may show anterior bite opening because maxillary posterior teeth move downward and the mandible shows clockwise rotation. [1] Vertical side effects such as bite opening could be minimized by placing the mini-screws more anteriorly in the palate, employing palatal segmental SS wires with hooks, and by applying elastic force in the anterior-caudal direction, like in this study. These vertical changes and advantages were proved by PP-MP angle and overbite distance which did not show any significant alterations in the present study.
It was advocated in the literature that if patients were treated at a younger age, the maximum skeletal effects could be achieved and that maxillary advancement is more acquirable if it is started before the age of 8 years. [15] In patients older than 8 years, skeletal effects may show reduced response and dental response, and the side effects may be increased with conventional RME/FM. In the current investigation, the mean age of patients was 11.5 ± 1.1 years and the hybrid memory hyrax RME/FM combination was advantageous in patients, in which was obtained more skeletal effects and no advanced root resorption. This treatment approach was a good choice for Class III patients who were at the age of early permanent dentition.
The hybrid memory hyrax RME/FM treatment approach showed no appliance failure and stable mini-implants during the entire treatment. It was observed in the current study that primary stability of the mini-implants was high and they remained stable. The underlying clarification for this high success rate is threefold:
- The anterior palate where the mini-implants are placed has very good bone quality;
- There are no root contacts or iatrogenic traumatic interference with anatomical structures; [16],[17] and
- A larger mini-implant diameter might improve the implant stability because of plentiful bone space in the insertion region. [18]
Therefore, the design and application of this biomechanical treatment approach could give excellent support to the mini-screws and they remained stable during treatment. Also, there was another advantage in using only two mini-screws, i.e. surgical procedures were minimally invasive compared to skeletal anchored transpalatal distractors.
| Conclusions | | |
In early permanent dentition Class III patients, the hybrid memory hyrax RME/FM combination seems to be effective for significant maxillary protraction with good orthopedic results. Clinically acceptable soft-tissue results can be achieved. Undesired maxillary tooth movements can be minimized by skeletal anchorage. This treatment approach involves comparatively low surgical invasiveness.
| Consent | | |
The authors state that the consent for using the photos was obtained from the child's parents.
| References | | |
| 1. | Toffol LD, Pavoni C, Baccetti T, Franchi L, Cozza P. Orthopedic treatment outcomes in Class III malocclusion. A systematic review. Angle Orthod 2008;78:561-73. 
[PUBMED] |
| 2. | Keles A, Tokmak EC, Erverdi N, Nanda R. Effect of varying the force direction on maxillary orthopedic protraction. Angle Orthod 2002;72:387-96.
[PUBMED] |
| 3. | Haas AJ. The Treatment of maxillary deficiency by opening the midpalatal suture. Angle Orthod 1965;35:200-17.
[PUBMED] |
| 4. | Nanda R. Biomechanical and clinical considerations of a modified protraction headgear. Am J Orthod 1980;78:125-39.
[PUBMED] |
| 5. | Tecco S, Festa F, Tete S, Longhi V, D′Attilio M. Changes in head posture after rapid maxillary expansion in mouth-breathing girls: A controlled study. Angle Orthod 2005;75:171-6.
[PUBMED] |
| 6. | Koudstaal MJ, van der Wal KG, Wolvius EB. Experience with the transpalatal distractor in congenital deformities. Mund Kiefer Gesichtschir 2006;10:331-4.
[PUBMED] |
| 7. | Mommaerts MY. Transpalatal distraction as a method of maxillary expansion. Br J Oral Maxillofac Surg 1999;37:268-72.
[PUBMED] |
| 8. | Wilmes B, Nienkemper M, Drescher D. Application and effectiveness of a mini-implant- and tooth-borne rapid palatal expansion device: The hybrid hyrax. World J Orthod 2010;11:323-30.
[PUBMED] |
| 9. | Ludwig B, Glas B, Bowman SJ, Drescher D, Wilmes B. Miniscrew-supported Class III treatment with the Hybrid RPE Advancer. J Clin Orthod 2010;44:533-9.
[PUBMED] |
| 10. | Halicioglu K, Yavuz I. Comparison of the effects of rapid maxillary expansion caused by treatment with either a memory screw or a Hyrax screw on the dentofacial structures - transversal effects. Eur J Orthod 2011.
|
| 11. | Kim JH, Viana MA, Graber TM, Omerza FF, BeGole EA. The effectiveness of protraction face mask therapy: A meta-analysis. Am J Orthod Dentofacial Orthop 1999;115:675-85.
[PUBMED] |
| 12. | Ludwig B, Glasl B, Bowman SJ, Wilmes B, Kinzinger GS, Lisson JA. Anatomical guidelines for miniscrew insertion: Palatal sites. J Clin Orthod 2011;45:433-41.
[PUBMED] |
| 13. | Wichelhaus A, Geserick M, Ball J. A new nickel titanium rapid maxillary expansion screw. J Clin Orthod 2004;38:677-80.
[PUBMED] |
| 14. | Zimring JF, Isaacson RJ. Forces produced by rapid maxillary expansion. 3. Forces Present during Retention. Angle Orthod 1965;35:178-86.
|
| 15. | Jager A, Braumann B, Kim C, Wahner S. Skeletal and dental effects of maxillary protraction in patients with angle class III malocclusion. A meta-analysis. J Orofac Orthop 2001;62:275-84.
|
| 16. | Kim HJ, Yun HS, Park HD, Kim DH, Park YC. Soft-tissue and cortical-bone thickness at orthodontic implant sites. Am J Orthod Dentofacial Orthop 2006;130:177-82.
[PUBMED] |
| 17. | Kang S, Lee SJ, Ahn SJ, Heo MS, Kim TW. Bone thickness of the palate for orthodontic mini-implant anchorage in adults. Am J Orthod Dentofacial Orthop 2007;131:S74-81.
[PUBMED] |
| 18. | Wiechmann D, Meyer U, Buchter A. Success rate of mini- and micro-implants used for orthodontic anchorage: A prospective clinical study. Clin Oral Implants Res 2007;18:263-7.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
[Table 1]
|












 Search Pubmed for
Search Pubmed for