|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 2 | Page : 105-108 |
|
Treatment of a severe class II div I malocclusion using J-hook headgear
Nishant Negi, Kehar Singh Negi
Department of Orthodontics and Dentofacial Orthopedics, Himachal Pradesh Government Dental College and Hospital, Shimla, Himachal Pradesh, India
| Date of Web Publication | 22-Apr-2014 |
Correspondence Address:
Nishant Negi
Department of Orthodontics and Dentofacial Orthopedics, Himachal Pradesh Government Dental College and Hospital, Shimla - 171 001, Himachal Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.131122

This case report describes 3-year follow-up of orthodontic treatment of a patient with Class II div 1 malocclusion who have 11 mm of overjet and 5 mm of overbite. Extractions of maxillary first and mandibular second premolars were carried out. Maxillary anteriors were retracted using extra-oral force in the form of J-hook headgear. Simple biomechanical principles were utilized for achieving normal occlusion and facial balance. Keywords: Biomechanics, class ii div 1, headgear
How to cite this article:
Negi N, Negi KS. Treatment of a severe class II div I malocclusion using J-hook headgear. J Orthod Res 2014;2:105-8 |
| Introduction | |  |
Class II div 1 malocclusion is a perplexing malocclusion to manage. There are numerous treatment strategies for the management of this malocclusion. [1] Severe cases with a marked maxillary dentoalveolar protrusion pose a dual challenge of prevention of anchorage loss and deepening of bite during retraction. Obtaining an absolute anchorage requires the use of skeletal anchors. [2]
Extra-oral anchorage is a viable alternate, provided patient co-operates to the most full. Retraction of incisors can be accomplished by tipping, bodily movement or a combination of these movements. [3] Often the biomechanics demand control of root apex and controlled tipping of crown. This case report describes 3-year follow-up of the treatment of a Class II div 1 malocclusion with severe maxillary dentoalveolar protrusion by careful application of biomechanical principles.
| Case Report | | |
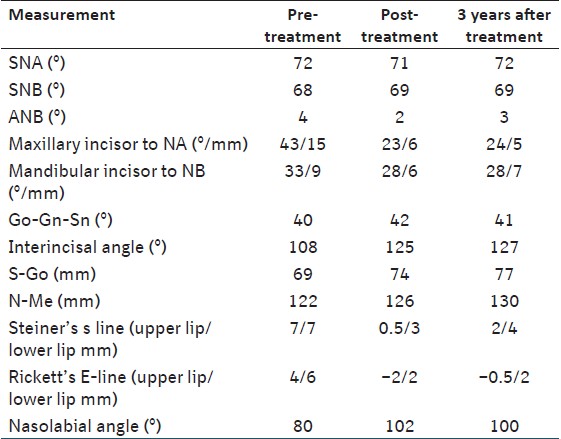
The present case report is about a 12-year-old female patient who reported to our clinic with the complaints of dissatisfaction with her appearance and forwardly positioned upper front teeth. Her pre-treatment records [Figure 1] and [Figure 2] showed a convex profile, short upper lip with incompetence and deep mentolabial sulcus. She had Angle Class II molar and canine relationship with excessive overjet of 11 mm and overbite of 5 mm. There was a mild crowding in the mandibular arch with deep curve of spee. Maxillary arch was narrow and v shaped. Cephalometric analysis showed a skeletal Class I pattern with a high mandibular plane angle, severe maxillary incisor proclination and lip procumbency [Table 1]. Our primary objective was to improve the facial appearance of the patient. The other objectives were to achieve a stable functional occlusion by establishing class I molar and class I canine relationship with normal overjet and overbite.
The maxillary first and mandibular second premolars were extracted. The case was started with standard edgewise prescription (0.022" slot). Initial angulation of maxillary anteriors was corrected using J-hook headgear applied to L-shaped loops in 0.016" ss archwire [Figure 3]a-c. Two step retraction was carried out with the first step involving retraction of canines followed by retraction of incisors. J-hook headgear was used with sliding jigs for canine retraction [Figure 3]d-f. [4] After achieving desired inclination of incisors further retraction was done in 0.019 ss × 0.025 ss archwires [Figure 3]g-i. A force of 100-150 g was applied on each side of headgear which was worn for 14-16 h/day [Figure 3]j. In the mandibular arch closed vertical loops in 0.019 × 0.025" TMA archwire were used for molar protraction. After space closure root paralleling, torquing and artistic positioning was done. Total treatment duration of active treatment was 30 months. After debonding patient was instructed to wear Hawley retainers for 1 year. Patient's profile was improved and a class I molar and canine relationship were achieved. The normal overjet and overbite were also achieved [Figure 4] and [Figure 5].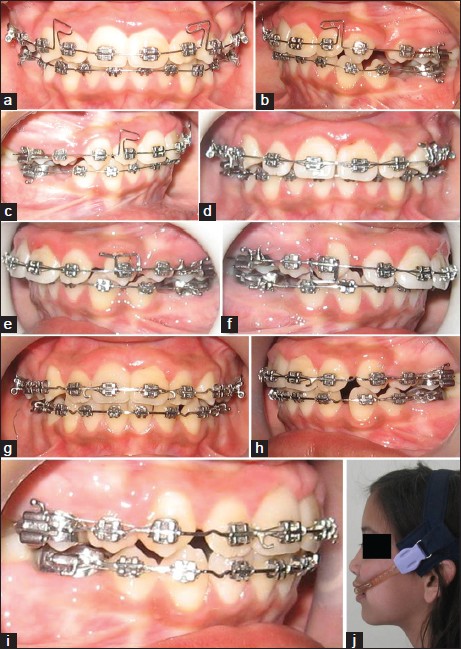 | Figure 3: Treatment progress photographs (a-c) L-shape loops in 0.016 ss wires. (d-f) Cuspid retraction with sliding jigs. (g-i) Final space closure in 0.019 ss × 0.025 ss wire. (j) J-hook headgear combination
Click here to view |
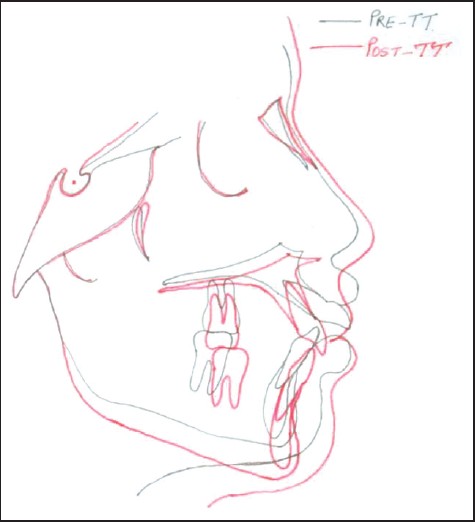
Superimposition on the anterior cranial base (along S-N plane with sella as registration point) revealed overjet correction with controlled tipping of maxillary incisors. Little anchorage loss was observed [Figure 6]. Patient exhibited downward and forward growth during treatment. Post retention stability of the occlusion was observed after 2 years of active treatment [Figure 7] and [Figure 8].
| Discussion | | |
Improving the appearance of the patient was our main objective. As our patient had severe maxillary dentoalveolar protrusion premolar extractions were required for retraction of the anterior teeth as well as for protraction of the molars. With severe maxillary dental protrusion problems are encountered in anchorage control and in maintaining the inclination of maxillary incisors. Surgical concern of patient and additional cost of microimplants excluded the option of skeletal anchorage. Hence we were left with the option of extra-oral anchorage only. Extra-oral anchorage and use of brackets without any tip/torque helped to prevent any strain on maxillary molars. High pull headgear has been proposed for treating patients with high-angle class II div 1 malocclusion. [5] Forces produced by the high pull headgear include both a distal component and an intrusive component. Furthermore, with high pull headgear it is possible to change the direction of force in relation to center of resistance of dental units to achieve better control of tooth movement. [6] Protrusive maxillary incisors which have apex in a good position require controlled tipping to reduce the overjet. Controlling the axial inclination of six anterior teeth is quite difficult. So we retracted the canines first with sliding jigs and high pull headgear. Two step retraction has the disadvantage of increased treatment time and unaesthetic appearance of extraction space but it highly recommended method of space closure in maximum anchorage cases. [7] To achieve controlled tipping, moment/force ratio of 7:1 was required. We planned retraction in 0.016" ss archwire which had sufficient play in 0.022" slot. When upper incisors are severely proclined, retraction is commonly begun by tipping the incisors until normal angulation is reached, at which point bodily movement is attempted. [8] Round wire and high pull headgear combination [Figure 3] created the desired moment/force ratio of 7:1 which allowed the controlled tipping of the incisors. After achieving desired incisor inclination, canines were retracted and the remaining extraction space was closed in 0.019 ss × 0.025 ss archwire to achieve bodily retraction. Mandibular extraction space was closed by protraction of mandibular molars and deep curve of spee was corrected by relative intrusion. This challenging malocclusion was managed without the adverse effects of anchorage loss and bite deepening. Exceptional co-operation from the patient and careful application of bio-mechanics helped us in achieving class I functional occlusion with marked improvement in her profile.
The skeletal anchorage offers a better alternative to headgear, with less anchorage loss and more anterior teeth retraction. [9],[10] In addition, wearing full time headgear is too demanding and many patients reject them for social reasons. However, traditional mechanics still have their role especially when skeletal anchorage is contraindicated due to poor bone volume, density, anatomic limitations etc. There is an additional cost and surgical concern for some patients, which leaves orthodontists with the option of extra-oral forces only.
| References | | |
| 1. | Bell WH, Jacobs JD, Legan HL. Treatment of Class II deep bite by orthodontic and surgical means. Am J Orthod 1984;85:1-20. 
[PUBMED] |
| 2. | Kuroda S, Yamada K, Deguchi T, Kyung HM, Takano-Yamamoto T. Class II malocclusion treated with miniscrew anchorage: Comparison with traditional orthodontic mechanics outcomes. Am J Orthod Dentofacial Orthop 2009;135:302-9.
|
| 3. | Marcotte MR. Prediction of orthodontic tooth movement. Am J Orthod 1976;69:511-23.
[PUBMED] |
| 4. | Tweed CH. Clinical Orthodontics. Saint Louis: C.V. Mosby Company; 1966.
|
| 5. | Firouz M, Zernik J, Nanda R. Dental and orthopedic effects of high-pull headgear in treatment of Class II, division 1 malocclusion. Am J Orthod Dentofacial Orthop 1992;102:197-205.
|
| 6. | Jacobson A. A key to the understanding of extraoral forces. Am J Orthod 1979;75:361-86.
[PUBMED] |
| 7. | Kuhlberg AJ. Steps in orthodontic treatment. In: Bishara SE, editor. Textbook of Orthodontics. Philadelphia, Pa: WB Saunders; 2001. p. 240-2.
|
| 8. | Bennett JC, McLaughlin RP. Overjet reduction with a preadjusted appliance system. J Clin Orthod 1992;26:293-309.
[PUBMED] |
| 9. | Li F, Hu HK, Chen JW, Liu ZP, Li GF, He SS, et al. Comparison of anchorage capacity between implant and headgear during anterior segment retraction. Angle Orthod 2011;81:915-22.
|
| 10. | Zhang N, Bai Y, Li S. Treatment of a Class II Division 1 malocclusion with miniscrew anchorage. Am J Orthod Dentofacial Orthop 2012;141:e85-93.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8]
[Table 1]
|















 Search Pubmed for
Search Pubmed for