|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 3 | Page : 168-172 |
|
Protrusive arch wire using for correction of pseudo class III in early mixed dentition
Maen Mahfouz
Department of Orthodontics and Pediatric Dentistry, Dental School, Arab American University, Jenin, Palestine
| Date of Web Publication | 12-Sep-2014 |
Correspondence Address:
Maen Mahfouz
Department of Orthodontics and Pediatric Dentistry, Dental School, Arab American University, Jenin
Palestine
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.140691

The timing at which orthodontic treatment starts, has always been a debatable matter. Pseudo Class III malocclusion is highly recommended to be treated early as this type of malocclusion worsens by age. If left untreated it may lead to serious problems like abnormal wear of the lower incisors, dental compensation of mandibular incisors leading to thinning of labial alveolar plate and/or gingival recession. There are different methods for solving this problem. The case report describes an effective method which corrects pseudo class III malocclusion in a short time in early mixed dentition by using a protrusive arch wire. Keywords: Early mixed dentition, protrusive arch wire, psuedo class III
How to cite this article:
Mahfouz M. Protrusive arch wire using for correction of pseudo class III in early mixed dentition. J Orthod Res 2014;2:168-72 |
| Introduction | |  |
The correct alignment of teeth is the key to development of a healthy occlusion". [1] Timing of orthodontic treatment especially for children with developing Class III malocclusions, has always been somewhat controversial, and definitive treatment tends to be delayed for severe Class III cases. [2]
The incidence of Class III malocclusion varies and depends upon the different methods of classification used. Class III malocclusion in white subjects occurs in fewer than 1 per cent of the population, while frequency in the Japanese population is approximately 10 per cent. [3]
The diagnosis of pseudo Class III malocclusion differs from that of skeletal Class III malocclusion because it is defined as functional forward displacement of the mandible as a result of retroclined maxillary incisors. [4] Because the major underlying cause of pseudo Class III malocclusion is the inclination of the maxillary incisors, the objective of the treatment is to change the inclination of those incisors.
Pseudo Class III malocclusion has been characterized by an anterior crossbite in the presence of a forward mandibular displacement. [5] The aim of early treatment of this type of malocclusion is to correct Pseudo Class III, as otherwise it can often lead to very serious Class III mallocclusion which would be possible to treat only with combined orthodontic and orthognathic method. [6]
The paper is going to demonstrate quite simple and rapid methods of treatment of pseudo class III malocclusion in early mixed dentition using protrusive arch wire as the modality of treatment.
| Case Report | | |
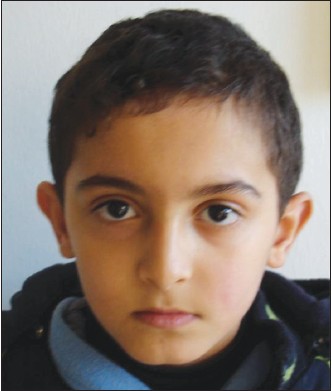
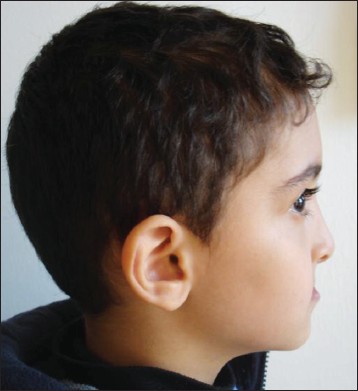
A 7-year-old boy attended my private orthodontic clinic with chief complaint of lower anterior teeth overlapping his upper anterior teeth. He was in early mixed dentition stage. In the extraoral examination the patient profile was straight while lip profile was reversed giving the appearance of class III [Figure 1],[Figure 2] and [Figure 3].
The intraoral examination revealed a forward shift of the mandible, with a marked class III molar relationship and an anterior crossbite [Figure 4],[Figure 5] and [Figure 6].
Diagnosis
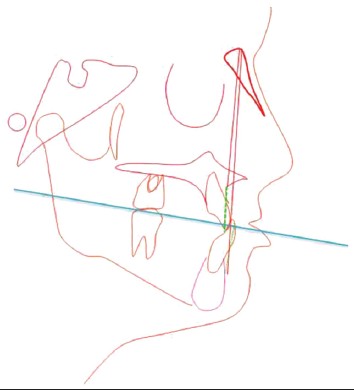
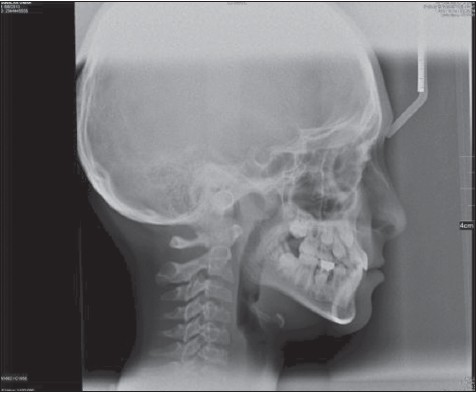
The clinical examination revealed retruded upper lip with protruded lower lip giving the view of deficient mid face as seen in class III. The upper incisors were retruded and spaced while the lower incisors were slightly proclined. An anterior crossbite in the presence of a forward mandibular displacement and functional shift to the left side due to premature contact between upper and lower central incisors was observed leading to diagnosis of Class III malocclusion with reverse overjet and negative deep overbite. The starting point in diagnosis and treatment of this case was by establishing centric relation through guiding the mandible into centric relation rather than centric occlusion and then initial contact with the teeth occurs so an edge to edge anterior incisor contact with posterior open bite indicating pseudo Class III [Figure 3],[Figure 4],[Figure 5],[Figure 6],[Figure 7] and [Figure 8].
Cephalometric analysis indicated a mild Class III malocclusion characterized by a little mandibular protrusion [ANB = −1 degree, Wits = −6 mm, [Figure 7],[Figure 8] and [Figure 9].
Treatment Objectives
Forward movement of 11 maxillary incisors, eliminating functional shift, mandibular displacement, enhancing normal lip profile, achieving class I molar relationship and canine relationship with ideal overjet and overbite.
Treatment Plan
Fixed orthodontic treatment by using protrusive arch wire for the forward movement of 11 maxillary incisors without raising the bite.
Treatment Procedure
Treatment started using bondable tubes placed on the buccal surfaces of upper first permanent molars on both sides with brackets (slot 22) placed on the labial surface of the upper central incisors. Then the placement of upper Niti arch wire rectangular (.016 × .022 inch Protrusive Arch Wire) was customized to the arch form of the patient. A gable bend was made mesial to the bondable tubes on first permanent molars. The exposed part of arch wire was coated with a sleeve to prevent irritation to the cheeks [Figure 10] and [Figure 11].
After carrying out two weeks of orthodontic evaluation of the retroclined upper central incisors, which was orthodontically adjusted, the patient could bite in the present situation due to the Class I canine and molar relationship. The patient presented a normal overbite and overjet and the midlines were coincident. The total treatment time was two weeks and the appliance was removed at the end of the second week [Figure 12] and [Figure 13].
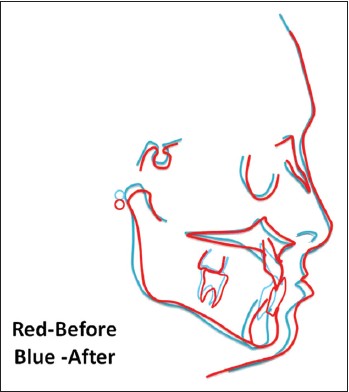
A 2-year follow-up of this case showed good stability of occlusion, function and aesthetics. Final superimpositions showed improvements in ANB and Wits values (+1 degree, −1 mm) respectively. The slight maxillary incisor protrusion coupled with the clockwise mandibular rotation produced an overall improvement of the patient's aesthetic appearance [Figure 14],[Figure 15],[Figure 16],[Figure 17] and [Figure 18],[Figure 19].
| Discussion | | |
There are a variety of treatments suggested in the literature for the correction of Psuedo Class III that includes several different appliances, both fixed and/or removable with heavy intermittent forces (inclined bite-plane, tongue blade) or light-continuous forces (removable appliance with auxiliary springs). [5],[6],[7],[8],[9]
The key to successful management is to remove the anterior interlock as early as possible so as to allow for the normal unrestricted growth of the maxilla and also to guide mandible to a normal position.
The early treatment also permits us to gain space for canine eruption, to enhance positive attitude towards dental treatment, in general, and to improve the aesthetic and functional requirements for development and growth.
In the present case, new treatment modality is demonstrated, which is a simple method for treatment of Pseudo class III in the early mixed dentition.
Protrusive arch wire as a treatment modality needs less compliance in comparison to the removable appliance regarding the wearing of the appliance, especially when dealing with young children. It is similar to 2 × 2 or 2 × 4 fixed utility appliance, which is made up of 0.16 × 0.16 chromium cobalt wire and is settled in bracket 0.018 inch slot without mesial bends and functions to intrude upper anterior teeth. [10] However, it is different cause that is made of 0.16 × 0.22 Niti arch wire and settled in bracket slot 22 with v bend mesial to bondable buccal tubes and functions to procline upper anterior teeth.
Recommendation
This method of pseudo Class III correction in the early mixed dentition, using protrusive arch wire resulted in a positive overjet, proclination of upper incisors and/or retroclination of lower incisors contribute to the correction of anterior crossbite.
| Acknowledgement | | |
To My Family especially my kids, Omar Mahfouz, Noor Mahfouz and Sara Mahfouz.
| References | | |
| 1. | Angle EH. The latest and best in orthodontic mechanisms. Dent Cosmos 1928;70:1143-58. 
|
| 2. | Campbell PH. The dilemma of class III treatment Early or Late?. Angle Orthodontist 1983;53:175-91.
|
| 3. | Nakasima A, Ichinose M, Nakata S. Genetic and environmental factors in the development of so-called pseudo-and true mesioclusions. Am J Orthod Dentofacial Orthop 1986;90:106-16.
[PUBMED] |
| 4. | Hagg U, Tse A, Bendeus M, Rabie AB. A follow-up study of early treatment of pseudo class iii malocclusion. Angle Orthod 2004;74:465-72.
|
| 5. | Jirgensone I, Liepa A, Abeltins A. Anterior crossbite correction in primary and mixed dentition with removable inclined plane (Bruckl appliance). Stomatologija 2008;10:140-4.
|
| 6. | Estreia F, Almerich J, Gascon F. Interceptive correction of anterior crossbite. J Clin Pediatr Dent 1991;15:157-9.
[PUBMED] |
| 7. | Rabie AB, Gu Y. Management of pseudo-Class III malocclusion in southern Chinese children. Br Dent J 1999;186:183-7.
|
| 8. | Giancotti A, Maselli A, Mampieri G, Spanò E. Pseudo-Class III malocclusion treatment with Balters′ Bionator. J Orthod 2003;30:203-15.
|
| 9. | Negi KS, Sharma KR. Treatment of pseudo class III malocclusion by modified Hawley′s appliance with inverted labial bow. J Indian Soc Pedod Prev Dent 2011;29:57-61.
[PUBMED]  |
| 10. | Proffit WR. The first stage of comprehensive treatment: Leveling and Alignment. In: Dalon J, editor. Contemporary Orthodontics. 3 rd ed. St Louis: Mosby; 2007. p. 551-76.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10], [Figure 11], [Figure 12], [Figure 13], [Figure 14], [Figure 15], [Figure 16], [Figure 17], [Figure 18], [Figure 19]
|
























 Search Pubmed for
Search Pubmed for