|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 49-56 |
|
Photographical evaluation of smile esthetics after extraction orthodontic treatment
Veerendra Prasad1, Pradeep Tandon2, Vijay Prakash Sharma2, Gulshan Kumar Singh2, Rana Pratap Maurya3, Vinay Chugh1
1 Department of Plastic Surgery, King George's Medical University (Erstwhile K.G.M.C.), Lucknow, Uttar Pradesh, India
2 Department of Orthodontics and Dentofacial Orthopaedics, King George's Medical University (Erstwhile K.G.M.C.), Lucknow, Uttar Pradesh, India
3 Babu Banarasi Das College of Dental Sciences, Lucknow, Uttar Pradesh, India
| Date of Web Publication | 29-Dec-2014 |
Correspondence Address:
Veerendra Prasad
Department of Plastic Surgery, K.G. Medical University, Lucknow - 226 003, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.147976

Aims: To evaluate and compare the smile esthetics in orthodontically treated subjects and subjects with an esthetically pleasing smile. Materials and Methods: Frontal smiling photographs of 80 subjects in the age group of 18-25 years (mean age of 21.97 years) were taken and divided into Group I (having an esthetically pleasing profile and normal occlusion) and Group II (orthodontically treated). Each Group had 40 subjects, who were further divided into male and female subgroups. Eight transverse and three vertical linear measurements were taken on the frontal photographs and eight ratios were derived. Esthetic scores and other variables were also obtained. The data so obtained were subjected to statistical analysis. Results: All seven ratios did not show any statistically significant differences in both the groups except for ratio 5 (<0.05) in Group IIb. No statistically significant differences were found in the variables of the upper lip curvature, visible marginal gingiva or visible mandibular teeth, except in the visible maxillary first molar (<0.05) for males. The esthetic score showed statistically higher values for males (<0.05) and females (<0.001) in Group I. Lay persons rated significantly higher mean values for esthetic scores in Group Ia (<0.05), Group Ib (<0.001), and Group IIb (<0.01). There were no significant correlations found between the esthetic scores and the seven ratios for both the groups. Conclusion: (1) Females had a more interpremolar/smile width ratio. (2) A greater positive upper lip curvature was found in Group I males and females and was rated higher for esthetic score. (3) The visible maxillary first molar was more in Group II males and females and rated lower for esthetic score. (4) Esthetic scores rated by lay persons were higher for all the subjects. Keywords: Extraction orthodontic treatment, frontal photographs, smile esthetics esthetic score
How to cite this article:
Prasad V, Tandon P, Sharma VP, Singh GK, Maurya RP, Chugh V. Photographical evaluation of smile esthetics after extraction orthodontic treatment. J Orthod Res 2015;3:49-56 |
How to cite this URL:
Prasad V, Tandon P, Sharma VP, Singh GK, Maurya RP, Chugh V. Photographical evaluation of smile esthetics after extraction orthodontic treatment. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:49-56. Available from: http://www.jorthodr.org/text.asp?2015/3/1/49/147976 |
| Introduction | |  |
Smile plays a significant role in facial attractiveness and is one of the most effective means by which people convey their emotions. It influences mating success, kinship opportunities, personality evaluations, performance, and employment prospects, and also influences personality development. Even a well-treated orthodontic case, in which the plaster cast meets every criterion of successful treatment, may not produce an esthetic smile. Stallards [1] thought, beauty being interrelated with the function of the lip and teeth was considered by comparing the smiles of subjects with normal occlusion with the smiles of orthodontically treated subjects.
The face is the most important individual factor determining the physical appearance of people; the mouth and teeth are considered fundamental in facial esthetics. According to Sarver and Ackerman [2] the 'art of a smile' lies in the clinician's ability to recognize the positive elements of beauty in each patient and to create a strategy to enhance the attributes that fall outside the parameters of the prevailing esthetic concept. Johnson and Smith [3] have stated the fact that the appearance of the smile is clearly of substantial clinical importance and often one of the key criteria by which patients judge the success of their own treatment. Hulsey [4] compares the smile of untreated 'Normal occlusion' subjects with subjects who had undergone orthodontic treatment.
According to Ackerman and Ackerman, [5] smile analysis and smile design have become the key elements of orthodontic diagnosis and treatment planning over the last decade. According to Isiksal et al.,[6] an attractive, well-balanced smile is a paramount treatment objective of modern orthodontic therapy. Thus, the purpose of this study was to compare smile esthetics in orthodontically treated subjects (extraction of first premolars) with non-orthodontic subjects having a pleasing smile.
| Materials and Methods | | |
The present study was conducted on frontal smiling photographs of 80 subjects in the age group of 18-25 years with mean age of 21.97 years. The subjects were divided into two groups; Group-I (Control subjects) and Group-II (orthodontically treated subjects). Group-I comprised of 40 non-orthodontic subjects having normal occlusion, a pleasing profile, and an esthetic smile, which were selected after careful examination of 280 students, studying at U.P. King George's University of Dental Sciences, Lucknow. Group-I was further divided into two subgroups; Subgroup-Ia comprising of 20 males and Subgroup-Ib comprising of 20 females. Group-II comprised of 40 subjects, who had undergone orthodontic treatment after extraction of all first premolars with standard edgewise appliances, and had been debonded recently. Group II were also divided into two subgroups, Subgroup-IIa comprising of 20 males and Subgroup-IIb, comprising of 20 females. All the treated subjects were collected from the Department of Orthodontics and Dentofacial Orthopaedics, U.P. King George's University of Dental Sciences, Lucknow.
Selection Criteria for Group - I Sample
- Pleasing faces, normal occlusion, with no obvious facial asymmetry.
- Subjects who had never undergone any orthodontic treatment.
- Subjects with an excessive gingival smile were not included.
Selection Criteria for Group - II Sample
- Pleasing faces, class I molar, and canine relationship, having a normal overjet and overbite after orthodontic treatment
- No obvious facial asymmetry.
- Subjects with an excessive gingival smile were not included.
Method
Standardized frontal photograph of all the subjects were taken during a pleasing natural smile. [3] All photographs were taken by the same investigator at a constant object to lens distance (30 inches) by using a digital camera (DSC W5 Sony) having a 5.1 mega-pixel, 3× optical zoom, and 6× digital zoom Carl Zeiss lens.
Criteria for Standardization of Photographs
- All photographs were taken with a natural head posture and with the interpupillary line parallel to the floor.
- The camera was positioned on a stand at the same distance for each photograph, so that the line of the central lens to the eye was parallel to the horizontal plane and the lens was centered between both eyes.
- Two electronic flashes on the stands were placed at an angle of 45 degrees slightly above the patient, to ensure equal lighting on both sides of the face, to avoid the shadow or darkness on face.
- A clear white background was used for taking photographs in the study.
Five frontal smiling display exposures of the face were taken for each subject and a single 'most pleasing smile' was selected. The selected exposure for each subject was then cropped off to a size of 5 × 3.5 inches using Adobe Photoshop 9.0 version (Adobe system, San Jose, California) and was developed on a Kodak glossy photo paper.
The smile esthetic score was evaluated by a panel of two orthodontists, one plastic surgeon, two general dentists, one cosmetologist, and six lay persons. The panel members were given a smile rating chart and were asked to rate the attractiveness of the smile on the basis of a five-point scale with 5 as excellent, 4 as very good, 3 as good, 2 as fair, and 1 as poor. Each panel member made his/her evaluation separately, without any knowledge of the subject's identity. The scores obtained for each subject were averaged and a mean rating for each smile was determined.
Photographic points used in the study are shown in [Figure 1]. Linear measurements in the transverse and vertical planes are shown in [Figure 2], [Figure 3] and [Figure 4]. [Figure 5] and [Figure 6] showvarious ratios, which are defined by the use of the above photographic points and measurements. [3],[4],[6]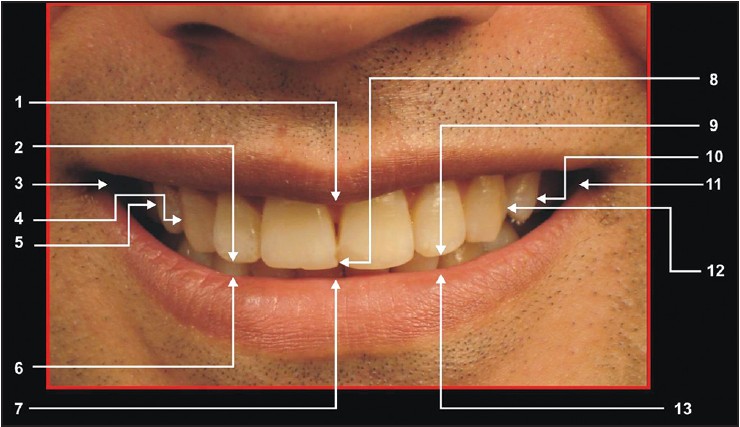 | Figure 1: Photographic points: 1. The most inferior point on the inferior curvature of the upper lip (C Low), 2. Point on the incisal edge of the upper right lateral incisor, where the long axis of the tooth intersects the incisal edge (RL), 3. The innermost corner of the lip on the right side (Rch), 4. Point on the most lateral surface of the upper canine of the right side (RCus), 5. Point on the lateral surface of the upper premolar of the right side (R PM), 6. Point on the upper curvature of the lower lip, directly inferior to point RL (R Lab), 7. The midmost point on the upper curvature of the lower lip, directly inferior to point C (C lab), 8. The midmost and incisal-most point between the incisal edges of the upper central incisors (C), 9. Point on the incisal edge of the left
lateral incisor, where the long axis of the tooth intersects at the incisal edge (LL), 10. Point on the lateral surface of the upper premolar of the left side (L PM), 11. The inner most corner of the lip on the left side (LCh), 12. Point on the most lateral surface of the upper canine on the left side (LCus), 13. Point on the upper curvature of lower lip directly inferior to point LL (L Lab)
Click here to view |
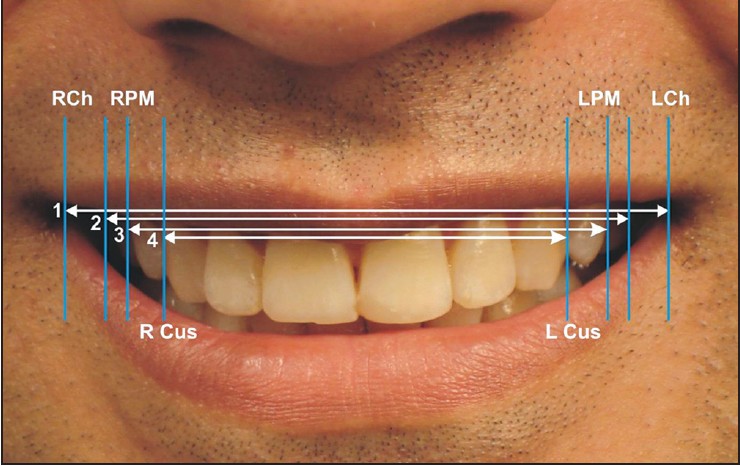 | Figure 2: Linear measurements in transverse plane: 1. Smile width or intercommissure width-Distance between most medial points on the lips at the angle of the mouth (left to right cheilion, RCh to LCh). 2. Visible dentition width-Distance between the most lateral left and right buccal points on maxillary dentition. 3. Interpremolar distance- Distance between the most distal visible points on the fi rst premolar (in case of extraction second premolars) (RPM to LPM). 4. Maxillary intercanine width-Distance between the most distal visible points on the canines (R Cus to L Cus)
Click here to view |
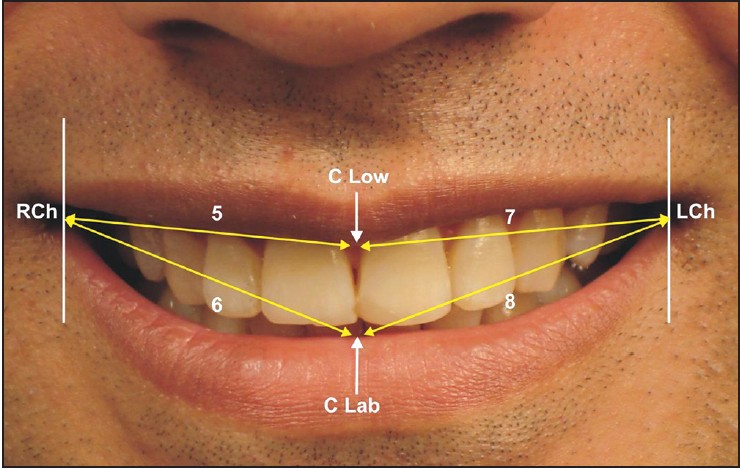 | Figure 3: Linear measurements in the transverse plane: 5. Distance between the innermost corner of the right side of the lip to the most inferior point on the inferior curvature of the upper lip (RCh to CLow), 6. Distance between the innermost corner of the right side of the lip to the midmost point on the upper curvature of the lower lip, directly inferior to point C (RCh to Clab), 7. Distance between the innermost corner of the left side of the lip to the inferior point on the inferior curvature of the upper lip (LCh to CLow), 8. Distance between the innermost corner of the left side of lip to the midmost point on the upper curvature of the lower lip, directly inferior to point C (LCh to Clab)
Click here to view |
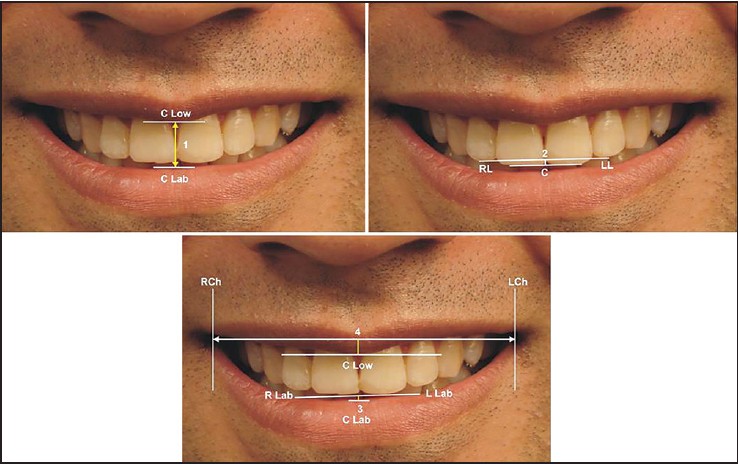 | Figure 4: Linear measurements in the vertical plane: 1. Smile height- Distance from the most inferior point on the upper lip between the maxillary central incisors to the most superior point on the lower lip, on a perpendicular vertical line from the upper point (C Low to C Lab). 2. Length of the perpendicular ofthe arc of the upper incisor- Perpendicular distance from the straight edge through points RL and LL to point C. 3. Length of the perpendicular for the arc of the lower lip-Perpendicular distance from the straight edge through points RLab and LLab to point C Lab. 4. Upper lip curvature (Positive or Negative)-A straight edge was aligned through points RCh and LCh, and point C Low was observed to determine whether or not the point was inferior or superior to the line established determined as positive if the corners of the smile were superior to the center of the upper lip, andnegative if the corners of smiles were below the corner of upper lip
Click here to view |
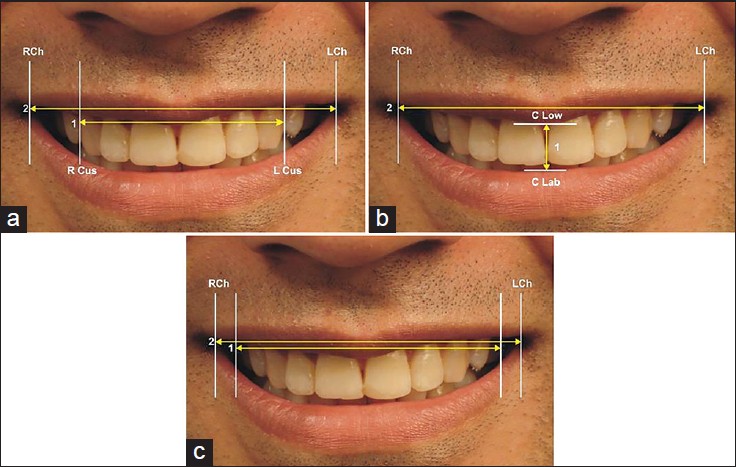 | Figure 5: Various ratios: (a) Ratio 1 (Buccal corridor) = Maxillary intercanine width (1)/Smile width (2); (b) Ratio 2 = Maxillary smile height (1)/Maxillary smile width (2); (c) Ratio 3 = Visible dentition width (1)/Smile width (2)
Click here to view |
 | Figure 6: Various ratios: (d) Ratio 4 = Maxillary intercanine width (1)/ Visible dentition width (2); E. Ratio 5 = Interpremolar distance (1)/ Smile width (2); (f) Ratio 6 (Smile line ratio) = Length of perpendicular for the arc of upper incisors (1)/Length of perpendicular for the arc of lower lip (2); (g) Ratio 7 (Smile symmetry ratio) = Distance from RCh to C Low + Distance from RCh to C Lab (1 + 2)/Distance from LCh to C Low + Distance from LCh to C Lab (3 + 4)
Click here to view |
Although the photographs were taken in a highly standardized manner and all photographs were developed identically, the measurements of the photograph were not as precise as, for example, measurements on cephalometric radiographs. Therefore, the data reported and comparisons between the subjects, for measurements, were limited to the seven mentioned ratios, which were not affected by the difference in magnification between the photographs.
Other variables used in the study were as follows: [3]
- The presence or absence of visible maxillary first molars was classified as: Visible, if any portion of the tooth could be seen during smiling. Each subject was coded as absent = 0 or present = 1.
- Presence or absence of visible mandibular teeth was classified as: Visible, if any tooth could be seen during smiling. Each subject was coded as having a presence = 1 or absence = 0 of any mandibular teeth.
- Presence or absence of any visible maxillary marginal gingiva was classified as: Visible, if seen during smiling. Each subject was coded as having a presence =1 or absence = 0 of any visible marginal gingiva.
Statistics
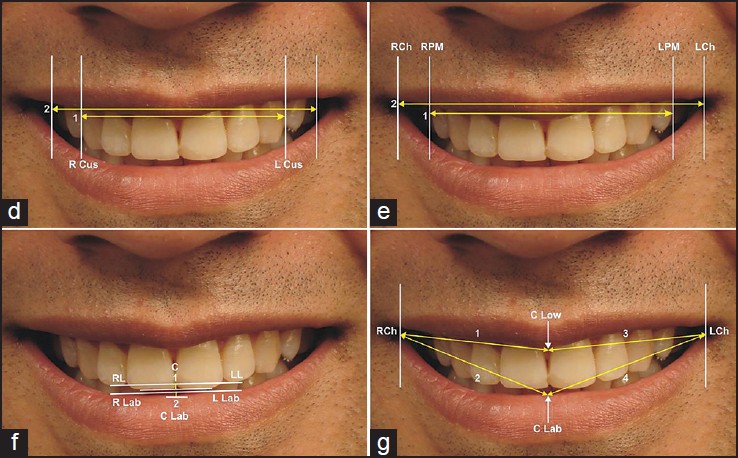
Descriptive data that included the mean and standard deviation were calculated for each group. Karl Pearson's coefficient of correlation was used to measure the degree of linear relationship between two variables and those between groups were compared by using the Student t-test. P < 0.05 was considered to be a statistically significant difference. Reliability of the measurements and the esthetic score were conductedby doing double determinations of 10 photographs, randomly selected, at 15-day intervals, from the collected sample, by the same operator. The comparison was drawn between the first and second determinations by the Student's t-test. There was an insignificant difference between the first and second measurements [Table 1].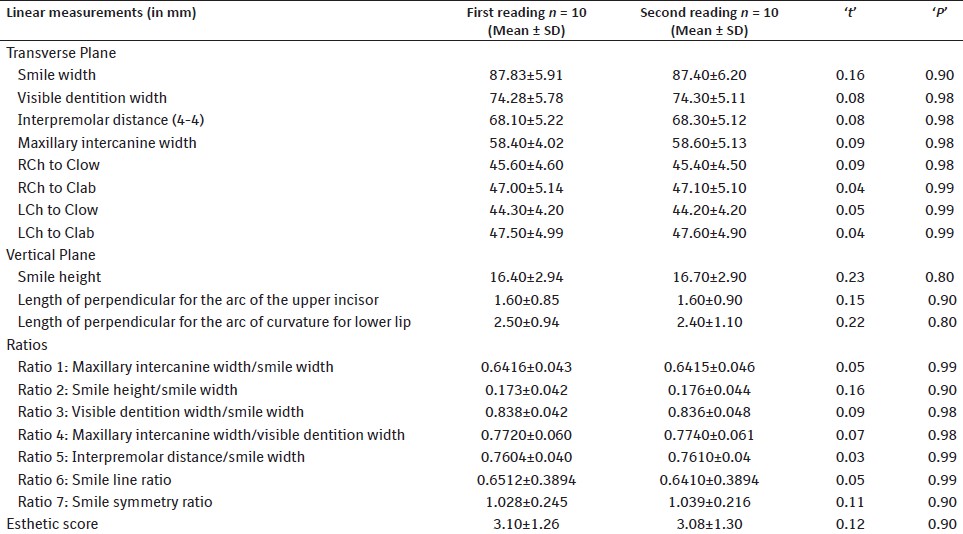 | Table 1: Reliability analysis of photographic variables at two different time intervals
Click here to view |
| Results | | |
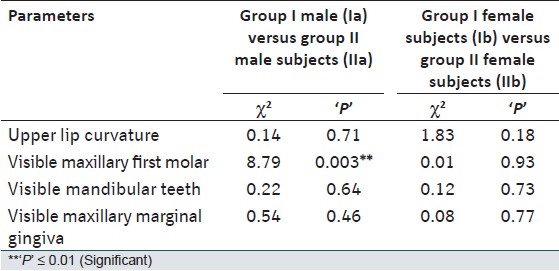
The Mean and SD's of transverse and vertical measurements of males and females in Group I and Group II are shown in [Table 2]. When the mean and SD values of various ratios between Group I and II for both subgroups were compared [Table 3], all seven ratios showed no statistically significant differences for males and females in both the groups, except for ratio 5, which was significantly higher (<0.05) in Group IIb. On intergroup comparison [Table 4] of other variables in males and females no statistically significant differences were found for the variables of upper lip curvature, visible marginal gingival, and visible mandibular teeth. However, the visible maxillary first molar showed a significant difference in males (<0.05), for both the groups. Intergroup and intragroup comparison of the mean and SD values [Table 5] of the esthetic scores showed statistically higher values for both males (<0.05) and females (<0.001) in Group I [Table 6]. Comparison of the means of the esthetic scores rated by professionals and lay persons among various groups and subgroups showed that lay persons rated significantly higher mean values for Group Ia (<0.05), Group Ib (<0.001), and Group IIb (<0.01) [Table 7]. There were no significant correlations found between the esthetic score and the seven ratios, in the males and females of Group I and Group II [Table 8]. | Table 2: The Mean and SD's of linear measurements of males and females in Group I and Group II
Click here to view |
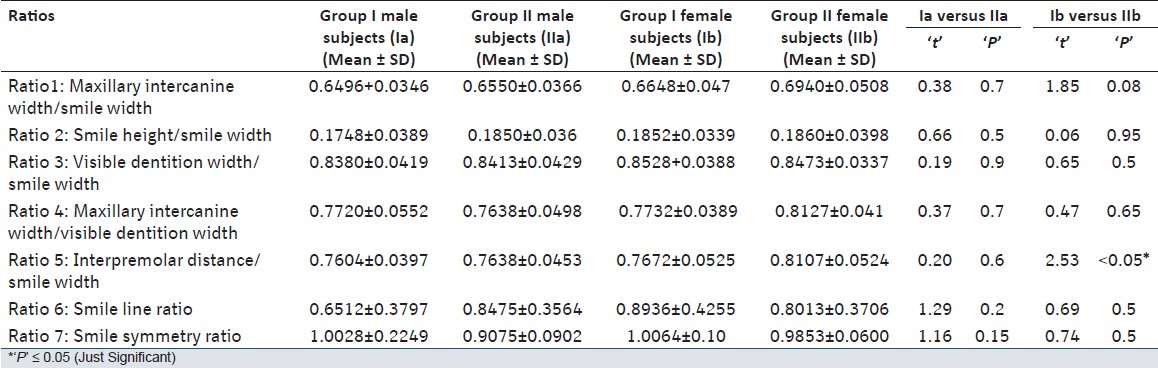 | Table 3: Comparisons of Means and SD's of various measurements of males and females in Group I and Group II
Click here to view |
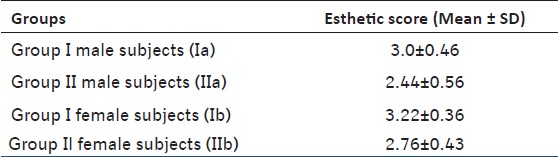 | Table 5: Means and SDs of the esthetic scores of males and females in group I and group II
Click here to view |
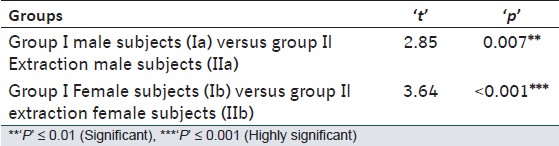 | Table 6: Comparison of the means of esthetic scores among various subgroups
Click here to view |
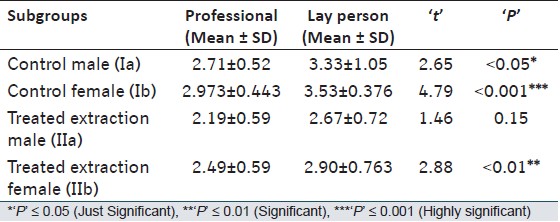 | Table 7: Comparison of means of esthetic scores rated by professionals and lay persons among various subgroups
Click here to view |
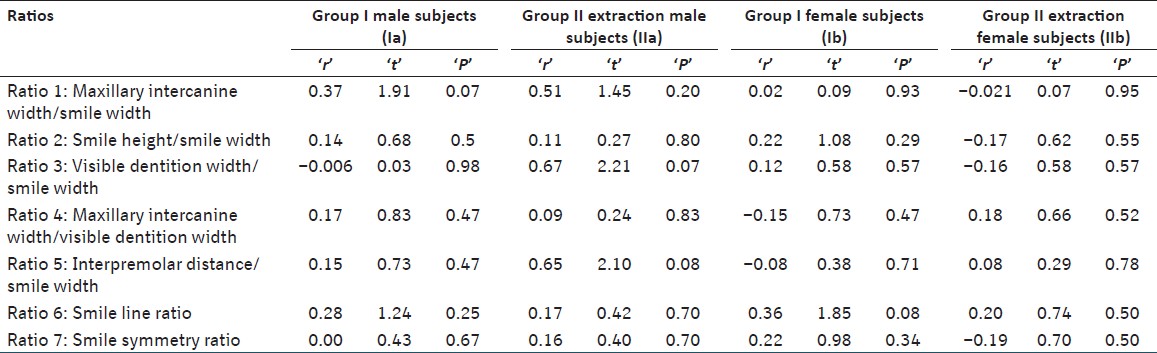 | Table 8: Correlation of esthetic scores with different ratios in control male subjects (Ia), treated extraction male subjects (IIa), control female subjects (Ib) and treated extraction female subjects (IIb)
Click here to view |
| Discussion | | |
Although orthodontic treatment is based primarily on occlusal relationships, greater attention is now paid to enhancing dentofacial characteristics to produce optimal facial esthetics. The major challenge in orthodontics is to establish esthetic excellence and create harmony of the components of the oral region and oral cavity. The orthodontic literature contains more studies on the skeletal structure and profile view than on the soft tissue structure and frontal view of a patient.
According to Isiksal et al., [6] harmony and balance are not fixed concepts. Standards of beauty vary tremendously among persons and racial groups, and also according to the socioeconomic mores. Stallard [1] has considered the smile in tooth positioning, stressing that the line of the upper incisor edge must be parallel to the lip borders and that the upper teeth must hang down evenly in the open smile. Frush and Fisher [7] have directed attention toward the smiling line, the harmony between curvatures of the incisal edges of the upper anterior teeth and upper border of the lower lip.
Poor smile esthetics have become one of the critiques of premolar extraction treatment. It has been suggested that extraction of premolars leads to an unesthetic smile, due to narrowing of the dental arch width and a decreased fullness of the dentition within the mouth during a smile. [8],[9] However, Johnson and Smith [3] have concluded that variables related to the buccal corridor or other measures of relationships between the widths of dentition and of the mouth during a smile showno relationship to the esthetics of a subject after extraction of teeth.
In the present study each group was divided into male and female subgroups, as the qualities of femininity and masculinityare important factors in the interpretation of a smile. [7] Sexual dimorphism was found in the smile line where at maximum smile, the upper-lip line, relative to the gingival margin of the maxillary central incisors, was positioned 1.5.mm more superiorly in females than in males. [10]
Frontal smile photographs were used in the study, because they were much better indicators of transverse dental asymmetry than any other view. [2]
In the present study, when the mean and SD values of various ratios between Group I and II for males and females were compared, it was found that all seven ratios did not show any statistically significant differences for males and females, in both the groups, except for ratio 6, which was significantly higher in Group IIb.
Ratio 1 is a measure of the buccal corridor, which is the space between the facial surfaces of the posterior teeth and the corners of the mouth, when the patient is smiling. Johnson and Smith, [3] in their study, have found that the buccal corridor ratio does not change after extraction treatment, which is similar to our study. Tikku et al. have found that as the buccal corridor space is increased it has rated a loweresthetic score and has mild-to-moderate inverse correlation with the intercanine and intermolar width. [11] E. Isiksal et al.[6] have argued that extraction causes arch-width reduction. [3] Ratio 3 reflects the dental arch fullness in the buccal segments better than Ratio 1. The subjects having a higher ratio 3 show lesser buccal corridor space. This ratio shows a statistically insignificant difference for both the groups and subgroups, in the present study. Similar findings have been reported by Johnson and Smith [3] and Isiksal et al.[6] The findings of our study for ratio 4 are in agreement with the previous studies, [2],[3],[6] which have stated that in adolescents, it is often desirable to increase the arch width with rapid maxillary expansion to create space for non-extraction treatment. Ratio 6 depicts the corresponding harmony between the arcs of curvature for the lower lip and upper incisor teeth. A ratio of 1:0 is defined as the perfect harmony, because the arcs must have equal depth. [4] Ratio 7 is depicted as the symmetry of facial musculature of one side to the other. This ratio is higher for both males and females in Group I, which is supported by the findings of Hulsey. [4]
Intergroup comparison of other variables in males and females, in the present study, showed statistically insignificant differences in distribution of the variables for upper lip curvature, visible marginal gingiva, and visible mandibular teeth. However, the visible maxillary first molar showed a significant difference for males and females in both groups.The upper lip curvature was expressed as positive if the corners of the smiles were superior to the center of the upper lip and as negative if the corners of smiles were below the center of the upper lip. Smiles with the upper lip curving upward were quite attractive, according to the mean smile scores. This fact was also stated by Hulsey. [4] The significant difference for a visible maxillary first molar could be explained on the basis of some mesial migration of molars in extraction cases, leading to their increased visibility. Johnson and Smith [3] found bilaterally visible maxillary first molars in 47% of the extraction patients. There was no evidence that the extraction treatment had a predictable effect on the visible marginal gingiva, although several authors pointed out that detrimental increases in gingival display would frequently occur from orthodontic treatment, with excessive use of intermaxillary Class II elastics. [3] Isikal et al.[6] stated that the upper lip should be at the height of the gingival margin of the maxillary central incisors in an attractive smile. Chinche and Pinault [12] stated that an esthetically ideal amount of visible gingiva was about 1 mm, although 2-3 mm of gingiva might be esthetically acceptable.
Intergroup and intragroup comparison of the esthetic score showed statistically higher mean and SD values for both males and females in Group I. This finding was supported by the study of Hulsey, [4] who reported that the mean smile scores of the normal occlusion subjects were significantly higher.
In the present study, the mean of the esthetic scores in Group Ia and Ib rated by lay persons was significantly higher than that rated by professionals. This finding was supported by previous studies, [3],[13],[14] which found that professionals were sensitized to observe and evaluate the features that did not seem to influence the general public. Orthodontists, on average, were found to be more critical of dental esthetics than lay people, when detecting minor discrepancies. [6]
In present study, there were no significant correlations found between the esthetic score and the seven ratios, in males and females of Group I and Group II. Johnson and Smith [3] found no relationship between the dental arch width/mouth width ratio during smiling and the esthetic score of the patient. Similarly, Gianelly [15] found no differences in arch width between the extraction and non-extraction orthodontic treatment and noted that extraction did not produce a buccal corridor space. When a significant difference at the 0.05 level was found to exist between the smile score with a larger smile line, the smile line ratio got closer to 1.00, or it resulted in perfect harmony between the arc of curvature of the lower lip and the incisal edges of the upper incisor teeth. [4]
This study examined certain characteristics of a smile on full-face frontal smiling photographs. Additional data can be obtained from lateral cephalograms and direct biometric measurements, which demonstrate the amount of lip contraction and amount of vertical lip drape over dentition at rest and when smiling. Digital videography is also useful in dynamic visualization and quantification of a smile.
| Conclusion | | |
The following conclusions were drawn from the present study:
- A significant difference was found for Ratio-5 in Group-I and Group-II females subjects.
- The incidence of positive Upper Lip curvature was found to be higher in both males and females for Group-I subjects and were rated higher for the esthetic score.
- The incidence of the presence of a visible maxillary first molar was higher in both males and females for Group-II subjects. Although, the incidence of the presence of visible mandibular teeth was higher in males of both the Groups.
- Subjects having a higher incidence of excessive visible maxillary marginal gingiva were rated lower in esthetic score.
- The mean esthetic score was rated as lower in Group-II subjects by the panel of judges. The mean esthetic score rated by professionals was found to be lower than those rated by lay persons, for all the subjects.
- No significant correlation was found between the esthetic score and any of the seven ratios.
| References | | |
| 1. | Stallard H. Survival of the periodontium during and after orthodontic treatment. Am J Orthod 1964;50:584-92.  |
| 2. | Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: Part I and II. Evolution of the concept and dynamic records for smile capture. Am J Orthod Dentofaical Orthop 2003;124:4-12. |
| 3. | Johnson DK, Smith RJ. Smile esthetic treatment with and without extraction of four first premolars. Am J Orthod Dentofac Orthop 1995;108:162-7. |
| 4. | Hulsey CM. An esthetic evaluation of lip-teeth relationships present in the smile. Am J Orthod 1970;57:137-44. |
| 5. | Ackerman JL, Ackerman MB, Bresinger CM, Landis JR. A morphometric analysis of the posed smile. Clin Orthod Res 1998;1:2-11. |
| 6. | Iºiksal E, Hazar S, Akyalçin S. Smile esthetics: Perception and comparison of treated and untreated smiles. Am J Orthod Dentofacial Orthop 2006;129:8-16. |
| 7. | Frush JP, Fisher RD. The dynesthetic interpretation of the dentogenic concept. J Pros Dent 1958;8:558-81. |
| 8. | Spahl TJ. Witzing JW. The clinical management of basic maxillofacial orthopedic appliances. Vol. 1. Mechanics. Littleton, Massachusetts: PSG Publishing Co; 1987. |
| 9. | Dierkes JM. The beauty of the face: An orthodontic perspective. J Am Dent Assoc 1987;(Special Issue):89E-95. |
| 10. | Peck S, Peck L, Kataja M. Some vertical lineaments of lip position. Am J Orthod Dentofac Orthop 1992;101:519-24. |
| 11. | Tikku T, Khanna R, Maurya RP, Ahmad N. Role of buccal corridor in smile esthetics and its correlation with underlying dental and skeletal structures. Indian J Dent Res 2012;23: 187-94. [ PUBMED]  |
| 12. | Chin Che GJ. Pinault A. esthetics of anterior fixed prosthodontics. Chicago: Quintessence; 1994. |
| 13. | Kokich V. Kiyak AH. Shapiro PA. Comparing the perception of dentists and laypeople to altered dental esthetics. J Esthet Dent 1999;11:311-24. |
| 14. | Brisman AS. Esthetics: A comparison of dentists and patients concepts. J Am Dent Assoc 1980;100:345-52. |
| 15. | Gianelly AA. Arch width after extraction and nonextraction treatment. Am J Orthod Dentofacial Orthop 2003;123: 25-8. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7], [Table 8]
|










 Search Pubmed for
Search Pubmed for