|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 138-140 |
|
Clinical blackout in orthodontics
Deepak Kumar Gupta1, Ashok K Utreja2
1 Department of Orthodontics and Dentofacial Orthopedics, Dr. Harvansh Singh Judge Institute of Dental Sciences and Hospital, Panjab University, Chandigarh, India
2 Unit of Orthodontics, Oral Health Sciences Centre, Post Graduate Institute of Medical Education and Research, Chandigarh, India
| Date of Web Publication | 15-May-2015 |
Correspondence Address:
Deepak Kumar Gupta
Department of Orthodontics and Dentofacial Orthopedics, Dr. Harvansh Singh Judge Institute of Dental Sciences and Hospital, Sector 25, South Campus, Panjab University, Chandigarh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.149048

Due to increased awareness of the general public in today's world of consumer information the nobility related to the health profession has become a thing of the past. Now-a-day, the patients are consumers, and the malpractice lawsuits are on the rise. There is a strong need to focus our mind and body while working on the patients. Further, there is an urgent need to make the body of literature that can help the common practitioner to see what are the most common error/mistakes, usually, committed and at least avoid those which have been reported. Keywords: Clinical blackout, lawsuit, malpractice, negligence, quack orthodontics, quackery
How to cite this article:
Gupta DK, Utreja AK. Clinical blackout in orthodontics
. J Orthod Res 2015;3:138-40 |
| Introduction | |  |
There has been a growing concern for malpractice and quackery in dentistry [1],[2],[3],[4],[5],[6],[7],[8] as well as in orthodontics in recent times. [9],[10] The malpractice can be defined as a wrong/negligence done by a qualified dentist/orthodontist. It is different from quackery, which is a derogatory term used to describe the promotion of unproven or fraudulent practices, and describes a "quack" as a "fraudulent or ignorant pretender to medical skill" or "a person who pretends, professionally or publicly, to have skill, knowledge, or qualifications he or she does not possess; a charlatan". [11]
However at times we witness such a gross error/negligence that we feel awestruck and really think, how can somebody do it? And why it should not be termed quackery? In these cases, malpractice can often be termed quackery, and when it relates to orthodontics, it could be appropriately called quack orthodontics.
There have been reports of doing such gross act of ignorance/negligence and we as an orthodontists may not have actually read all these instances but we do hear all the funny things in term of gross negligence/error happening in and around as more often than not, especially when few are sitting together for a break, during a conference. We just laugh at funny things being done around us, without realizing that someone amongst us has done that act.
Although it will be difficult to identify, what is a gross error/negligence and one cannot draw a line between a trivial and a gross error. Further the triviality of an error and a gross error will be judged not by the error itself but at what expense it has been to the patient in terms of time, money, discomfort, compromised result etc. The operator will always feel it was a minor and trivial error. Further, the problem of quackery and malpractice is not country-specific, it is a person to person problem meaning thereby that anybody, anywhere in the world can do it irrespective of the nationality of a person. [1],[2],[4],[8]
| Case Report | | |
An 11-year-old boy reported with a chief complaint that despite the fact, he has been wearing braces for more than 15-18 months, there has not been much improvement and thus wanted to change the orthodontist and continue the treatment. A clinical examination revealed that upper and lower arches were banded-bonded with almost complete breakage of lower arch brackets. Everything looked fine in the preliminary examination. Patient carried a pretreatment orthopantomogram (OPG) [Figure 1], which showed that when treatment was started, patient was in mixed dentition period (9-10 years).
Practically, it was easily apparent that the patient was given full banded-bonded appliance at early mixed dentition stage.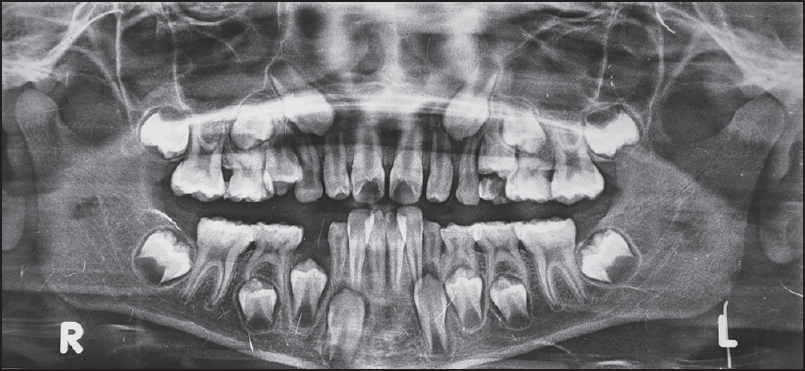 | Figure 1: Pretreatment orthopantomogram showing full eruption of permanent lower first molars
Click here to view |
A close examination revealed that instead of permanent lower first molars, deciduous lower second molars were banded, and treatment had been continuing as such. Further, in the upper arch deciduous canines on both sides were bonded, and left side deciduous canine has even been exfoliated with bracket on it, according to patient past dental history [Figure 2]. | Figure 2: Intraoral photographs showing brackets on deciduous upper right canine and recently exfoliated deciduous upper left canine (which was with bracket according to patient history). Further note the presence
of molars bands on deciduous lower second molars on both sides
Click here to view |
| Discussion | | |
There was no reason to believe that lower deciduous second molars were banded deliberately as the pretreatment OPG [Figure 1] showed full eruption of permanent lower first molars, thereby emphasizing that the clinician delivering the treatment ignored the basic anatomical difference of a permanent and deciduous molar. This ignorance was further emphasized by the fact that patient's maxillary deciduous canines were bonded, giving complete disregard to difference between deciduous and permanent canines. If deciduous canines were bonded intentionally then it is very difficult to comprehend the reason for the same. After clinical examination, patient's OPG [Figure 3] was taken, which confirmed the finding of the clinical examination.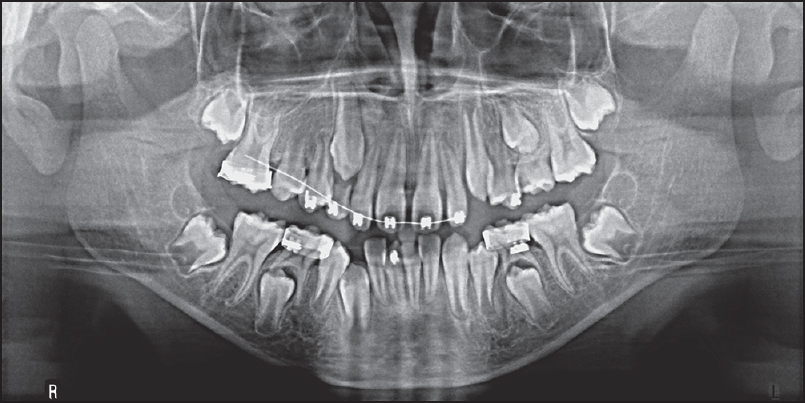 | Figure 3: Orthopantomogram taken on the day of examination which confirmed the clinical fi ndings
Click here to view |
Patient was being treated for the past 15-18 months with this kind of banded-bonded appliance is beyond the comprehension of a prudent orthodontist. What were it, orthodontics or quack orthodontics and who was to be blamed for it? We put this question to the orthodontic fraternity who is responsible for orthodontic care in the country and to Indian Orthodontic Society, who is governing body of orthodontists in India. What kind of care is being given to patients?
Despite best efforts, we failed to know if this person treating the patient was a self-styled orthodontist (dentist who has done short training of orthodontics), or a qualified orthodontist. What was the reason for such gross error, deliberate (to make more money), or there was no comprehension of anatomy of permanent and deciduous teeth, meaning thereby lack of training in undergraduate school, or there was a clinical blackout at that time (while bonding/banding) in his/her mind. To be more conservative, we will select the last, that the clinician's mind stopped working temporarily at that moment (clinical blackout) resulting into gross error. We plan to use the E space in the lower arch for treating crowding of incisors.
| Conclusion | | |
By allowing such cases to be reported, each one of us will be a conscientious orthodontist as well as orthodontic inspector, who will be in a position to monitor someone else's cases if they happen to cross us. The effect will be that each one of us will be more careful in imparting treatment due to the fear of case being reported as clinical blackout, and this may prick their conscience. Basically, the concept of "clinical blackout" works on one of the basic principles of life, that is, "learn from the mistakes of others".
The problem of quackery is a bug, which has bitten every country, developed or developing, but the difference comes with regard to taking concrete steps to tackle it. The magnitude of the problem is large and is, usually, unreported. The need of the hour is to make a concrete data of malpractice and quackery-related cases and use that data in formulating a strong policy to tackle it. Further, the data will act as a ready reference for malpractice and quackery-related cases and alert the prospective clinician to avoid malpractice lawsuits. The orthodontic specialty has always been at the forefront of dentistry and keeping that tradition we should stay upfront in tackling the bug of quackery.
| References | | |
| 1. | Ashkenazi M, Bijaoui E, Blumer S, Gordon M. Common mistakes, negligence and legal offences in paediatric dentistry: A self-report. Eur Arch Paediatr Dent 2011;12:188-94.  |
| 2. | Sandesh N, Mohapatra AK. Street dentistry: Time to tackle quackery. Indian J Dent Res 2009;20:1-2. [ PUBMED]  |
| 3. | Duke ES. New technologies: Quackery or fraud? Compend Contin Educ Dent 2005;26:210, 212. |
| 4. | Naidu RS, Gobin I, Newton JT. Perceptions and use of dental quacks (unqualified dental practitioners) and self rated oral health in Trinidad. Int Dent J 2003; 53:447-54. |
| 5. | Stevenson RB. Quackery, fraud, and denturists. J Am Coll Dent 2003;70:34-7. |
| 6. | Follmar KE. Taking a stand against fraud and quackery in dentistry. J Am Coll Dent 2003;70:4-5. |
| 7. | Schissel MJ, Dodes JE. Holistic dentistry: Innovation or quackery? CDS Rev 1994;87:8-10. |
| 8. | Questionable care: What can be done about dental quackery? J Am Dent Assoc 1987;115:679-85. |
| 9. | Pharande SV, Potnis S, Jamenis S, Jamenis R. Legal concerns for an orthodontist. J Indian Orthod Soc 2012;46:56-7. |
| 10. | Jerrold L. Litigation and legislation. Punitive damages in malpractice lawsuits. Am J Orthod Dentofacial Orthop 2011;139:569-70. |
| 11. | Wikipedia. Search term "Quackery". Available from: http://www.en.wikipedia.org/wiki/Quackery. [Last accessed on 2012 Jun 02]. |
[Figure 1], [Figure 2], [Figure 3]
|










 Related articles
Related articles