|
 
 |
| REVIEW ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 88-91 |
|
A systematic nutritional and dietary guideline for orthodontic patients
Amit Jaikumar Ajmera, Suchita Sadashiv Tarvade, Vishal Ramesh Patni
Department of Orthodontics and Dentofacial Orthopedics, CSMSS Dental College, Aurangabad, Maharashtra, India
| Date of Web Publication | 15-May-2015 |
Correspondence Address:
Amit Jaikumar Ajmera
Plot No. 48, Bhagyanagar, Behind Baba Petrol Pump, Aurangabad - 431 001, Maharashtra
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.150875

A review of the basic principles of nutritional science indicates its applicability to the orthodontics to the many levels. Nutritional considerations are most critical during growth and development and environmental challenges. The orthodontic patients avoid many types of food, particularly fruits, raw vegetables, and other hard and tough foods, as they cannot chew these properly, because of pressure sensitivity of the teeth in the initial 3-5 days period after routine. As a result, such individuals consume significantly less proteins and other key nutrients, fiber, calcium, nonhaem iron, and some vitamins. This paper presents an overview of the relationship between diet and orthodontic treatment. The nutritional guidelines to obtain good oral and general health in orthodontic patients are discussed. Keywords: Fruits, nutrition, orthodontics, vegetables
How to cite this article:
Ajmera AJ, Tarvade SS, Patni VR. A systematic nutritional and dietary guideline for orthodontic patients. J Orthod Res 2015;3:88-91 |
How to cite this URL:
Ajmera AJ, Tarvade SS, Patni VR. A systematic nutritional and dietary guideline for orthodontic patients. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:88-91. Available from: http://www.jorthodr.org/text.asp?2015/3/2/88/150875 |
| Introduction | |  |
In recent years, people have become more aware and concerned about maintaining good health and having a healthy lifestyle. A good diet plays an important role in maintaining good oral and overall health. [1]
A review of the basic principles of nutritional science indicates its applicability to the orthodontics to the many levels. Nutritional considerations are most critical during growth and development and environmental challenges. The literature suggests that the nutritional status of the orthodontic patients can affect the biologic response of the periodontal ligaments and the bone to orthodontic bands and brackets.
Growth and development are affected by nutritional environment. The diet can affect the process of cell replication and enlargement thus influencing tissue and organ growth. Many nutrients affect the enzymatic processes of the body and thus enzymatic regulation is also influenced by diet. [2]
The critical period concept reveals the importance of nutrition in children in allowing the body to attain its full growth and development potential. Oral tissues are no less susceptible to nutritional stresses that may affect a person's oral health and wellness throughout life. [3]
A diet that contains adequate amounts of all the necessary nutrients required for healthy growth and activity is a balanced diet. [4] The importance of a balanced diet cannot be overstated. A balanced diet provides natural disease prevention, weight control, and proper sleep without the use of sleeping pills. Balanced diet is also important because it enables to meet daily nutritional needs and enjoy a higher overall quality of life. [5] With nutritional issues in the spotlight, it seems a good time to evaluate how orthodontic treatment affects a patient's diet.
Orthodontic treatment creates physical, physiologic, and emotional stresses that increase the nutrient mobilization and utilization, thus raising the nutritional requirements of the person. This along with the fact that the nutritional needs of adolescents (the age of a typical orthodontic patient) is already stressed by growth and development as well as the emotional stress of puberty, maintenance of a well-balanced diet is of great importance. [6] Fixed orthodontic treatment typically lasts for around 1½ to 3 years and during this duration certain dietary restrictions and modifications are advised. Here, we discuss about the groups of food that make up a good diet. We also discussed here that how much we need to eat from each group, which food we should eat more or less.
Law of the minimum (formulated by Justus von Liebig 1843). [7]
Among the nutrients essential for growth, the one which is furnished in minimum amount (relative to the need for growth at normal rate) will thereby determine the rate of growth, the organism growing only to extent that it can increase in size. The law of minimum is applicable to proteins but not to minerals since the body may grow to adult size although poor in calcium and other minerals. Children with poor bone structure may still grow to the average or normal size.
Furthermore, the orthodontic patient is in special need of dietary counseling in view of the additional plaque retentive areas provided by the orthodontic appliances.
Furthermore, the patient undergoing orthognathic surgeries present special nutritional considerations. In addition, nutritional imbalances and deficiencies may be involved in the etiology of craniofacial anomalies.
| Effect of Nutritional Status on Tooth Movement and Tissue Response to Appliances | | |
Orthodontic treatment relies on the biologic response of the periodontal ligaments and the alveolar bone to the applied force system.
The orthodontic patient is usually selectively treated during the adolescent growth spurt, which provides an additional challenge to his nutritional status. During growth or healing, some nutrients that are otherwise nonessential become essential for optimal growth.
Other challenges accompanying the adolescent period are increased emotional stress, a higher level of physical activity, and the unbalanced diet that typifies this age group. Ascorbic acid is a classic example of a nutrient that may influence the biologic response to the orthodontic forces. Several studies have documented its effect in orthodontics. The rationale for the effect of ascorbic acid is based on the fact that a lack of it interferes with the collagen synthesis by preventing hydroxylation of proline to hydroxyproline, thus affecting both the periodontal ligament and the formation of osteoid.
If involved in the biologic response to the tooth movement, ascorbic acid may also influence retention.
Nutritional status may also play a role in the gingival response to the orthodontic bands and brackets, especially in regards to increased exposure to retained debris, tissue tolerance need to be maximized. Dusterwinkle et al. [8] banded one mandibular lateral incisor and provided a multivitamin trace mineral supplement or a placebo to this group and to a nonbanded group. After 30 days, the nonbanded group receiving a supplement showed an improved gingival score, decreased tooth mobility, and decreased labial debris. Thus, a nutritional status adequate to support a healthy periodontium in a nonbanded situation may provide suboptimal host resistance in a banded condition.
| Nutrition and Skeletal Maturation | | |
Prolonged nutritive failure in growing children shows a retarding influence on each of the 28 bone centers in the hand and the wrist which are used as indicators of skeletal maturation.
Correction of dietary deficiencies brings the acceleration in the overall rate of skeletal maturation but does not equally affect all the bone centers.
The fastest growing centers generally show the greatest relative response to dietary correction, whereas the slowest growing centers do not demonstrate a preferential utilization of nutrients.
| Dietary Counseling for Plaque Control and General Health in the Orthodontic Patients | | |
The orthodontic patient is subject to a number of challenges that will require a certain host response, which is partially dependent on nutritional status. These stresses include the requirement for tissue response to orthodontic forces in periodontal ligaments and bone. [9],[10]
The increased irritation to the periodontium, the physical and emotional stresses, the increased requirements to the adolescent growth and the often poor quality of the diet during this period. [11],[12]
In addition the use of alcohol or drugs may further increase nutritional requirements. [13],[14] For example, oral contraceptive steroids increase the need for pyridoxine, foliates, and ascorbic acid. [15]
The use of phenytoin by orthodontic patients with epilepsy represents another example of drug-induced vitamin requirement. An anticonvulsant induced osteomalacia with increased osteocytes and osteoclastic resorption was shown to exist in epileptic orthodontic patients and was reversed with Vitamin D therapy.
The increased amount of unmineralized new bone may result in a tendency for increased indirect bone resorption in the patients.
Incremental increase in height and weight as compared with standards are one of the best measures of satisfied nutritional needs, although they are not diagnostic for borderline nutritional states. Thus the orthodontist, who usually uses these data for growth prediction, is able to estimate past nutritional status. [16] In addition, the presence of such orthodontic appliances as bands and brackets should alert the orthodontist to the cariogenicity and poor gingival health due to diet. [17]
Perhaps the best method for patient education is dietary history. Proper instructions on how to keep a dietary history for several days can provide the basis of a brief educational session with the orthodontist or an auxiliary. In addition, a general evaluation of the patient's diet in regard to its balance of nutrients and food groups can be made.
In recent years, people have become more aware and concerned about maintaining good health and having a healthy lifestyle. A good diet plays an important role in maintaining good health. Even the government of different countries has been working to formalize national nutrition monitoring system, and there are new labeling laws for foods regarding fat and salt content.
With so much focus on healthier foods and more nutritional food choices, dietary counseling and nutritional education relevant to oral health have become an important component of dental education. In fact, 1987 guidelines for accreditation of dental schools by American Dental Association require "the graduate must be competent to provide dietary counseling and nutritional education relevant to oral health." [18] Study of diet and nutrition is also a mandatory part of the curriculum in Indian dental schools. [19]
Scientifically, food is divided into five major groups, each group provide some, but not all the nutrients we need. Each food group is as important as another, no one can replace other. For good health, we need them all. Here, we discuss about the groups of food that make up a good diet. We also discussed here that how much we need to eat from each group, which food we should eat more or less.
- Vegetables
- Fruit
- Milk, yogurt, and cheese
- Meat, poultry, fish, dry beans, eggs, nuts, oilseeds, and sweets
- Bread, cereal, rice, and pasta.
This discussion emphasizes that the nutrition is an important factor, influencing the general health and tissue tolerance of orthodontic patients at many levels. While orthodontists will rarely see frank manifestations of nutritional deficiencies, it should be recognized that suboptimal levels of certain nutrients are common and have an effect on the biologic responses of the tissues influenced by orthodontic treatment. 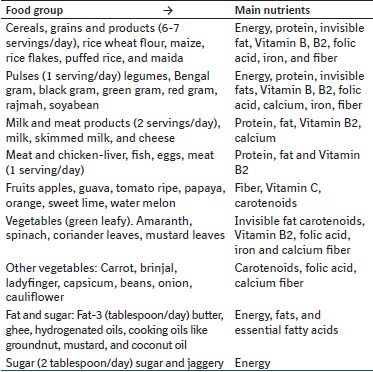
In addition, the age group typically involved in orthodontic treatment has particularly high nutritional demands and particularly poor dietary behavior.
Foods that cannot be cleaned off the braces may lead to discoloration and decay of teeth.
Even though braces and wires are metal or ceramic, they are fragile and are usually damaged by eating the wrong foods, thus taking longer to finish treatment.
Braces friendly eating tips
When you abide by the rules of what to eat and what not to eat when wearing braces, you are doing yourself a favor. Your orthodontist gives you dietary guidelines for a reason. When you are wearing braces, it is important to avoid certain foods that can damage the orthodontic appliances, brackets, and wires, which may cause delays in treatment. The key rule is: Nothing hard, sticky or chewy!
Here is a handy red-yellow and green light list of do's and don'ts when it comes to snacking while wearing braces.
You can also check out our complete list of orthodontic dietary guidelines and more.
Red light (never eat!)
Nuts, Popcorn, Chewing Gum, Hard Pretzels, Pizza Crust, Croutons, Gummy Bears, Caramels, Jelly Beans, Licorice, Jujubes, Chocolate Chips, Ice cubes, Skittles, Starburst, Smarties, M&Ms, Tootsie Rolls, pens and pencils.
Yellow light (use caution, cut up and chew with back teeth)
Nacho Chips, Bagels, Ribs, Chicken Wings, Raw Vegetables, Hard Fruit (i.e., apples, unless sliced thin or cut in small pieces), Fruit with Pits (i.e., peaches), Corn on the Cob, Crusty Bread, Granola Bars, Foods high in sugar (e.g., pop, candy): Don't eat often and brush soon after.
Green light (go for it!)
Ice Cream (no nuts), Potato Chips, Steamed Vegetables, Pasta Potatoes, French Fries, Soft Pretzels, Yogurt, Pudding, Jelly, Soup, Sub Sandwiches, Cereal in Milk, Cheese, Eggs, Milkshakes, Caramel Bars, Peanut Butter Cups.
| Conclusion | | |
To optimize patient's physiologic response to orthodontic treatment, it may be beneficial to provide dietary guidance to orthodontic patients in choosing soft food diets. This includes obtaining nutrition history, evaluating the diet, educating the patient about diet components important for oral health, motivating the patient to improve diet, and follow-up to support patient's effort to change food behaviors.
Patient with braces who prefer or switchover to convenience foods such as cakes, pastries, ice creams, and cookies, which are high in simple sugars and fats, should be advised regarding the value of fruits, vegetables, grains, and cereals in the irregular diet. Nutrition goals for the orthodontic patient should be to eat a variety of foods including protein sources, dairy food, fruits, vegetables, and cereals and to limit salt, fat, and sugar intake.
| References | | |
| 1. | Romite LM. Nutrition and oral health. Dent Clin North Am 2003;47:187-207.  |
| 2. | Southon S, Wright AJ, Finglas PM, Bailey AL, Belsten JL. Micronutrient intake and psychological performance of schoolchildren: Consideration of the value of calculated nutrient intakes for the assessment of micronutrient status in children. Proc Nutr Soc 1992;51:315-24. |
| 3. | Connolly KJ, Kvalsvig JD. Infection, nutrition and cognitive performance in children. Parasitology 1993;107 Suppl:S187-200. |
| 4. | Yetley EA, Beloian AM, Lewis CJ. Dietary methodologies for food and nutrition monitoring. Vital Health Stat 4 1992;58-67. |
| 5. | Luke B. Principles of Nutrition and Diet Therapy. Little, Brown and Company, 1984; p. 3, 816. |
| 6. | Hickory W, Nanda R. Nutritional considerations in orthodontics. Dent Clin North Am 1981;25:195-201. [ PUBMED] |
| 7. | Von J. Liebig and after Liebig. Liebig and the Law of the Minimum, a Century of Progress in Agricultural Chemistry. Lancaster, PA: The Science Press Printing Co., American Association for the Advancement of Science; 1843. |
| 8. | Dusterwinkle SA, Cheraskin E, Ringsdorf WM Jr, Setyaadmadja AT. Tissue tolerance to orthodontic banding: A study in multivitamin-trace mineral supplementation. J Periodontol 1966;37:132-45. [ PUBMED] |
| 9. | Bakdash MB, Zaki HA. The impact of diet and nutrition on periodontal health. Northwest Dent 1978;57:5-14. [ PUBMED] |
| 10. | Ferguson HW, Alfano MC. Controversies, perspectives, and clinical implications of nutrition in periodontal disease. Dent Clin North Am 1976;20:519-48. |
| 11. | Neiva RF, Steigenga J, Al-Shammari KF, Wang HL. Effect of nutrition on the periodontium. In: Biology of the Periodontium. London: Academic Press; 1969. p. 422-51. |
| 12. | Egelberg J. Local effect of diet on plaque formation and development of gingivitis in dogs. I. Effect of hard and soft diets. Odontol Revy 1965;16:31-41. |
| 13. | Cheraskin E, Ringsdorf WM Jr. Biology of the orthodontic patient. I. Plasma ascorbic acid levels. Angle Orthod 1969;39:137-8. |
| 14. | Cheraskin E, Ringdorf WM Jr. Biology of the orthodontic patient. II. Lingual vitamin C test scores. Angle Orthod 1969;39:324-5. |
| 15. | Litton SF. Orthodontic tooth movement during an ascorbic acid deficiency. Am J Orthod 1974;65:290-302. [ PUBMED] |
| 16. | Morhart RE, Fitzgerald RJ. Nutritional determinants of the ecology of the oral flora. Dent Clin North Am 1976;20:473-89. [ PUBMED] |
| 17. | Gustafsson BE, Quensel CE, Lanke LS, Lundqvist C, Grahnen H, Bonow BE, et al. The Vipeholm dental caries studies: The different levels of carbohydrate intake on caries activity in 436 individuals observed for five years. Acta Odontol Scand 1954;11:232-364. |
| 18. | American Dental Association. Procedures for Evaluation Requirements and Guidelines for Dental Education Programs. Chicago: American Dental Association; 1987. |
| 19. | Prevention of Food Adulteration (5 th Amendment) Rules, 2008. Ministry of Health and Family Welfare (Department of Health and Family Welfare) Notification. New Delhi, the 19 th September, 2008. |
|










 Search Pubmed for
Search Pubmed for