|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 192-198 |
|
Bimaxillary protrusion in a Sudanese sample: A cephalometric study of skeletal, dental and soft-tissue features and treatment considerations
Salma Babiker Idris Elhag, Shaza Kamal Abbas, Eman Salama Ibrahim, Hayder Abdallah Hashim, Abdallah Abdulhafiz Sharfy
Department of Orthodontics, University of Khartoum, Khartoum, Sudan
| Date of Web Publication | 11-Sep-2015 |
Correspondence Address:
Salma Babiker Idris Elhag
Department of Orthodontics, University of Khartoum, Khartoum
Sudan
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.158136

Introduction: Bimaxillary protrusion (BP) is a condition that results in the convexity of the face and lip incompetence. There are two forms of BP, a dentoalveolar type and a skeletal type each requiring a different treatment plan. Aims: The aims of this study were to cephalometrically determine the skeletal, dental and soft-tissue features of a sample of Sudanese adults with BP to establish the origin, growth pattern, and presence of gender dimorphism. Design: Descriptive, retrospective study. Setting: Orthodontic Clinics in University of Khartoum, Khartoum Dental Teaching Hospital and University of Science and Technology. Materials and Methods: Pretreatment lateral cephalometric radiographs of 60 patients (30 males and 30 females) with BP (mean age 25.4 ± 6 years) were collected and manually traced. Twenty-two variables were assessed and compared to Sudanese norms (n = 73) which included (35 males and 38 females) of similar age (22.5 ± 3 years) using Student t-test and one sample t-test. Results: The sample revealed significantly smaller SNA, SNB angles and increased incisor protrusion and lip thickness than Sudanese norms (P < 0.05). However, the sample showed significantly higher SNMP, MMPA, upper facial height (UFH), lower facial height, FP% (P < 0.05). Only five gender differences were demonstrated; UFH, U1L1, LlNB mm, LlNB (°), and lower lip length. Conclusion: It can be concluded that facial convexity in Sudanese patients with class 1 molars is a result of bimaxillary dentoalveolar protrusion and increased lip thickness. The patients also revealed a vertical growth pattern with males and females demonstrating similar cephalometric profiles. Treatment of such patient entails extraction of all first premolars with maximum anchorage. Keywords: Adults, bimaxillary proclination, bimaxillary protrusion, cephalometrics, Sudanese
How to cite this article:
Elhag SB, Abbas SK, Ibrahim ES, Hashim HA, Sharfy AA. Bimaxillary protrusion in a Sudanese sample: A cephalometric study of skeletal, dental and soft-tissue features and treatment considerations. J Orthod Res 2015;3:192-8 |
How to cite this URL:
Elhag SB, Abbas SK, Ibrahim ES, Hashim HA, Sharfy AA. Bimaxillary protrusion in a Sudanese sample: A cephalometric study of skeletal, dental and soft-tissue features and treatment considerations. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:192-8. Available from: http://www.jorthodr.org/text.asp?2015/3/3/192/158136 |
| Introduction | |  |
The main objective of orthodontic treatment is to improve facial esthetics and functional occlusion. [1] Orthodontists have a tendency to emphasize on the profile when planning treatment because most dental treatment problems relate to anteroposterior treatment goals particularly the correction of class II or III malocclusion. [2] Facial convexity can be found in patients with skeletal class II discrepancy or in patients with normal skeletal relationships but have bimaxillary skeletal or dentoalveolar protrusion (Bimaxillary protrusion [BP]). [3]
On reviewing the literature, differences in the skeletal sagittal and vertical relationships of various ethnic and racial groups were found. Some ethnic groups with BP were found to demonstrate a vertical facial growth pattern whereas others did not. Bills et al. [4] found a vertical facial pattern in their BP sample of multiethnic background. This is in contrast to a study conducted by Dandajena and Nanda [5] on Zimbabwean subjects, where it was revealed that bialveolar protruded individuals showed a reduced Frankfort mandibular plane angle, indicating a horizontal growth pattern. Furthermore, Aldrees and Shamlan [6] observed that Saudi individuals with BP had a normal vertical skeletal pattern.
Regarding the dental aspects of BP, the increased incisor proclination results in reduction of the interincisal angle. Lamberton and Reichart [7] in a study done in Thai subjects with bimaxillary dental protrusion concluded that the bimaxillary dental protrusion was considered to be present if the interincisal angle was below 124°. The increased proclination of the lower incisor specifically contributes to the BP. Kowalski et al. [8] compared black and white individuals and concluded that the single most effective discriminator to be the lower incisor to NB distance. The proclination of the lower incisor was much higher in black subjects.
The soft-tissue features of BP show differences among male and female subjects and between blacks and whites. de Freitas et al. [9] observed soft-tissue protrusion in black Brazilian subjects compared to white Brazilian subjects. The upper and lower lips were shown to be more protruded in blacks, but lip thickness was similar in both groups. Aldrees and Shamlan [6] found that Saudi individuals with BP demonstrated increased procumbency of the upper and lower lips. Males with BP were found to have increased lower lip thickness compared to the females in the Saudi sample.
The population of Sudan is a combination of indigenous inhabitants of the Nile Valley and descendants of migrants from the Arabian Peninsula. Due to the process of Arabization, which is common throughout the rest of the Arab world, today Arab culture predominates in Sudan. [10] Skeletal and dental cephalometric norms for the Sudanese with well-balanced faces were established in a previous study, in which distinctive features of this population were revealed. [11] Skeletally, the maxilla and mandible were more prognathic compared to the maxillae and mandibles of the Caucasians and Arabs but less prognathic than that of the Africans. Dentally, the maxillary and mandibular incisors were more proclined than those of the Arabs and Caucasians but less proclined when compared to the Africans. The soft-tissue profile norms of the Sudanese in another study showed more facial convexity and lip protrusion compared to Caucasians and Arabs but less than Africans. [12]
Bimaxillary protrusion is one of the most common malocclusions seen by orthodontists in Sudan. Despite that no published data exist describing its features in the Sudanese population. The intentions of the present study were to cephalometrically determine the skeletal, dental and soft-tissue features of a sample of Sudanese adults with BP to establish the origin, growth pattern and to conclude the presence of gender dimorphism. Also to compare the results with previously published Saudi and Zimbabwean values.
| Materials and Methods | | |
This study included patients who attended the Orthodontic Clinics at the University of Khartoum, Khartoum Dental Teaching Hospital and the University of Science and Technology from the period of 2008 to 2012.
The records were scanned for patients diagnosed with BP according to the following inclusion criteria; natural born ethnic Sudanese, minimum pretreatment age of 15 years for females and 18 years for males, facial convexity, lip prominence, lip incompetence, Angle class 1 molar relationship on both sides, good quality films that have no distortions or soft-tissue cut out, no history of previous orthodontic or prosthodontic treatment, no history of maxillofacial or plastic surgery, no congenital facial anomalies and no history of systemic diseases or chronic illness that may affect the normal dentofacial growth.
As a result, a total of 60 Sudanese adults (30 males and 30 females) with a mean age of 25.4 ± 6 years were included in the present study. The BP sample was compared to established Sudanese norms [11],[12] (n = 73) which included (35 males and 38 females) with similar age (22.5 ± 3 years). Permission was taken from concerned administration, and a signed consent form approved by Ethical Committee at the University of Khartoum, Faculty of Dentistry was obtained.
All cephalographs obtained had lips in a rest position and teeth in centric occlusion. The lateral cephalometric radiographs were hand traced on acetate paper by the same investigator (Elhag S) in a dark room using an illuminator box and 0.5 mm sharp pencil. Twenty-two landmarks were measured according to the definitions of Caufield, [13] Viteporn, and Athanasiou. [14] [Figure 1],[Figure 2] and [Figure 3] show the measurements carried out in this study.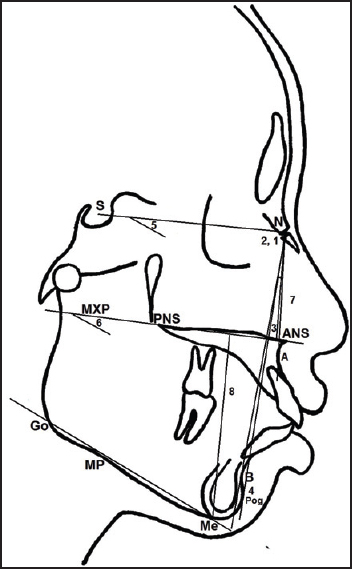 | Figure 1: Skeletal variables: (1) SNA, (2) SNB, (3) ANB, (4) SNPog, (5) SNMP, (6) MMPA, (7) upper facial height, (8) lower facial height
Click here to view |
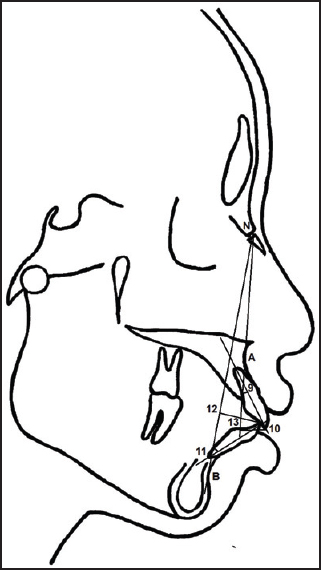 | Figure 2: Dental variables: (9) U1NA (°), (10) U1NA (mm), (11) L1-NB (°), (12) L1NB (mm), (13) Ul-Ll
Click here to view |
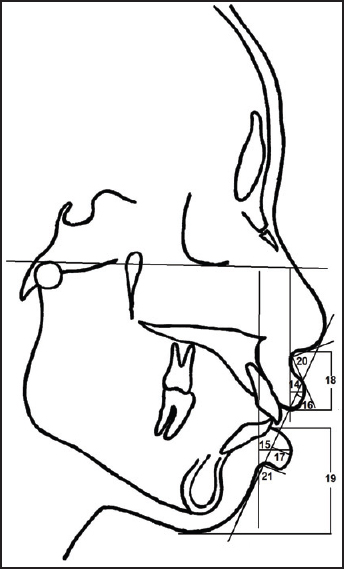 | Figure 3: Soft-tissue variables: (14) ULTH, (15) LLTH, (16) UL-E, (17) LL-E, (18) upper lip length, (19) lower lip length, (20) nasolabial angle, (21) mentolabial angle
Click here to view |
Statistical analysis
All statistical analyses were performed with SPSS® (Statistical Package for Social Science) program (version 16.0, Chicago, IL, USA). For each variable, the arithmetic mean and standard deviation were calculated. A one sample t-test was used to compare the mean results of the BP sample with Sudanese norms and compare males and females with BP with male and female norms. A paired sample t-test was utilized to compare males and females with BP. The level of significance was set at P < 0.05.
| Results | | |
[Table 1] shows significant differences in most of the skeletal, dental and soft-tissue variables of the BP sample compared to established Sudanese norms at (P < 0.05).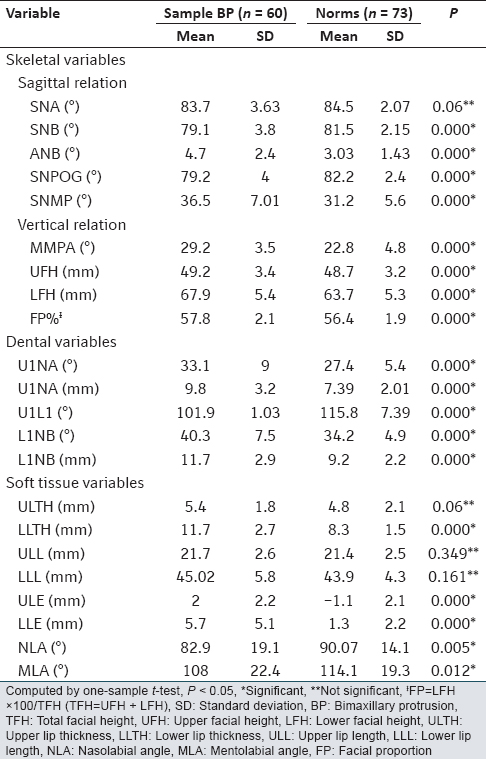 | Table 1: The mean and SD of cephalometric measurements in a Sudanese sample with BP compared with Sudanese norms
Click here to view |
[Table 2] reveals significant differences between males with BP and male norms in the majority of variables except the upper facial height (UFH), FP, ULTH, upper lip length (ULL), lower lip length (LLL), and mentolabial angle (P < 0.05) In the skeletal sagittal relationship, males with BP showed significantly reduced values compared to the male norms. The ANB angle of (4.1°) was significantly increased (P = 0.032) but within normal limits. The vertical measurements were significantly increased in the males with BP with exception to the UFH, which was similar in both groups. All dental variables were significantly protruded in males with BP. They also demonstrated significantly increased ULE, LLE, LLTH, and reduced nasolabial angle (P < 0.05).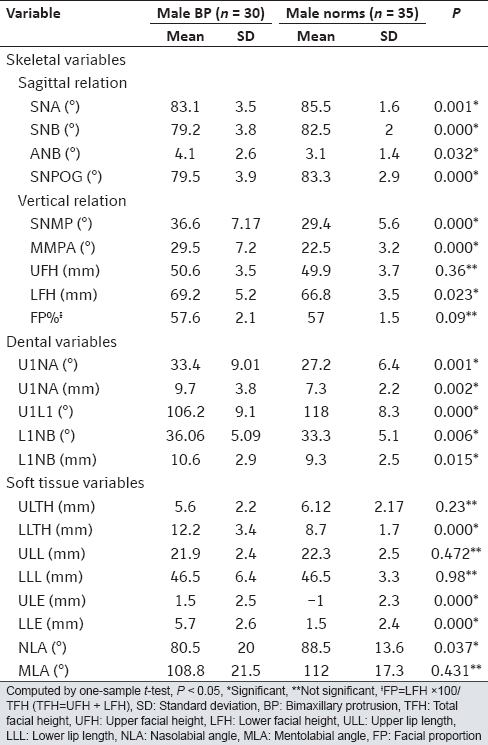 | Table 2: The mean and SD of males with BP compared with male Sudanese norms
Click here to view |
[Table 3] shows that females with BP demonstrated significant differences in most of the variables measured except the SNA, UFH, and ULL compared to female norms (P < 0.05).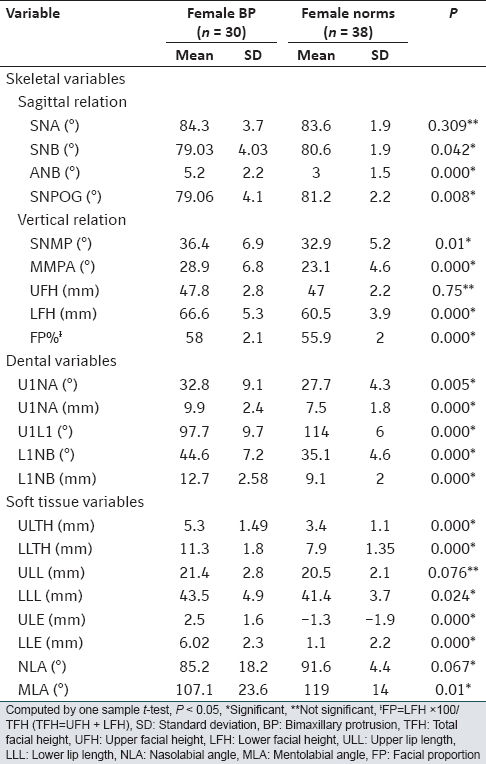 | Table 3: The mean and SD of females with BP compared with female Sudanese norms
Click here to view |
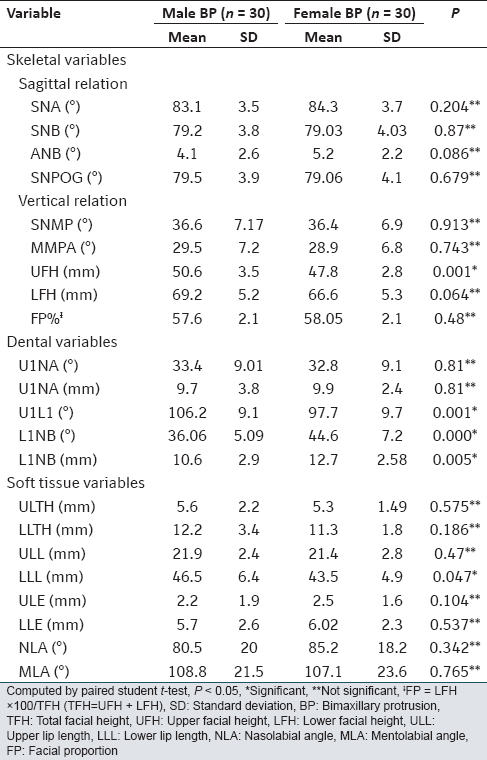
[Table 4] evaluates the existence of gender dimorphism. Only five gender differences out of the 22 variables measured showed statistical significance. These were the; UFH, L1NB (°), L1NB mm, U1L1, and LLL (P < 0.05). Males were found to have significantly increased UFH (P = 0.001) and LLL (P = 0.047) whereas females revealed significantly reduced interincisal angle (P = 0.001) and significantly increased lower incisor protrusion and proclination.
| Discussion | | |
Patients with BP have relatively more convex faces due to a more anterior position of skeletal, dental and soft-tissue structures in the mid-face region. [15] This study can be regarded as the first to study BP in a Sudanese sample revealing unique skeletal, dental and soft-tissue features.
Skeletal measurements
Bimaxillary skeletal protrusion is present when both the maxilla and mandible are prognathic. [2] The results of the present study showed that neither the maxilla nor the mandible was prognathic in the Sudanese adults with BP features. In actual fact, the maxilla of the BP sample was normal with an SNA angle of (83.7° ± 3.4°). On the other hand, the mandible was retrognathic with an SNB angle of (79.1° ± 3.8°), and this excluded the presence of bimaxillary skeletal protrusion in this sample. These findings were in agreement with that found in Indians. [16] The Sudanese with BP were found to have a higher SNA angle compared to Saudis [6] with BP whereas the SNB was comparable between them. The Zimbabweans [5] however, exhibited higher SNA and SNB values whereas the Caucasians [15] with BP revealed lesser values.
Several authors, including Jacobson [17] showed that the magnitude of the ANB angle was affected by four factors: The degree of protrusion of upper and lower jaws, rotation of the jaws, lower anterior facial height, anterior-posterior position of Nasion. In the present study, there was a slight increase in the ANB angle giving rise to a mild skeletal class II pattern. This may be attributed to the downward and backward rotation of the mandible which increases the ANB angle. This finding was consistent with the findings of Keating [15] on a Caucasian sample. Dandajena and Nanda [5] had also revealed an increased ANB angle in the Zimbabwean sample, but they attributed that to the mismatch of a small SNB angle compared to a larger SNA angle. Since a mild skeletal class II was detected in the Sudanese sample, these patients are ideal candidates for camouflage treatment. [3]
The present study also showed significantly recessive chins compared to Sudanese established norms. [11] This could be related to the vertical and backward rotation of the mandible indicated by the increased MMPA, SNMP, lower facial height (LFH), and FP leading to a vertical growth pattern and a hyperdivergent facial pattern. The results of the present study were in agreement with the findings of Bills et al. [4] where they found a vertical growth pattern and increased LFH in their sample. The results were also similar to the findings of Keating [15] on a Caucasian sample. However, these findings were in contrast to the horizontal type of growth pattern that was detected in Zimbabweans [5] and Moroccans [18] and also to the normal vertical growth pattern revealed by Aldrees and Shamlan [6] on Saudis.
The vertical growth pattern observed in the present study has significant clinical implications because orthodontic mechanotherapy tends to be extrusive in nature which will further rotate the mandible downward and backward. Therefore, the extrusive components of the mechanical system should be carefully controlled particularly in nongrowing patients. [3]
Dental measurements
It has been reported that blacks tend to have flared upper and lower incisors, [19],[20],[21],[22] these findings were also observed in the present study. The upper and lower incisors were significantly proclined and in a more forward position compared to Sudanese norms. The BP Sudanese sample had more proclined and protruded upper and lower incisors than Caucasians, [15] Moroccans, [18] Palestinians, [23] and Zimbabweans. [5] On the other hand, only the Saudis [6] had similar upper incisor protrusion. The interincisal angle of the Sudanese sample (101.9°) was found to be less than that reported for African Americans, [22] Nubians, [24] and Thais. [7]
Significant differences in the dental relationship between males and females were found only in the lower incisors proclination and protrusion. Females in the present study tended to have more proclined and protruded lower incisors. This may attribute to the significantly reduced interincisal angle in the females. These results were similar to that observed by Hussein and Abu Mois [23] where he noted that Palestinian females show more lower incisor proclination leading to a more reduced interincisal angle.
According to the Royal London space planning, [25] a space of 1 mm is needed when changing the inclination of the upper maxillary incisors 5°. In addition, every 1 mm of incisor retraction requires a space of 2 mm when bodily retracting the incisors anterior-posteriorly. The Sudanese sample showed increased incisor proclination and protrusion by 6° and 3 mm, respectively. The overall space requirement of about 7 mm can easily be obtained by extraction of first premolars. Maximum anchorage is required in these cases to prevent loss of the extraction space since space loss occurs readily in patients with increased facial heights owing to weaker facial muscles. [26]
Soft-tissue measurements
Soft-tissue evaluation for the whole sample revealed increased thickness of the lower lips in the BP sample compared to Sudanese norms. However, there was no significant difference in the lip thickness between Sudanese males and females with BP.
The current study found an increased protrusion of the upper and lower lips where both lips were anterior to Rickett's E line. This was in agreement with the findings of Bills et al. [4] and with the findings of Aldrees and Shamlan [6] who assessed lip protrusion with a different measurement on Saudis with BP. The results of the present study conflicted with that obtained by Hussein and Abu Mois [23] for the Palestinian sample where there was no lip protrusion despite the presence of incisor proclination. The increased lip protrusion in both males and females revealed in the present study may be attributed to the increased incisor proclination and increased lip thickness.
The present study also revealed that males with BP had significantly increased LLL compared to the females. A reduced nasiolabial and mentolabial angles were observed in this sample which were similar in both genders. Lack of a well-defined mentolabial sulcus can be due to an increased LFH, protrusion of the teeth and a recessive chin. [3] All these factors were found in this study.
In summary, facial convexity in Sudanese patients with class 1 molars was a consequence of bimaxillary dentoalveolar protrusion and increased lip thickness. These patients also exhibited an increased vertical growth pattern. Males and females revealed similar cephalometric profiles except that males showed increased UFH and LLL whereas females demonstrated increased lower incisor proclination and protrusion. Based on these findings, the treatment of BP in Sudanese patients entails first premolar extractions and maximum anchorage.
| References | | |
| 1. | Bishara SE, Abdalla EM, Hoppens BJ. Cephalometric comparisons of dentofacial parameters between Egyptian and North American adolescents. Am J Orthod 1990;97: 413-21.  |
| 2. | Dale GK, Dale CH. Interceptive guidance of occlusion with emphasis on diagnosis. In: Graber MT, editor. Orthodontics Current Principles and Techniques. 3 rd ed. Missouri: Mosby Inc.; 2000. p. 385. |
| 3. | Proffit WR, Sarver DM, Ackerman JL. Orthodontic diagnosis: The development of a problem list. In: Proffit RW, editor. Contemporary Orthodontics. 4 th ed. St. Louis: Mosby Elselvier; 2007. |
| 4. | Bills DA, Handelman CS, BeGole EA. Bimaxillary dentoalveolar protrusion: Traits and orthodontic correction. Angle Orthod 2005;75:333-9. |
| 5. | Dandajena TC, Nanda RS. Bialveolar protrusion in a Zimbabwean sample. Am J Orthod 2003;123:133-7. |
| 6. | Aldrees AM, Shamlan MA. Morphological features of bimaxillary protrusion in Saudis. Saudi Med J 2010;31:512-9. |
| 7. | Lamberton CM, Reichart PA. Bimaxillary protrusion as a pathologic problem in the Thai. Am J Orthod Dentofacial Orthop 1980;77:320-9. |
| 8. | Kowalski CJ, Nasjleti CE, Walker GF. Differential diagnosis of adult male black and white populations. Angle Orthod 1974;44:346-50. [ PUBMED] |
| 9. | de Freitas LM, de Freitas KM, Pinzan A, Janson G, de Freitas MR. A comparison of skeletal, dentoalveolar and soft tissue characteristics in white and black Brazilian subjects. J Appl Oral Sci 2010;18:135-42. |
| 10. | Sharkey HJ. Arab identity and ideology in Sudan: The politics of language, ethnicity, and race. Afr Aff 2008;107:21-43. |
| 11. | Ibrahim ES. Skeleto-Dental and Soft Tissue Relationship Among a Sudanese Sample: A Cephalometric Study. MSc Thesis. U of K. Sudan; 2008. |
| 12. | Almanan SS. Soft Tissue Cephalometric Analysis Among Sudanese University Students: A Cephalometric Study. MSc Thesis. U of K. Sudan; 2008. |
| 13. | Caufield WP. Tracing technique and identification of landmarks. In: Jacobson A, editor. Radiograpgic Cehalometry from Basics to Video Imaging. 2 nd ed. Surrey: Quintescence Publishing Co.; 1995. |
| 14. | Viteporn S, Athanasiou AE. Anatomy, radiographic anatomy and cephalometric landmarks of craniofacial skeleton, soft tissue profile, dentition, pharynx and cervical vertebrae. In: Athanasiou EA, editor. Orthodontic Cephalometry. 1 st ed. London: Mosby-Wolfe; 1995. |
| 15. | Keating PJ. Bimaxillary protrusion in the Caucasian: A cephalometric study of the morphological features. Br J Orthod 1985;12:193-201. [ PUBMED] |
| 16. | Sivakumar A, Sivakumar I, Sharan J, Kumar S, Gandhi S, Valiathan A. Bimaxillary protrusion trait in the Indian population: A cephalometric study of the morphological features and treatment considerations. Orthod Waves 2014;73:95-101. |
| 17. | Jacobson A. The "Wits" appraisal of jaw disharmony. Am J Orthod 1975;67:125-38. [ PUBMED] |
| 18. | Lahlou K, Bahoum A, Makhoukhi MB, Aalloula el H. Comparison of dentoalveolar protrusion values in Moroccans and other populations. Eur J Orthod 2010;32:430-4. |
| 19. | Connor AM, Moshiri F. Orthognathic surgery norms for American black patients. Am J Orthod Dentofacial Orthop 1985;87:119-34. |
| 20. | Drummond RA. A determination of cephalometric norms for the Negro race. Am J Orthod 1968;54:670-82. [ PUBMED] |
| 21. | Fonseca RJ, Klein WD. A cephalometric evaluation of American Negro women. Am J Orthod 1978;73:152-60. [ PUBMED] |
| 22. | Diels RM, Kalra V, DeLoach N Jr, Powers M, Nelson SS. Changes in soft tissue profile of African-Americans following extraction treatment. Angle Orthod 1995;65:285-92. |
| 23. | Hussein E, Abu Mois M. Bimaxillary protrusion in the Palestinian population. Angle Orthod 2007;77:817-20. |
| 24. | Kowalski CJ, Harris JE, Walker SJ. The craniofacial morphology of Nubian schoolchildren. Angle Orthod 1975;45:180-4. [ PUBMED] |
| 25. | Kirschen RH, O′higgins EA, Lee RT. The Royal London Space Planning: An integration of space analysis and treatment planning: Part I: Assessing the space required to meet treatment objectives. Am J Orthod Dentofacial Orthop 2000;118:448-55. |
| 26. | Mitchel L. An Introduction to Orthodontics. 3 rd ed. New York: Oxford University Press Inc.; 2000. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3], [Table 4]
|










 Search Pubmed for
Search Pubmed for