|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 204-207 |
|
Three cases with pycnodysostosis in a family
Çiçek Yilmaz, Hasan Kamak
Department of Orthodontics, Faculty of Dentistry, Kirikkale University, Kirikkale, Turkey
| Date of Web Publication | 11-Sep-2015 |
Correspondence Address:
Hasan Kamak
Department of Orthodontics, Faculty of Dentistry, Kirikkale University, 71100 Kirikkale
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.159543

Pycnodysostosis (the Toulouse - Lautrec syndrome), a rare autosomal-recessive disorder is caused by cathepsin K mutation. The main features of the disorder are osteosclerosis, bone fragility, short stature, acro-osteolysis, and delayed closure of the cranial sutures. Other common features are prominent eyes with blue sclera, beaked nose, clavicular dysplasia, obtused mandibular gonial angle, and in some cases visceromegaly. The aim of this case report is to emphasize the main aspects of interest to the orthodontists to give the right treatment to this population. Keywords: Blue sclera, osteopetrosis, pycnodysostosis
How to cite this article:
Yilmaz Ç, Kamak H. Three cases with pycnodysostosis in a family. J Orthod Res 2015;3:204-7 |
| Introduction | |  |
Pycnodysostosis was first described in 1962 by Maroteaux and Lamy. It is a rare lysosomal storage disease of the bone due to a mutation in the gene that codes the enzyme cathepsin K and this causes osteosclerosis. [1] The most frequent clinical maxillofacial features are: Grooved palate, midfacial hypoplasia, mandibular hypoplasia, and enamel hypoplasia. The most common radiographic maxillofacial features are: Obtuse mandibular angle, frontal/parietal/occipital bossing, open fontanels and sutures, multiple impacted teeth. [2] Early diagnosis is important to plan the more suitable treatment to provide a better life quality to the patients and this has a fundamental role in patients' general health. We consider that is very important that the dentist know the radiographic and clinical maxillofacial features of pycnodysostosis, which allows correct treatment planning avoiding risks and ensuring better life's quality to the patients.
| Case Report | | |
An 8-year-old female patient was referred to the Department of Orthodontics, Faculty of Dentistry, Kirikkale University, Kirikkale, Turkey for dental treatment. Patient's chief complaint was maxillary retrusion and crowded teeth. There was no report of abnormalities either during pregnancy or during childbirth. Her medical history revealed that at 5 years of age, the patient had a complete survey in a private medical clinic to investigate growth retardation (without conclusive results, according to her guardian). The patient has a sibling and the other sibling did not have the same problem. At the time of the appointment, she was attending school at a level compatible with her age group. The general clinical examination showed short stature, frontal bulge and disproportion of the size of her head with face, which was small [Figure 1]. | Figure 1: The patient's extraoral photographs and cephalometric radiograph
Click here to view |
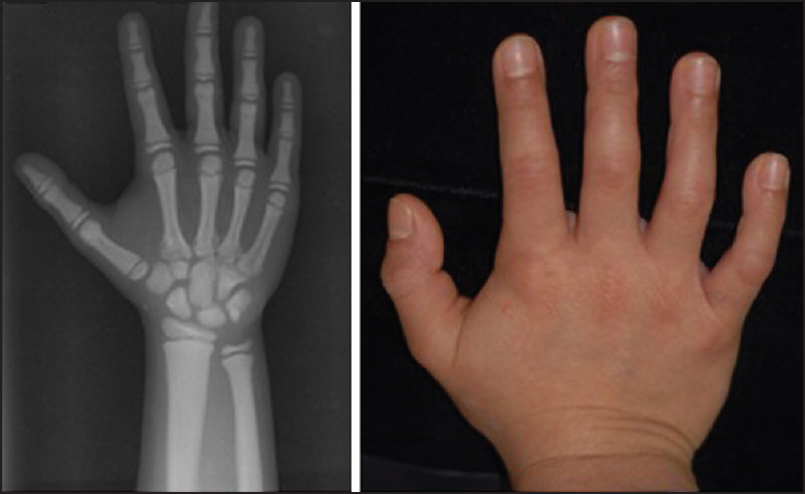
The weight and standing height of the patient were 26 kg and 122 cm, respectively. She also had shortened fingers, but the structure of nails was normal [Figure 2].
She also had a history of mouth breathing and atypical swallowing. At the intrabuccal clinical examination anterior open bite, posterior cross bite, deep palate, mandibular, and maxillary atresia were noted [Figure 3]. Lateral cephalogram showed thickening of the cranial base, a straight mandibular angle and panoramic radiography showed a lack of maxillary lateral incisors and left bicuspid.
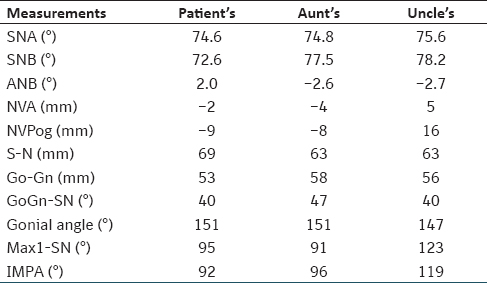
At the family history [Figure 4], her maternal aunt and uncle also had the same complaints, but they had not sought any medical attention [Figure 5] and [Figure 6]. Cephalometric measurements of the patient and the aunt and uncle's are showed at [Table 1].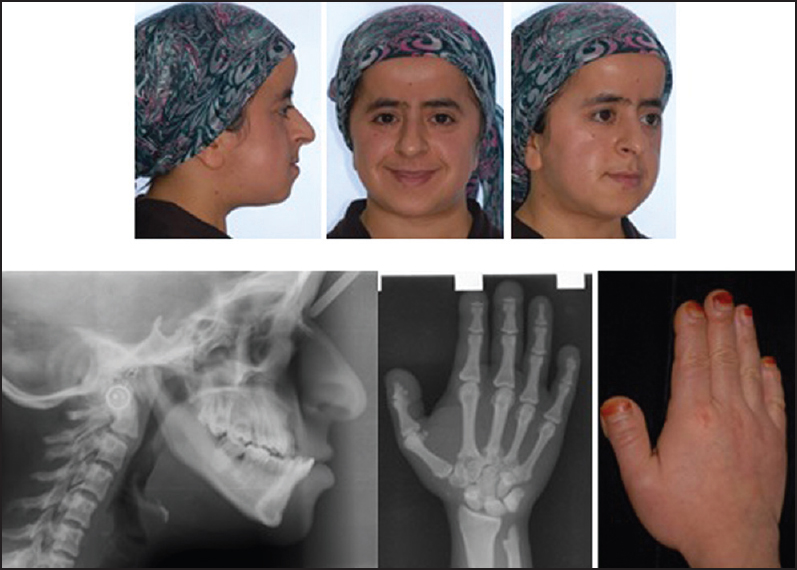 | Figure 5: The aunt's extraoral, hand photos and cephalometric, handwrist films
Click here to view |
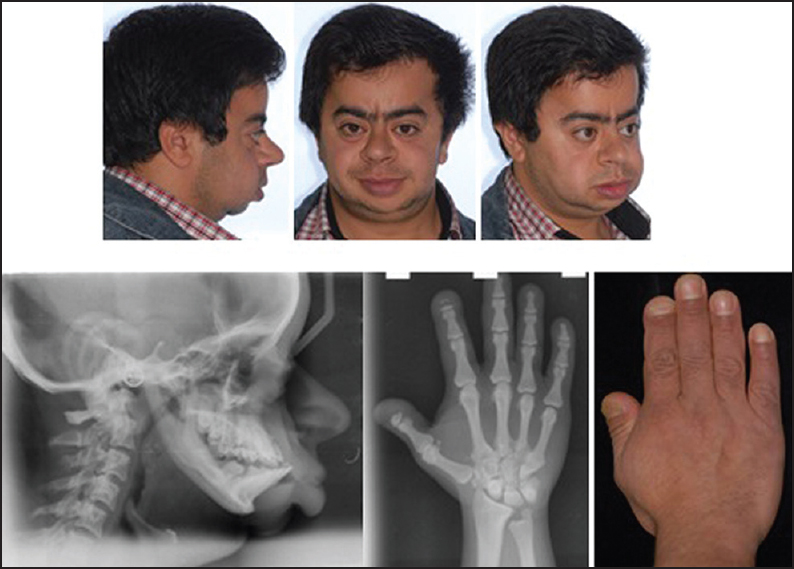 | Figure 6: The uncle's extraoral, hand photos and cephalometric, hand-wrist films
Click here to view |
We applied space maintainer for the early missing teeth in the lower arch of the patient. An association of the clinical and radiographic data suggested pycnodysostosis as the most likely diagnosis. The patient was then sent to the University's Pediatric Genetic Clinic, where the diagnosis was confirmed. The written informed consent of patients has been obtained for their photograph publication.
| Discussion | | |
Pycnodysostosis is a rare autosomal-recessive disorder with osteosclerosis which is caused from osteoclast dysfunction. [3] There could be various phenotypes. Clinically, the most frequent characteristics of maxillofacial phenotype are: Grooved palate, midfacial hypoplasia, mandibular hypoplasia, and enamel hypoplasia. The most common radiographic maxillofacial characteristics are: Frontal/parietal/occiptal bossing, open fontanels and sutures, multiple impacted teeth. [2] Furthermore, features include prominent eyes with blue sclerae, relative proptosis, beaked nose, hypoplastic paranasal sinuses, and an obtuse mandibular gonial angle, often with relative prognathism. [4],[5],[6] The incident of main clinical maxillofacial features in the pycnodysostosis are a grooved palate (66.66%), midfacial hypoplasia (60.60%), mandibular hypoplasia (39.39%), enamel hypoplasia (33.33%), dental crowding (36.36%), narrow palate (27.27%), cross bite (27.27%), Class III skeletal (24.24%), open bite (21.21%), and dental abnormalities (21.21%) [2] General features include short stature (<150 cm), generalized diffuse osteosclerosis with a tendency for fracture after minimal trauma, and hypoplastic clavicles. [4],[6]
The observation of mandibular and maxillary hypoplasia in pycnodysostosis can cause craniofacial disproportion. [7],[8] In our case, this craniofacial disproportion is also dramatically seen. Mandibular angular loss (flattening the angle between corpus-rami), which is another finding of pycnodysostosis, accompanied by Platibazi. [7],[8] Expected the normal value of mandibular angle or, in other words, gonial angle is average 130 ± 7°. [9],[10] With the mandibular angle measurement made also in this case, the angle was found 151° and being angle wider than the normal value is determined as another finding consistent with the literature. According to Soliman et al. the reason of short stature is that increased bone volume in sella turcica causes a deficiency in growth hormone production by making compression pituitary gland. In our case, there is pathologically short stature compatible with literature. Another problem that can be observed in cases is a respiratory failure due to the compression of extremely long soft palate to tongue. [11] Mouth breathing, and complaints of snoring at night is also exist in our case. It was learned that the uncle and the aunt of patient's anterior fontanelle are open and short stature. This case is determined as a familial pycnodysostosis case.
Osteopetrosis is a familial disorder that can be seen rarely whereby the bones harden, becoming denser, in contrast to more prevalent conditions like osteoporosis, in which the bones become less dense and more brittle, or osteomalacia, in which the bones soften. Osteopetrosis can cause bones to dissolve and break. [12] Sclerotic view in head bones is more uncertain in pycnodysostosis than the one in osteopetrozis. [13],[14] Blue sclera can be seen in the both diseases, is the common symptoms of these diseases. [15],[16] However, blue sclera was not sufficiently striking in our patient.
Currently, there is not any suggestion or information about efficacy and safety of orthodontics in children or even young adults with pycnodysostosis in the literature. Orthodontic and orthopedic interventions are totally related osteoclastic activity and bone resorption and remodeling capacities. It is found that deficiency of the lysosomal cysteine protease cathepsin K cause this osteopetrotic disease, now it is classified as a lysosomal disorder. [16]
Because osteomyelitis has been defined as a common occurrence in adults with pycnodysostosis, surgery, and comprehensive oral rehabilitation are challenges for these patients. For this reason, surgical intervention should be done earlier in life when risk factors for osteomyelitis development are reduced. [17],[18]
As a result, there is no specific treatment for this anomaly and the current treatment is only supportive. Frequent visits would be suitable for these patients to prevent dental decay and periodontal disease. [19]
| References | | |
| 1. | Schiller AL, Krane SM. Hyperostosis, fibrous dysplasia, and other dysplasias of bone and cartilage. New York, USA: McGraw-Hill; 1998.  |
| 2. | Alves N, Cantín M. Clinical and radiographic maxillofacial features of pycnodysostosis. Int J Clin Exp Med 2014;7: 492-6. |
| 3. | Beighton P, Horan F, Hamersma H. A review of the osteopetroses. Postgrad Med J 1977;53:507-16. |
| 4. | Hunt NP, Cunningham SJ, Adnan N, Harris M. The dental, craniofacial, and biochemical features of pyknodysostosis: A report of three new cases. J Oral Maxillofac Surg 1998;56: 497-504. |
| 5. | Glass RB, Fernbach SK, Norton KI, Choi PS, Naidich TP. The infant skull: A vault of information. Radiographics 2004;24:507-22. |
| 6. | Bathi RJ, Masur VN. Pyknodysostosis - A report of two cases with a brief review of the literature. Int J Oral Maxillofac Surg 2000;29:439-42. |
| 7. | Motyckova G, Fisher DE. Pycnodysostosis: Role and regulation of cathepsin K in osteoclast function and human disease. Curr Mol Med 2002;2:407-21. |
| 8. | Edeiken J. Roentgen Diagnosis of Disease of Bone. Baltimore, London: Williams & Wilkins; 1981. |
| 9. | Vanhoenacker FM, De Beuckeleer LH, Van Hul W, Balemans W, Tan GJ, Hill SC, et al. Sclerosing bone dysplasias: Genetic and radioclinical features. Eur Radiol 2000;10: 1423-33. |
| 10. | Hockel JL. Orthopedic Gnathology. Chicago, Illinois: Quintessence Pub. Co.; 1983. |
| 11. | Muto T, Yamazaki A, Takeda S, Tsuji Y, Shibata T. Pharyngeal narrowing as a common feature in pycnodysostosis - A cephalometric study. Int J Oral Maxillofac Surg 2005;34: 680-5. |
| 12. | Lam DK, Sándor GK, Holmes HI, Carmichael RP, Clokie CM. Marble bone disease: A review of osteopetrosis and its oral health implications for dentists. J Can Dent Assoc 2007;73:839-43. |
| 13. | Soliman AT, Ramadan MA, Sherif A, Aziz Bedair ES, Rizk MM. Pycnodysostosis: Clinical, radiologic, and endocrine evaluation and linear growth after growth hormone therapy. Metabolism 2001;50:905-11. |
| 14. | Meschan I. Roentgen Signs in Diagnostic Imaging. Philedelphia: W.B. Saunders Company; 1985. p. 320-1. |
| 15. | Silverman F. Caffey′s Pediatric X-ray Diagnosis. Chicago: Year Book Medical Publishers, Inc.; 1990. |
| 16. | Gelb BD, Shi GP, Chapman HA, Desnick RJ. Pycnodysostosis, a lysosomal disease caused by cathepsin K deficiency. Science 1996;273:1236-8. |
| 17. | Zachariades N, Koundouris I. Maxillofacial symptoms in two patients with pyknodysostosis. J Oral Maxillofac Surg 1984;42:819-23. |
| 18. | Muto T, Michiya H, Taira H, Murase H, Kanazawa M. Pycnodysostosis. Report of a case and review of the Japanese literature, with emphasis on oral and maxillofacial findings. Oral Surg Oral Med Oral Pathol 1991;72:449-55. |
| 19. | Kamak H, Kamak G, Yavuz I. Clinical, radiographic, diagnostic and cephalometric features of pycnodysostosis in comparison with Turkish cephalometric norms: A case report. Eur J Dent 2012;6:454-9. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]
[Table 1]
|












 Search Pubmed for
Search Pubmed for