|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 4
| Issue : 1 | Page : 13-17 |
|
Bond strength of aged lingual retainers
Sertac Aksakalli1, Bayram Corekci2, Celal Irgin2, Bora Ozturk3, Siddik Malkoc4
1 Department of Orthodontics, Bezmialem Vakif University, Istanbul, Turkey
2 Department of Orthodontics, Abant Izzet Baysal University, Bolu, Turkey
3 Department of Restorative Dentistry, Selcuk University, Konya, Turkey
4 Department of Orthodontics, Inonu University, Malatya, Turkey
| Date of Web Publication | 5-Apr-2016 |
Correspondence Address:
Sertac Aksakalli
Bezmialem Vakif University, Di? Hekimli?i Fakültesi, Ortodonti Anabilim Dali, Fatih, Istanbul
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.172219

Introduction: The purpose of this study was to examine the tensile bond strength (TBS) of two different lingual retainer (LR) composite systems and three LR wires after they were aged by loadcycling and thermocycling. Materials and Methods: A 15 mm length of wire was bonded to the lingual surfaces of pairs of human incisors using two bonding techniques. Seventy-two pairs of incisors were placed into six groups, and loadcycling (50,000 times) and thermocycling (10,000 times) were performed. The failure characteristics examined included the maximum force for debonding and the site of failure. The adhesive remnant index scores were calculated. Data were compared by two-way analysis of variance and Tukey highly significant difference analysis. Results: All groups generally showed statistically significant differences in TBS score (P < 0.05). For each group, the highest average TBS score (P < 0.05) was obtained from a Transbond LR + Remalloy LR combination. The main failure type was a mixed failure. Conclusions: Retainer wire and composite combinations had significant differences. One of the best selection criteria for LRs is the determination of the bond strength needs of a case. Keywords: Orthodontics, retainer, retention
How to cite this article:
Aksakalli S, Corekci B, Irgin C, Ozturk B, Malkoc S. Bond strength of aged lingual retainers. J Orthod Res 2016;4:13-7 |
| Introduction | |  |
Relapse after orthodontic therapy is an unpredictable and ubiquitous situation. [1] Littlewood et al. reported that relapse is usually seen on the lower anterior teeth. [2] To achieve stability and avoid relapse after treatment, orthodontists have studied different types and applications of lingual retainers (LRs). [3] Most of the studies stated that the fixed retainers were the most effective method for stabilization. [4] For the lower jaw, it has been thought that retainers bonded to six teeth are more efficient for preventing relapse. [5]
The most frequently selected retainers are stainless steel wires. Previously, LRs were produced from thick, round wires (0.030-0.032-inch), and they were bonded at the ends of the retention area. In this type of retainer, intercanine width is secured, and oral hygiene can be well-established. However, the rotation of the other unbonded teeth is evident. [2] Thinner multistranded wires (0.0195-0.0215-inch) were then introduced and bonded to each tooth to treat the rotation problem. [6] This retainer type also has disadvantages such as more plaque accumulation and higher failure rates and breakages. [7] Another type of retainer was the fiber-reinforced composite (FRC). An FRC allows chemical adhesion of the retainer to the bonding agent. With FRCs, the bonding interface between two materials can be annihilated. The problems with FRCs were decreased survival rates and many retainer failures. In the end, multistranded wires are the most popular retainers. [8]
The mode of failure for retainers has been researched; the most common failure mode was a loosening connection between the wire and the composite. [9] Bearn et al. [10] reported that the most common failure was in the wire-composite interface, although Lumsden et al. [11] reported that the most failure was seen at the adhesive pad. Another study reported that the majority of the failures were observed in the first 6 months after placement. [12]
Bonded LRs have to serve for long periods of time in the mouth. The researchers attempted to increase their success rates and durability. Loosening of the wire in bonded retainers can result from cracks in the composite, so wire and adhesive selection is very important for the best results. [9] Therefore, the purpose of this study was to examine the tensile bond strength (TBS) and failure modes of two different LR composite systems (Light Bond Retainer and Transbond LR) and three LR wires (Five-stranded wire Penta-One™ , Remalloy™ , and Ribbond™ ) after they were aged by loadcycling and thermocycling in vitro.
| Materials and Methods | | |
One hundred forty-four lower human incisor teeth were collected from patients who were undergoing dental therapies and their incisor teeth were extracted from periodontal problems. Teeth with cracks, caries, and abnormalities were excluded. Soft-tissue remnants were removed with a scaler, and teeth were stored in a 0.1% thymol solution. The solution was changed weekly to avoid bacterial growth. Author, S.A., performed collection and preparation of the teeth.
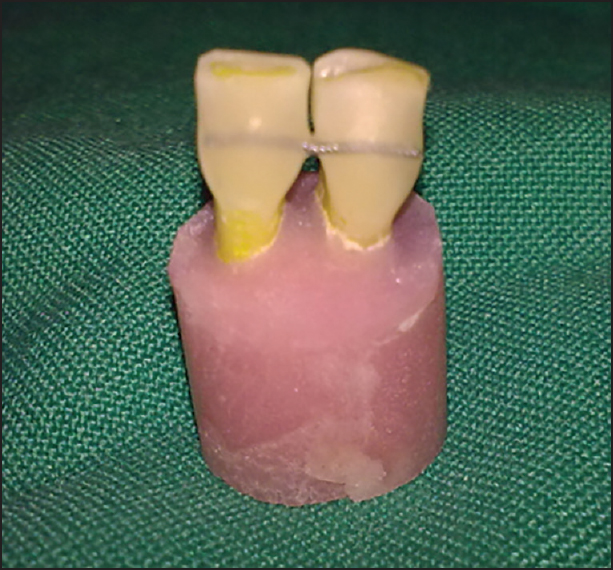
Pairs of teeth were matched to make a contact area to mimic the intraoral situation. Chemically cured acrylic resin was placed into plastic molds, and the roots of the teeth were embedded in acrylic [Figure 1]. The roots were mounted so that the long axis of the teeth was perpendicular to the base of the molds. The Ethical Committee in Selcuk University has approved the study.
The lingual parts of the teeth were polished with fluoride-free pumice (Zircate Prophy Paste, Dentsply Caulk, Milford, DE, USA) using a prophylaxis brush (Hawe Prophy Cup and Brush, latch-type, Kerrhawe Sa, Bioggio, Svizzera, Switzerland) for 20 s and were then rinsed with water and air-dried. The mesiodistal dimensions of the two teeth in each specimen were measured, and the midpoint 3 mm below the incisal edges was marked as the region for bonding.
Retainer Materials and Placement
Seventy-two specimens were randomly divided into six groups (n = 12). Groups and their explanations are shown in [Table 1]. Light Cure Retainer (Reliance, Reliance Orthodontic Products, Itasca, IL, USA) and Transbond LR (3M Unitek, Monrovia, CA, USA) composites were used with three different wires: Five-stranded wire Penta-One™ (0.0215-inch round wire), Remalloy™ (0.032-inch plain round wire), and Ribbond™ (Ribbond Inc., Seattle, USA). All composites were used according to the manufacturers' instructions.
Debonding Force Testing
All tests were performed in Selcuk University Dental Laboratories except stereomicroscopic evaluation. It was performed in Bezmialem University Research Center. All specimens were subjected to 10,000 thermal cycles between 55°C and 5°C using a digital thermocycling machine (Willytec/SD, Mechatronik GmbH, Munich, Germany), with a dwell time of 60 s and a transition time of 15 s [Figure 2]. For the cyclic loading procedure, in each group, the specimens were subjected to loading forces at the incisal edges of the incisors and were placed in a universal testing machine (Zwickroll, Z050, Zwick GmbH, Ulm, Germany) for mechanical cycling. The upper rod of the cycling machine could apply load pulses from 15 to 50 N at a frequency of 5 Hz. The specimens were cycled 50,000 times at a crosshead speed of 1 mm/min [Figure 3]. The specimens were used in debonding load testing. Embedded specimens were placed in a jig attached to the base plate of an Instron Testing Machine (Instron Corporation, Norwood, MA, USA). A chisel edge plunger was mounted on the crosshead of the testing machine and positioned so that the leading edge was aimed at the marked midpoint of the wire. The crosshead speed was set at 1 mm/min, and the maximum load necessary to debond the wire was recorded. TBSs were calculated.
The fracture mode was evaluated on the side where the initial bond failure occurred by using an optical stereomicroscope (SZ40, Olympus, Tokyo, Japan) at ×20 magnification. Remnant adhesive on the enamel surface was recorded by one researcher blinded to the study groups [Figure 4]. According to the adhesive remnant index, the fractures were coded and ranked from 0 to 3, based on the amount of adhesive remaining on the bracket removal. [13]
Statistical Analysis
All statistical analysis was performed using SPSS 17.0 (SPSS Inc., Chicago, Ill, USA). Descriptive statistics were calculated. Due to normal distributions, means were analyzed by two-way analysis of variance and the Tukey highly significant difference test to evaluate differences. For adhesive remnants, Chi-square analysis was performed. For the P < 0.05 was considered significant.
| Results | | |
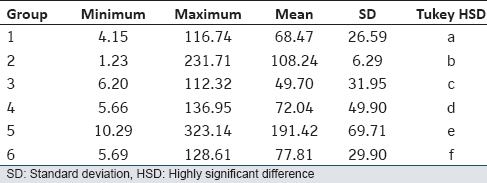
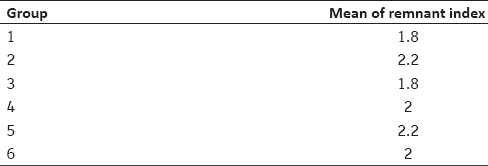
All groups generally showed statistically significant differences in TBS score (P < 0.05) for each composite and wire [Table 2]. Further, for the interaction of composites and wires, there were no statistically significant differences in TBS. For each group, the highest average TBS score (P < 0.05) was obtained from a Transbond LR + Remalloy LR combination, whereas the lowest score was seen in the Light Cure Retainer + Ribbond group. Generally, retainer wires used with Transbond LR gave higher results than Light Bond groups. When compared wires, Remalloy revealed higher strength values than the others. The main failure type was the fracture of the composite bond at the wire-composite interface, a mixed failure. There was no significant difference between the groups [Table 3].
| Discussion | | |
In the current study, none of the retainers on the specimens failed during thermocycling and loadcycling. This result is attributable to specimen properties, especially only two units were included. Two teeth formed a short retainer complex when compared with that used in the clinic. However, loadcycling could not be performed 4 or 6 units because of the experimental design. Cooke and Sherriff [14] used two units in their similar study. LRs are subjected to different stresses because of mastication, intraoral habits, and occlusion. [15],[16],[17] These types of loading forces trigger fatigue and can cause sectional or total failure of some components of the retainer. These forces seem to be below the maximum debonding forces in in vitro research, although they can have devastating effects when rare but sudden high magnitude impacts occur. Hence, the fatigue tests we used in the current research are expected to explain the durability better than static tests. [15],[18]
In this study, the specimens were loaded for 50,000 cycles under 50 N, representing the ideal occlusal forces during mastication and swallowing. [19] Fifty thousand cycles at 50 N simulates 3 months of oral masticatory stresses. [20] The durability of the bond between teeth and bonding resin in clinical use should be evaluated. The 10,000 thermocycles correspond to approximately 12 months under humidity and temperature changes. [21] Thermocycling is used to determine whether temperature variations might influence the bond strength of LRs. [22] According to De Munck et al., [23] decrease in the bond strength might be caused by hydrolytic degradation of the interface components. Most retainer failures have been observed within the first 12 months. [24] Hence, it is important to study changes of aged LRs since the incisors are more susceptible to relapse after orthodontic treatment. [25]
The type of composites and bonding agents is an important factor in the failure mechanism of LRs. In the current study, Transbond LR and the Light Bond Retainer system were used. Because a variety of composites and bonding agents is used for LRs, it is very hard to make comparisons. [26] In this study, both composites were light cured composites, and the Transbond LR had higher bond strength values when compared to the Light Bond Retainer composite. However, it has been reported that chemically cured adhesives have had higher survival rates than the others. [12],[24] Ramoglu et al. [27] stated that Transbond LR is the ideal resin for LRs in their bond strength study.
In the current study, Remalloy (0.032-inch plain wire) had the highest TBS value. Similarly, Artun et al. [6] compared failure rates of 0.032-inch plain wire, 0.032-inch spiral wire, and 0.0205-inch spiral wire and concluded that thick wires had lower failure rates than thin wires. In addition, Bearn et al. stated that larger diameter wires with greater surface area require a greater force to pull the wire. [10] Zachrisson [28] reported that wire fractures decrease as wire diameter increases. However, apart from these results, retainer wires must still be flexible enough to allow physiologic tooth movement. Thus, periodontal health can be maintained while stress decreases within the retainer and composite. [29] Uner et al. [30] studied the differences between Hawley appliance and LRs, stated there was no difference in periodontal effects of these two types. The Penta-One group had less deformation than the Ribbond group. This result in the Penta-One group was able to cause more force transfer to the periodontium than the Ribbond group, which would aid periodontal health. Moreover, easily deformed wires can be deformed by mastication forces or flossing the area beneath the retainer wires.
When applying the results of this study to clinical applications, care must be taken, because this was an in vitro study. The intraoral environment is affected by multiple factors such as diet, oral habits, and saliva. This study was performed under well-controlled circumstances in vitro. Although every stage in the current study was highly similar to intraoral conditions, it would be inappropriate to expect the same results in vivo. Bearn [7] stated that composite abrasion and detachment between the wire and composite were the main causes of retainer failure. According to a similar study conducted by Artun and Urbye, [9] failures mostly occur between the wire and resin. In the current study, the main failure was found between the wire and the resin.
The enamel age, lingual morphology, and sizes of the teeth affect the forces exerted at the bonding interfaces. [14] The current study was limited by the usage of human lower incisors. We included teeth with various morphologies and donor ages to more greatly imitate in vivo conditions, as performed by Baysal et al. [29] A large range of retainer wires and composites are available so that different combinations could be used and the number of specimens could be increased.
| Conclusions | | |
Within the limitations of this study, it can be concluded that retainer wire selection is more important than composite selection. However, due to significant differences among groups, wire and composite usage should be determined according to the bond strength needs of each case.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
| References | | |
| 1. | Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop 1988;93:423-8.  |
| 2. | Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev 2006;1:CD002283. |
| 3. | Nanda RS, Nanda SK. Considerations of dentofacial growth in long-term retention and stability: Is active retention needed? Am J Orthod Dentofacial Orthop 1992;101:297-302. |
| 4. | Zachrisson BU. Clinical experience with direct-bonded orthodontic retainers. Am J Orthod 1977;71:440-8. |
| 5. | Zachrisson BJ. Third-generation mandibular bonded lingual 3-3 retainer. J Clin Orthod 1995;29:39-48. |
| 6. | Artun J, Spadafora AT, Shapiro PA. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod 1997;19:501-9. |
| 7. | Bearn DR. Bonded orthodontic retainers: A review. Am J Orthod Dentofacial Orthop 1995;108:207-13. |
| 8. | Renkema AM, Renkema A, Bronkhorst E, Katsaros C. Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofacial Orthop 2011;139:614-21. |
| 9. | Artun J, Urbye KS. The effect of orthodontic treatment on periodontal bone support in patients with advanced loss of marginal periodontium. Am J Orthod Dentofacial Orthop 1988;93:143-8. |
| 10. | Bearn DR, McCabe JF, Gordon PH, Aird JC. Bonded orthodontic retainers: The wire-composite interface. Am J Orthod Dentofacial Orthop 1997;111:67-74. |
| 11. | Lumsden KW, Saidler G, McColl JH. Breakage incidence with direct-bonded lingual retainers. Br J Orthod 1999;26:191-4. |
| 12. | Lie Sam Foek DJ, Ozcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of flexible, braided, bonded stainless steel lingual retainers: A historic cohort study. Eur J Orthod 2008;30:199-204. |
| 13. | Oliver RG. The effect of different methods of bracket removal on the amount of residual adhesive. Am J Orthod Dentofacial Orthop 1988;93:196-200. |
| 14. | Cooke ME, Sherriff M. Debonding force and deformation of two multi-stranded lingual retainer wires bonded to incisor enamel: An in vitro study. Eur J Orthod 2010;32:741-6. |
| 15. | Ruse ND, Shew R, Feduik D. In vitro fatigue testing of a dental bonding system on enamel. J Biomed Mater Res 1995;29:411-5. |
| 16. | Grandini S, Chieffi N, Cagidiaco MC, Goracci C, Ferrari M. Fatigue resistance and structural integrity of different types of fiber posts. Dent Mater J 2008;27:687-94. |
| 17. | Bani M, Bani A. Oral health awareness and rehabilitation oral health of orthodontic patients. J Dent Fac Ataturk Univ 2014;24:442-51. |
| 18. | McCabe JF, Carrick TE, Chadwick RG, Walls AW. Alternative approaches to evaluating the fatigue characteristics of materials. Dent Mater 1990;6:24-8. |
| 19. | Bolhuis P, de Gee A, Feilzer A. Influence of fatigue loading on four post-and-core systems in maxillary premolars. Quintessence Int 2004;35:657-67. |
| 20. | Kumar N, Aggarwal V, Singla M, Gupta R. Effect of various endodontic solutions on punch out strength of Resilon under cyclic loading. J Conserv Dent 2011;14:366-9. [ PUBMED]  |
| 21. | Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of dental restorations. J Dent 1999;27:89-99. |
| 22. | Yuasa T, Iijima M, Ito S, Muguruma T, Saito T, Mizoguchi I. Effects of long-term storage and thermocycling on bond strength of two self-etching primer adhesive systems. Eur J Orthod 2010;32:285-90. |
| 23. | De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, et al. A critical review of the durability of adhesion to tooth tissue: Methods and results. J Dent Res 2005;84:118-32. |
| 24. | Störmann I, Ehmer U. A prospective randomized study of different retainer types. J Orofac Orthop 2002;63:42-50. |
| 25. | Parker GR. Transseptal fibers and relapse following bodily retration of teeth: A histologic study. Am J Orthod 1972;61:331-44. |
| 26. | Rose E, Frucht S, Jonas IE. Clinical comparison of a multistranded wire and a direct-bonded polyethylene ribbon-reinforced resin composite used for lingual retention. Quintessence Int 2002;33:579-83. |
| 27. | Ramoglu SI, Uysal T, Ulker M, Ekizer A. Shear Bond Strength Evaluation of Different Composites Used As Lingual Retainer Adhesives. Turk J Orthod 2008;21:196-205. |
| 28. | Zachrisson BU. The bonded lingual retainer and multiple spacing of anterior teeth. Swed Dent J Suppl 1982;15: 247-55. |
| 29. | Baysal A, Uysal T, Gul N, Alan MB, Ramoglu SI. Comparison of three different orthodontic wires for bonded lingual retainer fabrication. Korean J Orthod 2012;42:39-46. |
| 30. | Uner O, Akkaya M, Akkaya S. Retansiyon apereylerinin periodontal yonden degerlendirilmesi. Gazi Univ Dishekim Fak Derg 1994;11:57-61. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
[Table 1], [Table 2], [Table 3]
|













 Search Pubmed for
Search Pubmed for