|


 |
| ORIGINAL ARTICLE |
|
| Year : 2012 | Volume
: 4
| Issue : 1 | Page : 10-14 |
|
|
Total arterial off-pump coronary revascularization with a bilateral internal mammary artery Y graft (208 cases)
Jun-Feng Yang1, Hong-Chao Zhang2, Cheng-Xiong Gu1, Hua Wei1
1 Department of Cardiac Surgery, Beijing Anzhen Hospital, Capital University of Medical Science, Beijing 100029, People's Republic of China
2 Department of Cardiac Surgery, Airfore General Hospital, Beijing 100142, People's Republic of China
| Date of Web Publication | 5-Sep-2012 |
Correspondence Address:
Cheng-Xiong Gu
Department of Cardiac Surgery, Sixth Ward, Beijing Anzhen Hospital, Beijing 100029
People's Republic of China
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.100345

 Abstract Abstract | | |
Objective: The aim was to evaluate the early outcome of off-pump coronary artery bypass grafting (OPCABG) with a bilateral internal mammary artery (BIMA) Y configuration graft to achieve total arterial myocardial revascularization. Materials and Methods: From October 2002 to December 2008, 208 patients (196 male and 12 female patients) underwent OPCABG by only using a BIMA Y configuration graft. The average age of the patients was 56.5±11.3 years, with the age range being 33-78 years. A total of 167 (80.2%) cases had triple-vessel disease. Left main stem disease was found in 33 (15.9%) cases, and double-vessel disease was found in 8 (3.9%) cases. The semiskeletonization skill was used to harvest the two IMAs, and then the free right internal mammary artery was anastomosed end-to-side to the in situ left internal mammary artery to composite a Y configuration graft. Off-pump and sequential anastomosis methods were used to perform coronary artery bypass surgery for the patients. Graft patency was assessed by using the HT311 transit time flowmeter (USA Transonic Systems Inc.), intraoperatively. Results: We performed distal anastomoses of the grafts in 728 patients, the average being 3.5±1.3 per person. No one died and got recurrent angina within 30 days after operation. Conclusion: OPCABG by using the BIMA Y graft was safe and effective to achieve total arterial revascularization, and avoid surgical operation on the ascending aorta, and other incisions. Keywords: Bilateral internal mammary arteries, coronary artery bypass grafting, internal mammary artery, LIMA -RIMA Y graft, off-pump
How to cite this article:
Yang JF, Zhang HC, Gu CX, Wei H. Total arterial off-pump coronary revascularization with a bilateral internal mammary artery Y graft (208 cases). J Surg Tech Case Report 2012;4:10-4 |
How to cite this URL:
Yang JF, Zhang HC, Gu CX, Wei H. Total arterial off-pump coronary revascularization with a bilateral internal mammary artery Y graft (208 cases). J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:10-4. Available from: http://www.jstcr.org/text.asp?2012/4/1/10/100345 |
| Introduction | |  |
A Y graft is a graft formed by the left internal mammary artery (LIMA) connected to the left anterior descending (LAD) artery and by a free right internal mammary artery (RIMA) connected to the LIMA and to a marginal artery of the left circumflex artery (LCx). Since the internal mammary artery (IMA) conduit for coronary artery bypass grafting (CABG) has better long-term results [1] than saphenous vein grafts (SVGs), the LIMA graft is considered the best graft for bypassing the LAD coronary artery. [2],[3],[4] The RIMA used under the same condition as the LIMA may offer the same results. [5],[6],[7] Thus, Barn [8] , Tector [9] and Barr [10] proposed the Y or T graft procedure carried out by anastomosing the proximal end of the free RIMA to the side of the attached LIMA. This procedure provides an additional length to reach a distal coronary artery branch, such as the posterior descending branch of the right coronary artery, or the post branch of the left ventricle.
Kamathi [11] and Chocron [12] first reported their experiences with off-pump coronary artery bypass grafting (OPCABG) in the last century. Then this technique became more popular because it could avoid more complications caused by cardiopulmonary bypass.
So, we used the bilateral internal mammary artery (BIMA) Y graft under OPCABG for the selected patients. We wanted to know whether it is the most appropriate selection for CABG. It may included four good effects as follow: total arterial revascularization being advantageous to long-term patent of bypass graft, no-touch to aortic avoiding cerebral apoplexy, beautify for wound, and less main organ complications.
In this paper, we have summarized our experience in recent years concerning the off-pump coronary artery bypass surgery using a BIMA Y graft to achieve total arterial revascularization. The report is as follows.
| Materials and Methods | | |
Clinical data
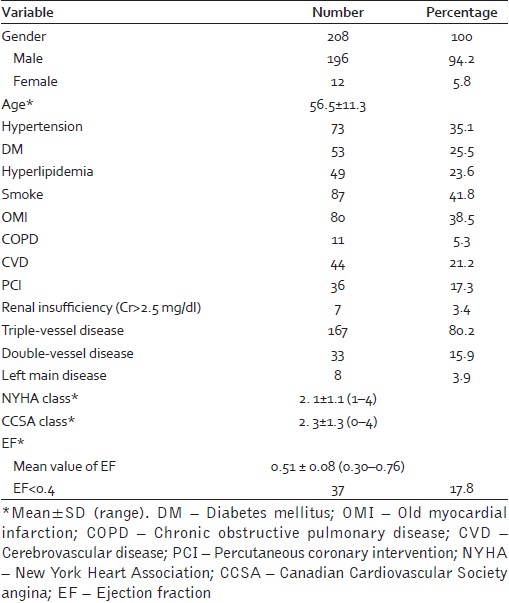
From October 2002 to December 2008, our department completed 208 (196 male and 12 female patients) cases of the CABG surgery using a BIMA Y configuration graft to achieve total arterial myocardial revascularization. The age range of the patients was 33-78 years, with the average age being 56.5±11.3 years. Of the 208 patients, 15 (7.2%) patients were over 70 years of age. Triple-vessel lesions were present in 167 (80.2%) patients, left main trunk lesions in 33 (15.9%), and double-vessel diseases in 8 (3.9%) patients. The data and basic information are given in [Table 1]. At the same time, there were 3561 patients who finished CABG, including 3280 with OPCAB. The most of our patient were done CABG with the operation fashion LIMA + SVG. Patients treated with the BIMA Y graft were 5.84%. The patients were included in different operation groups. Since the results would be effected the different operation method selection preference and learning curve form individual surgeon, we did not compare the result from LIMA + SVG with the BIMA Y graft.
Surgical technique
All patients received general anesthesia under a standardized protocol of the median sternotomy. The semiskeletonization method of the BIMA harvesting technique was employed. [9] Internal mammary artery exposure was achieved with a sternal retractor, and was dissected from the chest wall along with a narrow pedicle of surrounding tissues with electrocautery and hemoclips. The LIMA was harvested first, and dissected from the origin to distal bifurcation. The RIMA was then dissected the same way as the LIMA. After heparinization, the RIMA was removed as a free graft. The LIMA was divided at the last bifurcation. The endothoracic fascia of the BIMAs was then resected with scissors or electrocautery. The IMA pedicle was left with accompanying veins and little fat. Both arteries were placed onto a thick pad of gauze. An oblique 1-cm incision was made in the LIMA, and the proximal end of the RIMA was anastomosed with a continuous 8-0 polypropylene suture. The anastomosis location was under the level of the pulmonary annulus. The BIMA composed a Y configuration graft, with the LIMA being as the short limb of the Y graft, and the RIMA the long one. The length of the RIMA made it possible to graft as far as the lateral circumflex or posterior descending arteries.
Off-pump technique
The off-pump coronary artery bypass surgery was performed by the same surgeon. The patients were heparinized with an initial dose of 1.5 mg/kg of heparin, and periodically received supplemental doses to maintain an activated clotting time of ≥300 s. Anesthesia management, including volume loading and placing the patient in the Trendelenburg position, was controlled hemodynamic derangement during displacement or manipulation of the heart. To reduce the amplitude of ventricular wall movement, a compression-type mechanical stabilizer (Chase; Chase Medical Company) or suction-type mechanical stabilizer (Octopus; Medtronic, Minneapolis, MN, USA) was used. To obtain a bloodless operative field, the small bulldog clamp occluded the coronary flow with a temporary time, and a warm saline solution flush was used. The most critical vessel, the LAD branch in almost all patients, was revascularized first with the LIMA in an end -to-side fashion to provide a backup to the less critical area. Then the diagonal and circumflex branches' sequential anastomoses were performed in a side-to-side perpendicular (diamond) fashion using the RIMA. The posterior descending or distal right coronary artery graft was performed last using the distal end of the RIMA as an end-to-side anastomosis in parallel. All anastomoses were performed with a single continuous 7-0 polypropylene suture, under ×2.5 magnification. After the anastomoses were completed, the flow of the Y graft was measured with the HT311 transit time flowmeter (USA Transonic Systems Inc.). Graft patency was assessed using flow curves, mean flow, and pulsatility index (PI). A left extrapericardial fat pad was secured to anterior percardiotomy, and the sternum was closed with 8 wires.
Cardiac enzyme analyses and electrocadiogram were performed on all patients immediately postoperatively and at 1, 2, and 6 days. A surgical review was done at 1 month postoperatively and routine follow-up was undertaken by the cardiologists.
Statistical analysis
The variables are expressed were means±standard deviations (SDs). The baseline characteristics and outcomes were compared using χ2 analysis for categorical data and Student's t-test for continuous variables. Differences were considered significant only when the P-value was < 0.05.
| Results | | |
A total of 728 distal anastomoses were made in all patients, with an average of 3.5±1.3 bypasses performed for each patient. No one received supplemental vein graft. The flow of the Y graft was measured intraoperatively, which showed that all of the anastomoses were patent. The mean flow in the main stem of the LIMA was 62.8±14.3 ml/min, with the PI being 2.9±1.8. The mean flow of the distal LIMA graft was 32.3±11.1 ml/min, with the PI being 3.2±1.7. The mean flow of the proximal RIMA was 31.8±8.5 ml/min, with the PI being 2.7±1.5. At the same time, 29 (13.9%) cases underwent off-pump ventricular aneurysm plasty; 21 (10.1%) cases underwent coronary artery endarterectomy. There were no perioperative deaths.
A total of 35 (16.8%) patients did not undergo blood transfusion; 4 (1.9%) patients had myocardial infarction perioperatively and 2 (1.0%) cases IABP (aortic balloon pump). Two (1.0%) patients received CRRT (continuous renal dialysis). Three (1.4%) cases needed reentry for bleeding. Six (2.9%) patients developed wound problems (including 2 diabetic patients), with superficial wound infection in 2 (1.0%) patients, sternal dehiscence due to wire loosening in 2 (1.0%), and sternal wound infection in 2 (1.0%) patients (including 1 diabetic patient). One (0.5%) case had a cerebral vascular accident. All patients were successfully discharged from the hospital.
All patients were free of angina at the 1-month visit. Cardiology angiography was not performed because of the economic reason and worry about iatrogenic injury of the LIMA. Only one patient died of CVD at 3 months postoperatively during the follow-up. Others were still alive after a mean follow-up of 20.4±4.3 months (6-69 months) and no patient had newborn myocardial infarction and severe angina. Postoperatively at 6 months, the mean left ventricular ejection fraction was 0.52±0.11, compared with that preoperatively, 0.51±0.08 (P=0.13). Patients' NYHA score was 2.0±1.2 versus 2.1±1.1 (P=0.24). But patients' CCSA score were 1.6±1.1 versus 2.3±1.3 preoperatively (P=0.00001).
| Discussion | | |
In 1967, Kolessov [1] first reported internal mammary artery to coronary artery anastomosis; Green, [2] Tector, [3] Mills, [4] Loop, [5] Dion, [6] and their associates increased the versatility of the IMA in CABG. The lower patency of SVGs compared with IMA grafts awoke more surgeons to apply arterial conduit for coronary bypass, especially using BIMAs. [7],[8] Tector, [9] Barra, [10] Kamath, [11] and Chocron [12] described sequential anastomoses, BIMA anastomoses, the free graft technique, and reimplantation of the RIMA as a free graft into the LIMA in situ to compose a Y or T graft. Good late clinical results were reported by Tector, [9] Tatoulis [13] and Lytle. [14]
Among the various strategies regarding the selection of the ideal arterial graft, the IMA, we used a single Y configuration graft with a free RIMA attached to the side of the LIMA in situ. Through this graft strategy, the LIMA could be anastomosed to the LAD, which was fundamental to CABG because of the graft's superior long-term patency. The other important reason for us to use this graft strategy was to maximize the use of ideal arterial grafts, namely, BIMAs. Patients who had undergone CABG with BIMAs were well known to have long-term results that were superior to those found with only the LIMA. [14],[15] The RIMA was histologically identical to the LIMA, and might show similar long-term patency rates. The length of the semiskeletonized RIMA in the Asian population is approximately 15-20 cm if harvested from the first rib to the bifurcation. In most patients, the RIMA could reach the RCA system without difficulty. Consequently, all of the triple-vessel diseases could be revascularized with the two ideal arterial grafts − the BIMAs. This technique used previously also showed good early clinical and angiographic results when performed without a cardiopulmonary bypass. [16],[17] The total arterial OPCABG using BIMA was with a very low incidence of in-hospital death, complication, and late outcomes compared to the on-pump technique. In our study, the off-pump coronary artery bypass graft with the BIMA Y graft was safe and feasible for all patients. No one was obliged to chang off-pump to on-pump intraoperation, especially including moderate or severe heart function (LVEF < 30%). There was no death within 30 days postoperatively.
Transit-time flowmetry was widely accepted for use in intraoperative graft assessment because it is noninvasive, technically simple, reproducible, fast, and inexpensive. [18],[19],[20] It provided important and accurate intraoperative information on the status and patency of each individual graft. The ideal PI value should be between 1 and 5 after bypass grafts finished. Sometimes the technical error in the anastomosis may increases higher PI values. [18] A problem was thought to be present when the mean flow of the graft was less than 15 ml/min. In our study, the mean flow of all the Y grafts was measured intraoperatively at the main stem, distal LIMA graft, and proximal RIMA. The ideal patent was confirmed, indicating that all the Y grafts were patent following the anastomosis.
Numerous studies had shown that the use of both internal mammary arteries improved long-term survival relative to the use of the left internal thoracic artery and SVGs. However, the concern that diabetes may lead to an increased risk of deep sternal wound infection had limited the use of both internal mammary arteries in nondiabetic patients. [14],[15],[21] Although use of BIMA is considered a risk factor for sternal infection, [22] this risk appears to be attenuated by skeletonized IMA mobilization. [23] Tarrio and colleagues reported the largest group of patients (743 cases) who underwent OPCABG with the BIMA Y or T graft. [24] They used the skeletonization technique to reduce the sternal complication. The rate of mediastinitis was 0.9% (7/743), similar to that in our study (1%, 2/208). In our series, we dissected the BIMA using the narrow pedicle IMA first, and then resected the endothoracic fascia by the semiskeletonization technique. [25],[26] Therefore, more muscle was left attached to the chest wall, thus minimizing sternal devascularization and possibly reducing the risk of deep sternal wound infection as well. In this group, there were six patients who suffered from a wound event, including two diabetic patients. There were two infected, with one diabetic patient. We did not find any difference with the other CABG patients without the BIMA Y graft in our department. If the blood glucose was controlled ideally before operation, and the sternum fracture was avoided, and the sternum was fixed stably in operation, diabetic patients could get same result as no diabetic patients. So we feel that diabetes is not a contraindication to the BIMA Y graft. For a mature team, this technique could be easily performed in daily practice. It was not a time-consuming procedure and was the same technique as the conventional pedicle technique in our department. In fact, a long learning curve is needed for a fresh team. We think freshers should finish 100 conventional CABGs before taking up a BIMA Y graft.
However, total arterial revascularization with two arterial grafts can cause the life-threatening hypoperfusion syndrome [27] because reperfusion of the entire myocardium depends on the proximal source of the left IMA. This scenario had led to the concern whether the flow reserve in the LIMA was sufficient to supply more than one coronary anastomosis. Several reports had concluded that the IMA T graft allowed complete myocardial revascularization with good perioperative results and that the flow reserve of the proximal LIMA was adequate for multiple coronary anastomoses. [28] Clinically, we did not observe any hypoperfusion syndrome in our study, which was consistent with other surgeons who preferred this graft strategy. [29],[30] We performed CABG without CPB to reduce the occurrence of unstable hemodynamics, and avoided using the distal IMA for anastomoses. Adding to that, we did pay more attention to treat first the intercostal artery and removing the unstable hypertension patient. There were evidences that the coronary flow reserve could be improved several months after operation, [31],[32] and that the IMA could adapt to the myocardial blood demand by compensatory dilatation. [33],[34]
OPCABG combined with the aorta no-touch technique has been accepted as an effective procedure to avoid neurologic and aortic complications, and to reduce operative risks. [35] In our study, the incidence of stroke was 0.4% (1 of 208), similar to Tarrío's (0.4%, 3 of 743) and Kim's (0.8%, 4 of 512) results.
In conclusion, the total arterial off-pump coronary bypass grafting using a BIMA Y graft could be safely performed with low in-hospital mortality and complication rates. Surgical tricks and the new technology in coronary stabilizers allow surgeons to perform a complete myocardial coronary revascularization using the best available arterial conduit (BIMA).
| References | | |
| 1. | Kolessov VI. Mammary artery -coronary artery anastomosis as method of treatment of angina pectoris. J Thorac Cardiovasc Surg 1967;54:535-14. 
[PUBMED] |
| 2. | Green GE, Stetzer SH, Reppert EH. Coronary arterial bypass grafts. Ann Thorac Surg 1968;5:443-50.
|
| 3. | Tector AJ, Schmahl TM, Canino VR. The internal mammary artery graft the best choice for bypass of the diseased left anterior descending coronary artery. Circulation 1983;68:II214-7.
[PUBMED] |
| 4. | Mills NL, Bringaze WL. Preparation of the internal mammary artery graft: Which is the best method?. J Thorac Cardiovasc Surg 1989;98:73-9.
|
| 5. | Loop FD, Lytle BW, Cosgrove DM, Golding LA, Taylor PC, Stewart RW. Free (aorta-coronary) internal mammary artery graft late results. J Thorac Cardiovasc Surg 1986;92:827-31.
[PUBMED] |
| 6. | Dion R, Etienne PY, Verhelst R, Khoury G, Rubay J, Bettendorff PH, et al. Bilateral mammary grafting: Clinical, functional and angiographic assessment in 400 consecutive patients. Eur J Cardiothorac Surg 1993;7:287-94.
|
| 7. | Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW, et al. Influence of the internal mammary artery graft on 10-year survival and other cardiac events. N Engl J Med 1986;314:1-6.
[PUBMED] |
| 8. | Barner H, Barnett M. Fifteen-to twenty-one-year angiographic assessment of internal thoracic artery as a bypass conduit. Ann Thorac Surg 1994;57:1526-8.
|
| 9. | Tector AJ, Amundsen S, Schmahl TM, Kress DC, Peter M. Total revascularization with T grafts. Ann Thorac Surg 1994;57:33-8.
[PUBMED] |
| 10. | Barra JA, Bezon E, Mansourati J, Rukbi I, Mondine P, Youssef Y, et al. Reimplantation of the right internal thoracic artery as a free graft into the left in situ internal thoracicartery (Y procedure). One-year angiographic results. J Thorac Cardiovasc Surg 1995;109:1042-7.
|
| 11. | Kamath ML, Matysik LS, Schmidt DH, Smith LL. Sequential internal mammary artery grafts expanded utilization of an ideal conduit. J Thorac Cardiovasc Surg 1985;89:163-9.
[PUBMED] |
| 12. | Chocron S, Etievent JP, Schiele F, Clement F, Alwan K, Cordier A, et al. The Y graft: Myocardial revascularization with both internal thoracic arteries: Evaluation of eighty cases with coronary angiographic assessment. J Thorac Cardiovasc Surg. 1994;108:736-740.
[PUBMED] |
| 13. | Tatoulis J, Buxton BF, Fuller JA, Royse AG. Total arterial coronary revascularization: Techniques and results in 3,220 patients. Ann Thorac Surg 1999;68:2093-9.
[PUBMED] |
| 14. | Lytle BW, Blackstone EH, Loop FD, Houghtaling PL, Arnold JH, Akhrass R, et al. Two internal thoracic arteries are better than one. J Thorac Cardiovasc Surg 1999;117:855-72.
|
| 15. | Lytle BW, Blackstone EH, Sabik JF, Houghtaling P, Loop FD, Cosgrove DM, et al. The Effect of Bilateral internal thoracic artery grafting on survival during 20 postoperative years. Ann Thorac Surg 2004;78:2005-14.
|
| 16. | Sung K, Lee YT, Park KH, Jun TG, Park PW, Yang JH. Beating heart revascularization using only bilateral internal thoracic arteries for triple-vessel disease: Early angiographic findings. Heart Surg Forum 2003;6:336-40.
[PUBMED] |
| 17. | Navia D, Vrancic M, Vaccarino G, Piccinini F, Raich H, Florit S, et al. Total arterial off-pump coronary revascularization using bilateral internal thoracic arteries in triple-vessel disease: Surgical technique and clinical outcomes. Ann Thorac Surg 2008;86:524-31.
[PUBMED] |
| 18. | D'Ancona G, Karamanoukian H, Ricci M, Schmid S, Bergsland J, Salerno TA. Graft revision after transit time flow measurements in off-pump coronary artery bypass grafting. Eur J Cardiothorac Surg 2000;17:287-93.
|
| 19. | Shin H, Yozu R, Mitsumaru A, Iino Y, Hashizume K, Matayoshi T, et al. Intraoperative assessment of coronary artery bypass graft: Transit-time flowmetry versus angiography. Ann Thorac Surg 2001;72:1562-5.
[PUBMED] |
| 20. | Leong DK, Ashok V, Nishkantha A, Shan YH, Sim EK. Transit-time flow measurement is essential in coronary artery bypass grafting. Ann Thorac Surg 2005;79:854-8.
[PUBMED] |
| 21. | Rizzoli G, Schiavon L, Bellini P. Does the use of bilateral internal mammary artery (IMA) grafts provide incremental benefit relative to the use of a single IMA graft? A meta-analysis approach. Eur J Cardiothorac Surg 2002;22:781-6.
[PUBMED] |
| 22. | Borger MA, Rao V, Weisel RD, Ivanov J, Cohen G, Scully HE, et al. Deep sternal wound infection: Risk factors and outcomes. Ann Thorac Surg 1998;65:1050-6.
[PUBMED] |
| 23. | Sofer D, Gurevitch J, Shapira I, Paz Y, Matsa M, Kramer A, et al. Sternal wound infection in patients after coronary artery bypass grafting using bilateral skeletonized internal mammary arteries. Ann Surg 1999;229:585-90.
[PUBMED] |
| 24. | Horii T, Suma H. Semiskeletonization of internal thoracic artery: Alternative harvest technique. Ann Thorac Surg 1997;63:867-8.
[PUBMED] |
| 25. | Tarrío RF, Cuenca JJ, Gomes V, Campos V, Herrera JM, Rodríguez F, et al. Off-pump total arterial revascularization: Our experience. J Card Surg 2004;19:389-95.
|
| 26. | Tector A, McDonald ML, Kress DC, Downey FX, Schmahl TM. Purely internal thoracic artery grafts: Outcomes. Ann Thorac Surg 2001;72:450-5.
|
| 27. | Sakaguchi G, Tadamura E, Ohnaka M, Tambara K, Nishimura K, Komeda M, et al. Composite arterial Y graft has less coronary flow reserve than independent grafts. Ann Thorac Surg 2002;74:493-6.
|
| 28. | Wendler O, Hennen B, Markwirth T, König J, Tscholl D, Huang Q, et al. T grafts with the right internal thoracic artery to the left internal thoracic artery versus the left internal thoracic and radial artery: Flow dynamics in the internal thoracic artery main stem. J Thorac Cardiovasc Surg 1999;118:841-48.
|
| 29. | Tector AJ, McDonald ML, Kress DC, Downey FX, Schmahl TM. Purely internal thoracic artery grafts: Outcomes. Ann Thorac Surg 2001;72:450-5.
|
| 30. | Wendler O, Hennen B, Demertzis S, Markwirth T, Tscholl D, Lausberg H, et al. Complete arterial revascularization in multivessel coronary artery disease with 2 conduits (skeletonized grafts and T grafts). Circulation 2000;102 (19 Suppl 3):III79-83.
|
| 31. | Nakayama Y, Sakata R, Ura M. Growth potential of left internal thoracic artery grafts: analysis of angiographic findings. Ann Thorac Surg 2001;71:142-7.
|
| 32. | Seki T, Kitamura S, Kawachi K, Morita R, Kawata T, Mizuguchi K, et al. A quantitative study of postoperative luminal narrowing of the internal thoracic artery graft in coronary artery bypass surgery. J Thorac Cardiovasc Surg 1992;104:1532-8.
|
| 33. | Markwirth T, Hennen B, Scheller B, Schäfers HJ, Wendler O. Flow wire measurements after complete arterial coronary revascularization with T-grafts. Ann Thorac Surg 2001;71:788-93.
|
| 34. | Spyrou N, Khan MA, Rosen SD, Foale R, Davies DW, Sogliani F, et al. Persistent but reversible coronary microvascular dysfunction after bypass grafting. Am J Physiol Heart Circ Physiol 2000;279:H2634-40.
|
| 35. | Kim WS, Lee J, Lee YT, Sung K, Yang JH, Jun TG, et al. Total arterial revascularization in triple-vessel disease with off-pump and aortic no-touch technique. Ann Thorac Surg 2008;86:1861-5.
|
[Table 1]
|