|


 |
| CASE REPORT |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 129-131 |
|
|
Single Incision Laparoscopic Cholecystectomy in situs Inversus Totalis
Suleyman Bozkurt1, Halil Coskun1, Tuba Atak2, Huseyin Kadioglu1
1 Department of Surgery, Faculty of Medicine, Bezmialem Vakif University, Istanbul, Turkey
2 Department of Surgery, Istanbul Medeniyet University, Goztepe Research Hospital, Istanbul, Turkey
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Suleyman Bozkurt
Tepeoren M, Istanbulpark C, Arkeon Evleri Sit, H 67, 34959 Akfirat Tuzla Istanbul, Istanbul
Turkey
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/2006-8808.110264

 Abstract Abstract | | |
Situs inversus totalis (SIT) is a rare genetic anomaly characterized by arrangement of the abdominal and thoracic organs in a perfect mirror image reversal of the normal positioning. Transposition of the organs causes difficulty in diagnosis and treatment of the diseases related to abdomen and thorax. Single incision laparoscopic surgery (SILS) is a new technique and it is increasingly used with better cosmetic results. In this paper, a single incision laparoscopic cholecystectomy (SILC) performed in a patient with SIT is presented. SILC can be performed safely in the patients with SIT with better cosmetic results. Keywords: Gallstones, single incision cholecystectomy, situs inversus totalis
How to cite this article:
Bozkurt S, Coskun H, Atak T, Kadioglu H. Single Incision Laparoscopic Cholecystectomy in situs Inversus Totalis. J Surg Tech Case Report 2012;4:129-31 |
How to cite this URL:
Bozkurt S, Coskun H, Atak T, Kadioglu H. Single Incision Laparoscopic Cholecystectomy in situs Inversus Totalis. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:129-31. Available from: http://www.jstcr.org/text.asp?2012/4/2/129/110264 |
| Introduction | |  |
Situs inversus totalis (SIT) is a rare congenital condition seen in 0.01% of the population. [1] It is characterized by the transposition of major thoracic organs and all of abdominal visceral organs to the opposite side of the body. The liver and gallbladder are located on the left side of the abdomen, while the stomach and the spleen are on the right side. Even though the etiology is not known exactly, it is thought to be due to a genetic defect occurring within the second week of embryonic life. It is seen equally in both genders. [2],[3]
Laparoscopic cholecystectomy has become the gold standard for treatment of symptomatic gallbladder calculi in late 1900s. [4] However, trend for minimizing of surgical trauma lead to development of new techniques in laparoscopic surgery. In 1997, Navara et al. performed cholecystectomy via two umbilical ports and using three-sling-sutures. [5] Since then, single incision laparoscopic surgery (SILS) entered a rapid development. It has promising advantages such as better cosmetic result and lesser postoperative pain.
In this manuscript, single incision laparoscopic cholecystectomy (SILC) performed in a case with SIT is presented.
| Case Report | | |
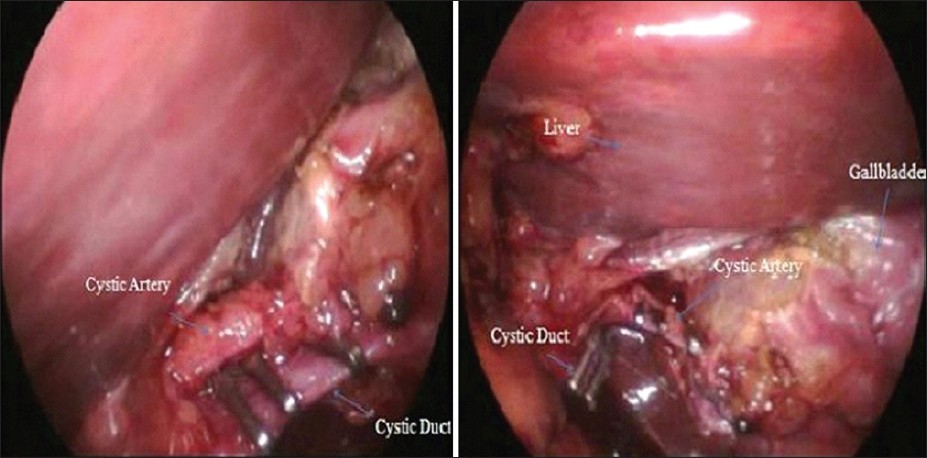
A 49-year-old man who was known to have SIT, was admitted for elective cholecystectomy due to cholelithiasis. He presented to the department of surgery with complaints of left sided pain in the hypochondrium accompanied with nausea and vomiting after meals. The electrocardiogram and chest X-rays shows signs of dextrocardia [Figure 1]. On ultrasonographic evaluation, the right lobe of the liver and gallbladder were found on the left side; the spleen was visualized on the right. The gallbladder was filled with several gallstones. The common bile duct was normal in diameter. In the operating room, the surgeon and camera assistant were positioned on the right and the laparoscopy tower on the left. A single intra-umbilical 20 mm vertical incision was made by pulling out the umbilicus. After exposing the fascia, a single port trocar (Ethicon® Single Port) was applied just through the umbilicus and pneumoperitoneum was maintained stable at 12 mm Hg with carbon dioxide. The patient was put in a reverse trendelenburg position and rotated to the right. An initial laparoscopy inspected the reversed position of all intraperitoneal viscera [Figure 1]. The gallbladder was retracted with a suture placed along the gallbladder through the left side of the abdominal wall. Reticulating devices were entered through the port. Dissection was performed using an electric cautery hook (Ethicon® Endopath® Hook Electrode) and reticulating dissector (Covidien Articulating SILS TM Dissector and SILS TM Grasper). Before clipping, meticulous dissection and complete clearance of cystic duct and cystic artery represent an essential step for a safe procedure [Figure 2]. The cystic duct and artery were separately clipped with a standard 5-mm clip applier (Ethicon® Ligaclip® ) and divided [Figure 3]. The specimen was retrieved through the umbilical incision. Finally, the 20 mm trocar site was closed with an absorbable suture and the umbilicus was restored to its physiological position. The operating time was 90 min and the procedure was completed without technical problems and complication. Patient received per os at 6 h postoperatively and was mobilized. The patient was discharged on the first day in a nice condition.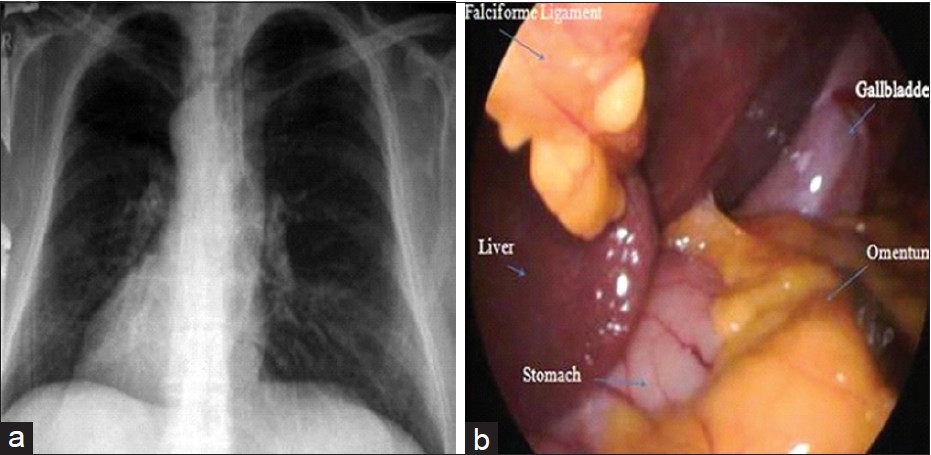 | Figure 1: (a) Plane chest X‑ray demonstrates dextrocardia and (b) laparoscopic view of situs inversus totalis
Click here to view |
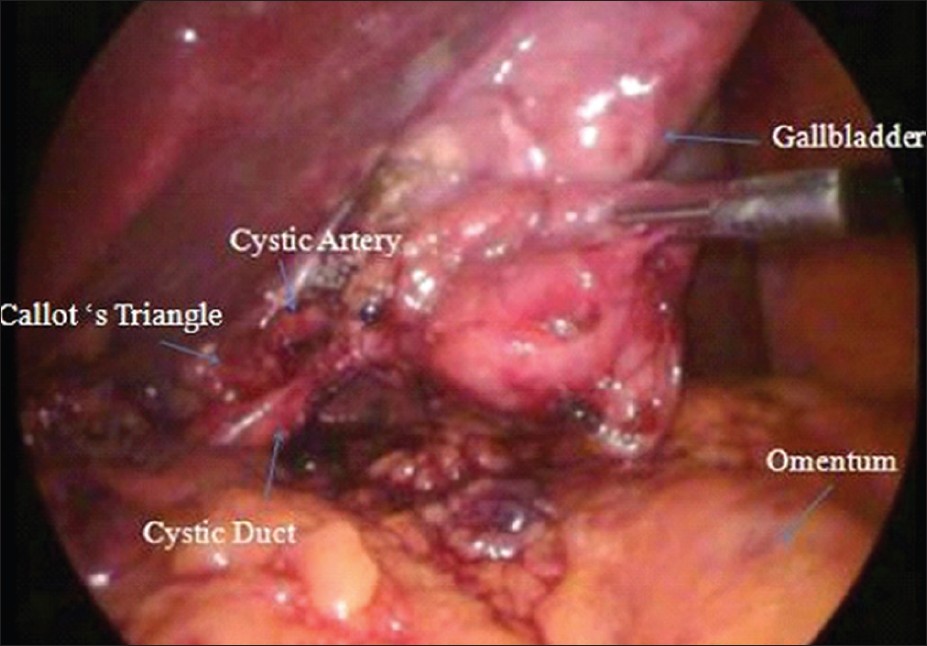 | Figure 2: Laparoscopic view of Callot's triangle after meticulous dissection
Click here to view |
| Discussion | | |
SIT is characterized by the transposition of thoracal and abdominal organs to the opposite side of the body and seen rarely. Frequently, it can be associated with many anatomic variations. When it is associated with bronchiectasis and sinusitis, it is called as Kartagener's syndrome. [2],[3],[4],[5],[6] Diagnosis can be made with physical examination, electrocardiography, chest X-ray and abdominal scanning like ultrasonography or computed tomography.
Laparoscopic cholecystectomy is one of the most frequently performed surgical procedures in surgical clinics. The method has many advantages such as better toleration by the patients, less postoperative pain, less postoperative scarring, rapid recovery and faster return to work. Surgeons went into the effort of reducing the number and size of trocars in order to increase these obvious and clear benefits of conventional laparoscopy. Natural orifice surgery and SILS emerged in this sense and they were introduced into medical practice as the newest and the least invasive surgical methods. [7] First SILS was defined in 1990s and its use is rapidly increasing today by means of new instruments and equipment developed in this area. Randomized controlled studies are warranted to compare the clinical advantages of SILS with conventional laparoscopy. Major advantage of the technique is better cosmetic results obtained in the absence of obvious abdominal scarring. The most important problem in SILS application is the difficulty, experienced by the surgeon in adaptation to new instruments. Surgeon and assistant usually interfere with each other. Some of these disadvantages of the technique can be removed by using semi-flexible camera systems and cross-angled hand devices. Despite these restrictions of SILS, we could successfully perform our operation in the case with SIT in an appropriate period.
In SILC with SIT the surgeon stood on the patient's left side and operated using standard SILS laparoscopic instruments. The fundic retraction of the gallbladder in our patient was achieved with a hanging suture to the skin, but this may also be performed with a clinch or grasper by the surgeon. We preferred to use the grasper, for retracting the Hartmann's pouch of the gallbladder, we thought that this maneuver eased the exposure of Calot's triangle and anterograde dissection. [8] The gallbladder was retracted with a grasper clasped in surgeon's left hand and dissection of cystic structures performed with a dissector with the surgeon's right hand. The challenging factor is the mirror-image anatomy of the patient which leads some or less problems with orientation and dissection. Although there is no evidence suggesting that there is increased risk of injuries in SIT patients, the surgeon should identify the whole anatomy before clipping and dissecting any structure, because, there is an increased possibility of associated biliary tract and vascular anomalies in SIT patients.
In the English-language literature we found many reports of successful laparoscopic cholecystectomy with SIT. [8],[9],[10],[11] However, reported SILC cases are scarce. [12],[13],[14] No natural orifice transluminal endoscopic surgery (NOTES) procedure for cholecystectomy in patient with SIT has reported yet. Although the single-port or single-incision procedures are cosmetically more approvable, technically they are slightly more time-consuming and more difficult and costly procedures. However, they can be performed safely in SIT patients using particular attention to the structural anatomy of the biliary field. To achieve this, surgeon has to pay attention to stand in strategic position of a patient, himself or herself and laparoscopic instruments.
In conclusion, SILC can be safely applied in the cases with SIT. Randomized controlled studies compared with conventional laparoscopy are warranted to be able to introduce the technique into routine practice.
| References | | |
| 1. | Morelli SH, Young L, Reid B, Ruttenberg H, Bamshad MJ. Clinical analysis of families with heart, midline, and laterality defects. Am J Med Genet 2001;101:388-92. 
|
| 2. | D'Agata A, Boncompagni G. Video laparoscopic cholecystectomy in situ viscerum inversus totalis. Minerva Chir 1997;52:271-5.
|
| 3. | Demetriades H, Botsios D, Dervenis C, Evagelou J, Agelopoulos S, Dadoukis J. Laparoscopic cholecystectomy in two patients with symptomatic cholelithiasis and situs inversus totalis. Dig Surg 1999;16:519-21.
|
| 4. | Jaffray B. Minimally invasive surgery. Arch Dis Child 2005;90:537-42.
|
| 5. | Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I. One-wound laparoscopic cholecystectomy. Br J Surg 1997;84:695.
|
| 6. | Kuon Lee S, You YK, Park JH, Kim HJ, Lee KK, Kim DG. Single-port transumbilical laparoscopic cholecystectomy: A preliminary study in 37 patients with gallbladder disease. J Laparoendosc Adv Surg Tech A 2009;19:495-9.
|
| 7. | Iannelli A, Schneck AS, Ioia G, Gugenheim J. Single incision laparoscopic surgery cholecystectomy: A preliminary experience. Surg Laparosc Endosc Percutan Tech 2010;20:e89-91.
|
| 8. | Han HJ, Choi SB, Kim CY, Kim WB, Song TJ, Choi SY. Single-incision multiport laparoscopic cholecystectomy for a patient with situs inversus totalis: Report of a case. Surg Today 2011;41:877-80.
|
| 9. | Iusco DR, Sacco S, Ismail I, Bonomi S, Virzì S. Three-trocar laparoscopic cholecystectomy in patient with situs viscerum inversus totalis: Case report and review of the literature. G Chir 2012;33:10-3.
|
| 10. | Pahwa HS, Kumar A, Srivastava R. Laparoscopic cholecystectomy in situs inversus: Points of technique. BMJ Case Rep 2012;2012. pii: Bcr2012006170.
|
| 11. | Borgaonkar VD, Deshpande SS, Kulkarni VV. Laparoscopic cholecystectomy and appendicectomy in situs inversus totalis: A case report and review of literature. J Minim Access Surg 2011;7:242-5.
|
| 12. | de Campos Martins MV, Pantaleão Falcão JL, Skinovsky J, de Faria GM. Single-port cholecystectomy in a patient with situs inversus totalis presenting with cholelithiasis: A case report. J Med Case Rep 2012;6:96.
|
| 13. | Uludag M, Yetkin G, Kartal A. Single-incision laparoscopic cholecystectomy in situs inversus totalis. JSLS 2011;15:239-43.
|
| 14. | Ozsoy M, Haskaraca MF, Terzioglu A. Single incision laparoscopic cholecystectomy (SILS) for a patient with situs inversus totalis. BMJ Case Rep 2011;2011. pii: Bcr0820114581.
|
[Figure 1], [Figure 2], [Figure 3]
| This article has been cited by | | 1 |
Single-incision cholecystectomy in a patient with situs inversus totalis presenting with cholelithiasis: A case report |
|
| Yoshio Deguchi,Keitaro Mitamura,Shunsuke Omotaka,Jun-ichi Eguchi,Dai Sakuma,Masashi Sato,Norihiro Nomura,Takayoshi Ito,Kevin Lawrence Grimes,Haruhiro Inoue | | Asian Journal of Endoscopic Surgery. 2015; 8(3): 347 | | [Pubmed] | [DOI] | | | 2 |
Single Fulcrum Laparoscopic Cholecystectomy in Situs Inversus Totalis |
|
| Sun Jung Kim,Jiae Park,Chang Moo Kang,Woo Jung Lee | | Journal of Minimally Invasive Surgery. 2015; 18(3): 89 | | [Pubmed] | [DOI] | |
|




 |
|
|
|