|


 |
| CASE REPORT |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 135-137 |
|
|
Spontaneous Epidural Haematoma in Sickle Cell Anaemia: Case Report and Literature Review
Bankole O Babatola1, Yusuf A Salman2, Asha M Abiola1, Kanu O Okezie1, Arigbabu S Oladele1
1 Department of Surgery, Neurosurgery Unit, Lagos University Teaching Hospital, Idi Araba, Lagos, Nigeria
2 Department of Surgery, University of Ilorin Teaching Hospital, Ilorin, Nigeria
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Yusuf A Salman
Department of Surgery, Neurosurgery Unit, University of Ilorin Teaching Hospital, Ilorin
Nigeria
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.110271

 Abstract Abstract | | |
Non traumatic spontaneous epidural Haematoma is a rare and often unmentioned complication of sickle cell disease. It is often associated with skull bone infarction. We report an eighteen year old boy with sickle cell anaemia who developed persistence headache during a vaso-occlusive crisis. Brain computed tomography (CT) revealed a right frontal epidural Haematoma (EDH) compressing on the brain. No other etiologic factor was identified. A right frontal craniotomy and evacuation of the Haematoma was performed and he made good recovery. The possible pathogeneses of this rare condition are discussed. Keywords: Computed tomography, craniotomy, sickle cell anaemia, spontaneous epidural Haematoma
How to cite this article:
Babatola BO, Salman YA, Abiola AM, Okezie KO, Oladele AS. Spontaneous Epidural Haematoma in Sickle Cell Anaemia: Case Report and Literature Review. J Surg Tech Case Report 2012;4:135-7 |
How to cite this URL:
Babatola BO, Salman YA, Abiola AM, Okezie KO, Oladele AS. Spontaneous Epidural Haematoma in Sickle Cell Anaemia: Case Report and Literature Review. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:135-7. Available from: http://www.jstcr.org/text.asp?2012/4/2/135/110271 |
| Introduction | |  |
Spontaneous intracranial epidural Haematoma (EDH) is a rare complication of sickle cell anaemia (SCA). Twelve cases have been reported previously. An association with vaso-occlusive crises [1],[2],[3] and skull infarction. [4],[5],[6],[7],[8] were observed in the few reported cases. With no history of head trauma the pathogenesis of spontaneous EDH in patients with sickle cell anaemia is still not clearly defined. Non traumatic spontaneous EDH has also been reported in association with other clinical conditions like coagulopathies, [8] infectious diseases of the skull like sinusitis, [9],[10] vascular malformations of the dura mater and metastasis to the dural, [11] or skull, [12] and chronic kidney disease. [13] This is a case of a young man with SCA (Haemoglobin SS, HbSS) with non traumatic spontaneous intracranial EDH following a vaso-occlusive crisis that was successfully managed with craniotomy and evacuation of Haematoma without any undesirable sequel.
| Case Report | | |
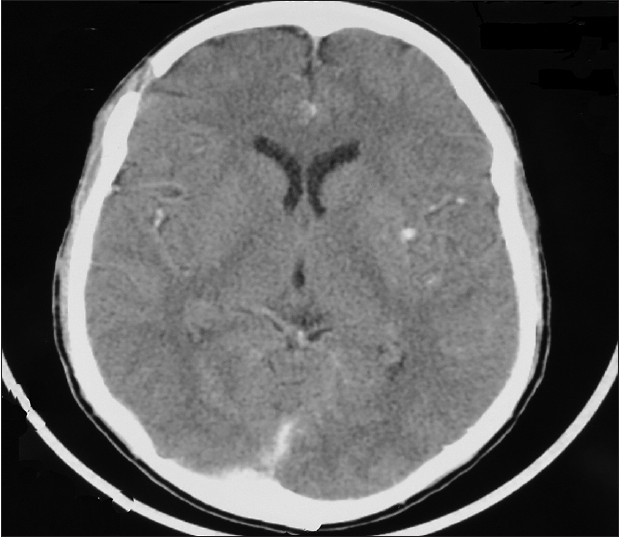
We report a case of an 18-year-old boy with sickle cell anaemia (HbSS). He presented to our unit with seven days history of frontal headache which was preceded by an episode of vaso-occlusive crisis necessitating admission and blood transfusion in a peripheral hospital. There was no history of trauma or altered consciousness. The patient was fully conscious, pale and icteric but not febrile. There was no local evidence of head trauma and no neurologic signs. Coagulation studies results were within normal limit. His packed cell volume on admission was 19%. A computerized tomography (CT) scan of the brain done due to non resolution of headache revealed a right frontal hyper dense biconvex epidural lesion compressing the underlying brain suggestive of EDH. There was no skull fracture, osteomyelitis or CT scan evidence of brain infarction [Figure 1]. The patient underwent a right frontal craniotomy and evacuation of EDH under general endotracheal anaesthesia. Intraoperatively, the skull appeared grossly normal and the patient had an uneventful postoperative recovery with complete resolution of headache. He was discharged after 11 days of hospital admission. He has remained symptom free 2 years post operatively. Post operative CT scan showed complete evacuation of Haematoma [Figure 2]. | Figure 1: Brain computed tomography scan showing right frontal acute epidural Haematoma
Click here to view |
 | Figure 2: Post operative computed tomography scan showing complete evacuation of Haematoma
Click here to view |
| Discussion | | |
Epidural Haematoma is collection of blood between the calvaria and the dura. It is almost always caused by head trauma associated with skull fracture. Haematoma occurs as a result of bleeding from ruptured middle meningeal vessels or diploic veins. Spontaneous EDH is rarely reported in literature and its incidence is not known. Spontaneous EDH in a patient with sickle cell disease (SCD) represents a rare and frequently unmentioned complication of this haemoglobinopathy. In this category of patients, typically there is no evidence of head trauma, cephalhaematoma or skull fracture. The clinical presentation of EDH in SCD patients is different from the classic description of post traumatic EDH which usually is characterized by a lucid interval. A high index of suspicion is needed for prompt diagnosis and treatment of this rare complication of SCD. Spontaneous EDH in patients with HbSS often occurred along with skull infarction. [1],[4],[5],[6],[7],[8] However, the pathogenesis has not been fully elucidated. At least three pathophysiologic mechanisms have been proposed. The frequent concurrence of skull infarctions along with spontaneous intracranial epidural Haematoma has been noted to suggest a mechanism whereby infarction of the skull leads to periosteal elevation, disruption of the cortical bone margin, and bleeding into the epidural space. [5] Another theory proposes that insufficient venous drainage is the inciting event that leads to oedema and haemorrhage. [1] In spontaneous EDH not associated with skull infarction, the patients' skull is said to have abnormal anatomy because of a pathological process of chronic medullary haematopoiesis. The proliferation of this hematopoietic skull tissue with resultant expansion in response to acute anaemia results in the expanding hematopoietic tissue disrupting the inner and outer skull margins and precipitating extravasations of blood and hematopoietic tissue into the subgaleal and epidural spaces. [2] Our patient presented with persistent headache which started a day after blood transfusion during a vaso-occlusive crisis, there was no evidence of skull infarction on CT scan and the skull looked normal during craniotomy. The exact cause of the EDH in our patient remains unclear. However as noted by Nader, the violation of the cortical bone margin resulting in extravasations of blood into epidural space in our patient might have occurred at microscopic level. [2] Further research into the pathogenesis of spontaneous EDH in sickle cell disease is required. Unlike spontaneous EDH associated with sinus infection, an infective process is a remote possibility in the pathogenesis of spontaneous intracranial EDH in patients with SCD.
Despite the background haemoglobinopathy, this patient successfully underwent standard craniotomy and evacuation of EDH under general endotracheal anaesthesia with complete resolution of symptom and no undesirable complication. Two patients with small EDH were managed conservatively in earlier reports with radiological evidence of Haematoma resolution. [1],[7] However, surgical evacuation remains the standard of treatment for this condition and the presence of sickle cell haemoglobinopathy should not serve as a contraindication.
A search of English literature on spontaneous intracranial EDH in sickle cell disease yielded a total of 12 patients; 10 patients with HbSS, [1],[2],[3],[4],[5],[6],[8] 1 patient with HbSC, [7] and 1 patient with HbS with β-thalasemia. [6] Our patient is the first to be reported in Nigeria despite the high prevalence of SCD in the Nigerian population. [14] This may be because CT scan machines are just becoming widely available and affordable to many patients in the country. A high index of suspicion is required among clinicians to make prompt diagnosis of this rare condition. Any SCD patient with symptoms and signs of raised intracranial pressure (ICP) should be referred for cranial CT scan which will diagnose EDH in all cases where it is present.
| Conclusion | | |
Spontaneous EDH is a rare occurrence; its occurrence in SCD patients is rarer still. A high index of suspicion is required in the diagnosis and treatment of EDH in patient with sickle cell anaemia. Operative management is associated with excellent outcomes as demonstrated in our index patient.
| References | | |
| 1. | Kalala Okito JP, Van Damme O, Calliauw L. Are spontaneous epidural haematoma in sickle cell disease a rare complication? A report of two new cases. Acta Neurochir (Wien) 2004;146:407-10. 
|
| 2. | Dahdaleh NS, Lindley TE, Kirby PA, Oya H, Howard MA 3 rd . A "neurosurgical crisis" of sickle cell disease. J Neurosurg Pediatr 2009;4:532-5.
|
| 3. | Naran AD, Fontana L. Sickle cell disease with orbital infarction and epidural hematoma. Pediatr Radiol 2001;31:257-9.
|
| 4. | Karacostas D, Artemis N, Papadopoulou M, Christakis J. Case report: Epidural and bilateral retroorbital hematomas complicating sickle cell anemia. Am J Med Sci 1991;302:107-9.
|
| 5. | Resar LM, Oliva MM, Casella JF. Skull infarction and epidural hematomas in a patient with sickle cell anemia. J Pediatr Hematol Oncol 1996;18:413-5.
|
| 6. | Ganesh A, Al-Zuhaibi S, Pathare A, William R, Al-Senawi R, Al-Mujaini A, et al. Orbital infarction in sickle cell disease. Am J Ophthalmol 2008;146:595-601.
|
| 7. | Arends S, Coebergh JA, Kerkhoffs JL, Van Gils A, Koppen H. Severe unilateral headache caused by skull bone infarction with epidural haematoma in a patient with sickle cell disease. Cephalalgia 2011;31:1325-8.
|
| 8. | Ng WH, Yeo TT, Seow WT. Non-traumatic spontaneous acute epidural haematoma-report of two cases and review of the literature. J Clin Neurosci 2004;11:791-3.
|
| 9. | Takahashi Y, Hashimoto N, Hino A. Spontaneous epidural hematoma secondary to sphenoid sinusitis: Case report. Neurol Med Chir (Tokyo) 2010;50:399-401.
|
| 10. | Chaiyasate S, Halewyck S, Van Rompaey K, Clement P. Spontaneous extradural hematoma as a presentation of sinusitis: Case report and literature review. Int J Pediatr Otorhinolaryngol 2007;71:827-30.
|
| 11. | Hassan MF, Dhamija B, Palmer JD, Hilton D, Adams W. Spontaneous cranial extradural hematoma: Case report and review of literature. Neuropathology 2009;29:480-4.
|
| 12. | Kim BG, Yoon SM, Bae HG, Yun IG. Spontaneous intracranial epidural hematoma originating from dural metastasis of hepatocellular carcinoma. J Korean Neurosurg Soc 2010;48:166-9.
|
| 13. | Zheng FX, Chao Y. Spontaneous intracranial extradural hematoma: Case report and literature review. Neurol India 2009;57:324-6.
[PUBMED]  |
| 14. | Akinyanju OO. A profile of sickle cell disease in Nigeria . Ann N Y Acad Sci 1989;565:126-36.
|
[Figure 1], [Figure 2]
|
















