|


 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 5
| Issue : 1 | Page : 56-57 |
|
|
Carcinoid tumor in accidental, asymptomatic Meckel's diverticulum
Zsolt Baranyai1, Valeria Jósa2, Keresztely Merkel3, Zsofia Zolnai4
1 Department of Surgery, United Szent István and Szent László Hospital; Department of Tissue Preservation, Tumorgenetika, Human Biospecimen Collection and Research, Budapest, Hungary
2 Department of Tissue Preservation, Tumorgenetika, Human Biospecimen Collection and Research, Budapest, Hungary
3 Department of Surgery, United Szent István and Szent László Hospital, Budapest, Hungary
4 Department of Pathology, Szent Imre Hospital, Budapest, Hungary
| Date of Web Publication | 21-Sep-2013 |
Correspondence Address:
Zsolt Baranyai
Kerékgyártó Street 36 38, Budapest, 1147
Hungary
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.118633

 Abstract Abstract | | |
Although Meckel's diverticulum is the most common congenital gastrointestinal disorder, it is controversial whether asymptomatic diverticula in adults should be respected. The authors report the case of a patient who was operated due to ileus caused by adhesions and a Meckel's diverticulum without any sign of inflammation was accidentally noted and removed. As a surprise, the pathological examination of the diverticulum proved carcinoid tumor, a neuroendocrine malignant tumor. The case raises the importance of the removal of asymptomatic Meckel's diverticulum. Keywords: Carcinoid tumor, ileus, Meckel′s diverticulum
How to cite this article:
Baranyai Z, Jósa V, Merkel K, Zolnai Z. Carcinoid tumor in accidental, asymptomatic Meckel's diverticulum. J Surg Tech Case Report 2013;5:56-7 |
How to cite this URL:
Baranyai Z, Jósa V, Merkel K, Zolnai Z. Carcinoid tumor in accidental, asymptomatic Meckel's diverticulum. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:56-7. Available from: http://www.jstcr.org/text.asp?2013/5/1/56/118633 |
| Introduction | |  |
Meckel's diverticulum is a very rare localization for neuroendocrine tumors, including carcinoid tumors. [1] We have found no report in the literature where it was found accidentally. Carcinoid tumors in the gastrointestinal tract arise from amine precursor uptake and decarboxylation cells with neuroendocrine origin. They often infiltrate the peritoneum locally, but their direct spread is uncommon. They metastasize at first to local lymph nodes, followed by the liver. However, the typical clinical picture of carcinoid syndrome is only present if hepatic metastasis has already developed. The treatment of choice is basically surgical that is defined by the size of the primary tumor and the presence of metastases. If the tumor is smaller than 1 cm and no invasive spread or metastasis is noted local excision can be satisfactory. In other cases, radical operation is recommended and the resection should be performed 10 cm orally and distally from the tumor. In case of a carcinoid tumor occurring in the terminal ileum right hemicolectomy is the therapy of choice. The palliative resection of the tumor tissue with additional symptomatic and cytostatic therapy can contribute to the relief of the symptoms of carcinoid syndrome.
| Case report | | |
A 75-year-old female patient had a history of appendicectomy. Following blunt abdominal injury she was admitted due to lack of bowel movements, abdominal cramps, pain, distension and vomiting. Ileus of the small bowels was established as the underlying cause of her complaints and urgent operation was performed. During abdominal exploration adhesions were found on an approximately, 15 cm section of the terminal ileum and adhesiolysis was carried out. During the operation, Meckel's diverticulum without any sign of inflammation was found and wedge excision was performed. No ectopic tissue could be palpated intraoperatively. Patient passed a smooth post-operative period and the bowel movements returned post-operatively and she was discharged with no complaints.
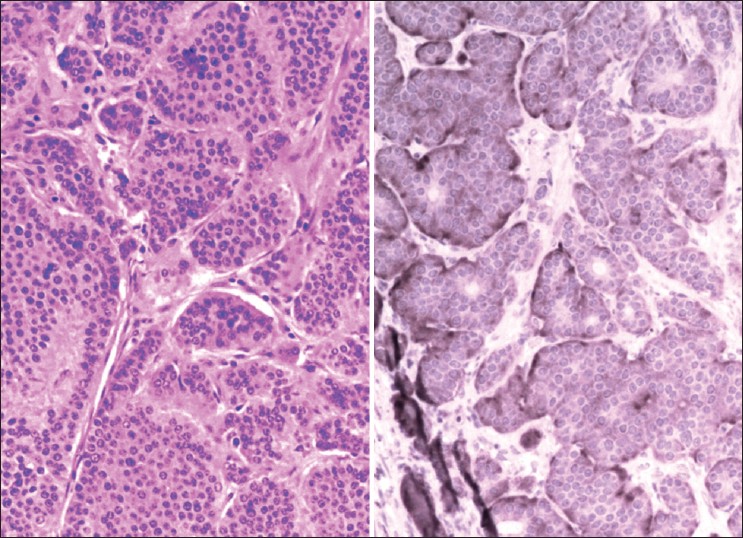
Pathological work-up of the resected Meckel's diverticulum revealed ectopic tissue in addition to the small bowel, mucosa and gastric glands were found. However, a well-circumscribed lesion of 0.5 cm was also detected that was well-distinguishable from the adjacent tissues. It infiltrated the muscle layer of the bowel, but no further layers were involved. The round, cuboidal cells built up nests and fascicles in the involved area. The nuclei were centrally located the chromatin was finely granulated. Immunohistochemical studies were also performed that proved the suspected diagnosis of carcinoid tumor. They were positive for synaptophysin, but negative for chromogranine, cytokeratin (CK) 7 and CK20. No vascular or lymphatic invasion was found and no abnormal lymph node could be detected. The final diagnosis was neuroendocrine carcinoma of Meckel's diverticulum based on the pathological finding [Figure 1]. Patient has been followed-up by oncologists since the operation.
| Discussion | | |
The majority of Meckel's diverticulum remains asymptomatic throughout life. In general, they are discovered accidentally during the laparotomy or laparoscopy. The main complications it can lead to are bleeding, ulceration, perforation, ileus or intussusception. Diverticulitis occurs in 10-20% of the cases. [2] The removal of asymptomatic Meckel's diverticulum in adults is controversial that is in contrast to childhood when the resection is recommended by most authors. [3],[4]
Soltero and Bill reported 800 diverticulectomies. [5] They do not recommend the resection of Meckel's diverticulum because the complication rate of the intervention can reach 8%, including 1.2% mortality rate. It exceeds the lifelong risk of 2-4% to develop complication due to Meckel's diverticulum. Therefore, Dumper et al. [6] suggest deciding about resection individually by each patient. At younger age, in case of visible or palpable abnormal lesions in the Meckel's diverticulum or in symptomatic cases such as hemorrhage or ileus resection is recommended.
Other authors prefer resection even in asymptomatic Meckel's diverticulum. They report only a rate of 2% of post-operative complications and 0% mortality rate following diverticulectomy. [7] Zingg suggests diverticulectomy both in symptomatic and accidental Meckel's diverticulum as complications related to the Meckel's diverticulum itself exceed the morbidity rate after its removal. [8]
Cullen et al. [3] reported a similar experience and has stated that the incidence of complications caused by Meckel's diverticulum decreases with age and the benefits of diverticulectomy due to accidental Meckel's diverticulum exceed the accompanying morbidity and mortality. In addition, Romano et al. [9] recommends the resection of Meckel's diverticula due to the risk of malignant transformation.
| Conclusion | | |
There is still debate about the recommendation whether asymptomatic Meckel's diverticulum should be removed if found accidentally. Although no definite recommendation can be formed based on one case, our example rather supports the opinion that it is worth to perform resection also in asymptomatic cases. The diverticulectomy cannot only prevent the complications potentially occurring throughout life, but it can also reveal malignant transformation. The present surgical techniques, especially the spreading of laparoscopy decreases the risk of post-operative complications.
| References | | |
| 1. | Modlin IM, Shapiro MD, Kidd M. An analysis of rare carcinoid tumors: Clarifying these clinical conundrums. World J Surg 2005;29:92-101. 
[PUBMED] |
| 2. | Longo WE, Vernava AM 3 rd . Clinical implications of jejunoileal diverticular disease. Dis Colon Rectum 1992;35:381-8.
|
| 3. | Cullen JJ, Kelly KA, Moir CR, Hodge DO, Zinsmeister AR, Melton LJ 3 rd . Surgical management of Meckel's diverticulum. An epidemiologic, population-based study. Ann Surg 1994;220:564-8.
|
| 4. | St-Vil D, Brandt ML, Panic S, Bensoussan AL, Blanchard H. Meckel's diverticulum in children: A 20-year review. J Pediatr Surg 1991;26:1289-92.
[PUBMED] |
| 5. | Soltero MJ, Bill AH. The natural history of Meckel's Diverticulum and its relation to incidental removal. A study of 202 cases of diseased Meckel's Diverticulum found in King County, Washington, over a fifteen year period. Am J Surg 1976;132:168-73.
[PUBMED] |
| 6. | Dumper J, Mackenzie S, Mitchell P, Sutherland F, Quan ML, Mew D. Complications of Meckel's diverticula in adults. Can J Surg 2006;49:353-7.
[PUBMED] |
| 7. | Yahchouchy EK, Marano AF, Etienne JC, Fingerhut AL. Meckel's diverticulum. J Am Coll Surg 2001;192:658-62.
[PUBMED] |
| 8. | Zingg U, Vorburger S, Metzger U. Perforation of Meckel's diverticulum by a toothpick. Chirurg 2000;71:841-3.
[PUBMED] |
| 9. | Romano F, Franciosi C, Cerea K, Bravo AF, Colombo G, Isimbaldi G, et al. A case of carcinoid of Meckel's diverticulum associated with gastric adenocarcinoma. Tumori 2001;87:272-5.
|
[Figure 1]
|