|


 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 5
| Issue : 2 | Page : 106-108 |
|
|
Clinicoradiological diagnosis of cough-induced intercostal hernia
Andrew Dobradin, Jessica Bello
Department of Surgery, Winter Park Memorial Hospital, Winter Park, Florida, USA
| Date of Web Publication | 13-Mar-2014 |
Correspondence Address:
Andrew Dobradin
320 North Edinburgh Drive, Suite B, Winter Park, Florida 32792
USA
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.128754

 Abstract Abstract | | |
Cough-induced intercostal hernias without any type of external trauma are very uncommon. There have been less than 10 cases documented in literature. This clinical report describes a 66-year-old male who developed an intercostal hernia induced by a severe cough due to bilateral pneumonia and a subsequent rib fracture. It took almost a full year to diagnose this patient's chest wall mass. Only after taking careful history and reviewing all the images, the diagnosis of intercostal hernia was made. He was referred to a cardiothoracic surgeon for treatment. Intercostal hernias can be caused by the sheer exertion of coughing without any prior history of trauma to the chest wall or abdomen. Early diagnosis is difficult and had to be based on clinical signs and symptoms. The imaging studies might help to establish diagnosis, but cannot replace a diligent examination and clinical interview. The treatment of the chest wall defect is case dependent. Surgical repair reinforcement of the intercostal muscles might be required with prosthetic nonabsorbable (polypropylene) mesh. Keywords: Chest wall hernia, cough induced hernia, intercostal hernia, pneumonia, rib fracture
How to cite this article:
Dobradin A, Bello J. Clinicoradiological diagnosis of cough-induced intercostal hernia. J Surg Tech Case Report 2013;5:106-8 |
How to cite this URL:
Dobradin A, Bello J. Clinicoradiological diagnosis of cough-induced intercostal hernia. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:106-8. Available from: http://www.jstcr.org/text.asp?2013/5/2/106/128754 |
| Introduction | |  |
Cough-induced intercostal hernias are rarity in the medical field. Most of them are secondary to trauma of abdomen or chest wall. [1] We report a 66-year-old man who struggled with a painless left-sided chest mass for almost a year without an established diagnosis. Prior to this report only eight other cases have been documented in literature of an intercostal hernia being induced by coughing or other source of increase in positive pressure in the chest wall cavity. [2]
| Case Report | | |
A 66-year-old male presented to the clinic with an 11-month history of a painless enlarging mass on the left side of his chest wall. The patient noticed the mass after being discharged after a weeklong hospitalization for bilateral pneumonia. During that week the patient was continuously coughing and developed a pain in the left side of chest wall. Chest X-ray and computed tomography of the abdomen imaging showed no rib fracture or other type of injury to the chest wall, diaphragm, or abdominal wall. Discharge diagnosis included pneumonia and back pain. A few months later the patient found the mass on the left side of chest wall enlarging and decided to seek medical reevaluation by his primary care physician. He was later referred for another CT of his abdomen with intravenous contrast. This study report stated: "Patient developed a fracture with some displacement in the left posterior lateral eighth rib. The ribs more cephalad could be fractured as well. Associated with this finding there is some distortion of the ribs caudal to this left eighth rib fracture. Those ribs are displaced medially and there is bulging of the fat of the peritoneal cavity laterally without evidence of an actual hernia" [Figure 1]. The images were not conclusive for an intercostal hernia. A few more months past and the patient returned to the primary care physician with the same complaint of the chest wall mass. Additional CT of the abdomen was performed, and it showed the eighth rib fracture, the torn intercostal muscles, and no diaphragmatic defect [Figure 2].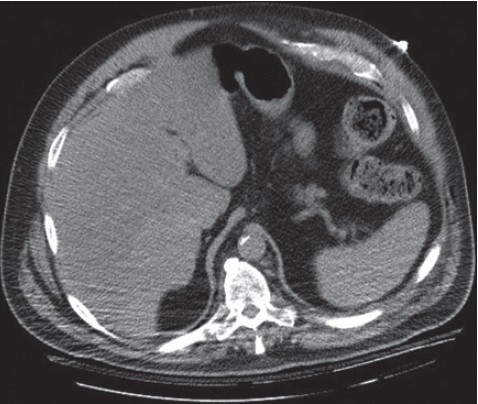 | Figure 1: Computed tomography (CT) of abdomen during hospitalization for bilateral pneumonia is not showing any evidence of the chest wall hernia
Click here to view |
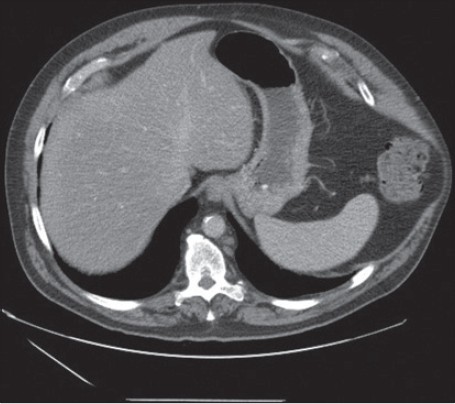 | Figure 2: CT of abdomen 10 months after hospital discharge shows left side chest wall hernia through the torn intercostal muscles
Click here to view |
Physical examination revealed an obese patient who had a soft, nontender, reducible mass on the lateral aspect (midclavicular line to the midaxillary line) of the left-sided chest wall between eighth and 11 th ribs. The mass measured 12 cm in diameter. Sensation over the mass was decreased slightly when compared to the right side.
His past medical history was significant for hyperlipidemia, hypertension, and benign prostatic hyperplasia. The patient had no history of any external trauma, no history of any rib fractures, and no lung disease other than the recent pneumonia. Patient denied any current tobacco use (quit 25 years earlier), patient occasionally used alcohol, and denied any illicit drug use.
After reviewing the CT scans and examining the patient, a diagnosis of a chest wall hernia induced by severe coughing was established. The patient was referred to a cardiothoracic surgeon to repair the hernia.
| Discussion | | |
Chest wall intercostal hernia is not seen very often. Its etiology is acquired or congenital. It can be acquired from either external or internal trauma. External trauma has been most commonly associated with intercostal hernia. [1] External trauma can be penetrating or blunt and most resulting in fracture of ribs. [1],[3],[4] The surgical causes of the intercostal hernia include lumbar incision for kidney surgery, open lung biopsy, rib resection, tube thoracostomy, and harvesting of internal mammary artery. [1] The presented patient denied any external trauma.There is also spontaneous herniation that may occur in the presence of the local impairment of the thoracic wall with associated increased intrathoracic pressure. [3] External trauma has been known to contribute to diaphragmatic injury as well. This can lead to herniation of the abdominal components. This type of herniation (transdiaphragmatic intercostal hernia) is rare with less than 40 cases documented. [3]
Intercostal hernias may develop either acutely or over a number of years. Intercostal muscles can tear or underlying ribs can even fracture after severe chronic coughing. The intra-abdominal and intrathoracic positive pressure that occurs with every expiration, act of defecation, and in times of coughing or vomiting forces the content of abdominal and chest cavity out through the weakened areas of the chest wall. [2],[4]
Intercostal hernias without any external trauma are rare. An intercostal hernia secondary to coughing developed by our patient is very unique. There have been only eight previous cases of cough-induced chest wall hernia documented prior to our report. [2]
The first case was reported in 1970. The patient was a prisoner of war 25 years earlier in Poland and developed pneumonia with a severe cough. The patient noticed a pain in his lower ribcage area and a few days later felt a mass that was diagnosed as a hernia. [2] All other cases that were reported showed increase in positive intrathoracic pressure (coughing or vomiting), whether it was chronic or acute, and no history of trauma. Coughing can be associated with many complications of which rib stress fracture is one most frequently documented complication. [5] Typical locations of rib fractures are between the fifth and the ninth rib at the lateral aspect of the rib cage. These fractures are caused by opposing muscular forces in the middle of the rib at the axillary line from the serratus anterior and external oblique muscles. [4] Fifty-nine percent of intercostal hernia cases were reported to be found at the ninth intercostal interspace. [4]
The chest wall is weak from the costochondral junction to the sternum because of lack of external intercostal muscle support and from the costal angle posteriorly to the vertebrae because of lack of internal intercostal musculature. Defects in this area can lead to separation of the ribs and the development of a potentially weakened space that is vulnerable to the development of a hernia. [4]
The diagnosis of intercostal hernia can be made by finding a palpable defect of the thoracic wall through which a reducible soft tissue mass can appear. The contents can be ascertained by observing that the containing lung varies in size paradoxically with respiration and can increase with Valsalva maneuver. An increase in hernia size with inspiration and a decrease with expiration occur when there is a diaphragmatic injury with prolapse of abdominal viscera into the thorax and out through the chest wall defect. The chest radiograph may reveal divergent ribs with bowel gas shadows beyond the confines and the abdominal cavity. CT scan frequently confirms the diagnosis. [6] The initial imaging studies were however inconclusive in this case.
Treatment of intercostal hernia is individually tailored to the patient needs because of its rarity and variability. Surgical treatment is recommended for each case. [7] It can depend on whether it happens in an acute or chronic setting. Possible associated diaphragmatic damage or rupture has to be always taken under careful consideration. In an acute setting, patient would be taken to the operating room for an exploratory laparotomy to repair the diaphragmatic defect. The common approach to treatment is to reduce the chest wall hernia and suture the defect, with the ribs approximation. That has been known to cause recurrence and because of this, reinforcement with prosthetic mesh may be preferred. [2]
| Conclusion | | |
Cough-induced intercostal hernia is a rare clinical condition. The initial imaging studies frequently are inconclusive. High positive intrathoracic pressure secondary to bilateral pneumonia can contribute to subsequent rib fracture and later cause formation of a hernia through the ruptured intercostal muscles. In cases of chest wall masses caused by internal or external trauma, serial imaging studies may be necessary to confirm the diagnosis of the hernia.
| References | | |
| 1. | Khan Z. Acquired spontaneous intercostal hernia. Pak J Surg 2007;23:223-25. 
|
| 2. | Connery A, Mutvalli E. Cough-induced abdominal intercostal hernia. JRSM Short Rep 2010;23:1-3.
|
| 3. | Sarkar D, Warta M, Solomon J. Transdiaphragmatic Intercostal Herniation following Blunt Trauma. Case Rep Radiol 2012;2012:502765.
|
| 4. | Unlu E, Temizoz O, Cagli B. Acquired spontaneous intercostal abdominal hernia: Case report and a comprehensive review of the world literature. Australas Radiol 2007;51:163-7.
|
| 5. | Hillernbrand A, Henne-Bruns D, Wurl P. Cough induced rib fracture, rupture of the diaphragm and abdominal herniation. World J Emerg Surg 2006;1:34.
|
| 6. | Khan AS, Bakhshi GD, Khan AA, Kerkar PB, Chavan PR, Sarangi S. Transdiaphragmatic intercostal hernia due to chronic cough. Indian J Gastroentrol 2006;25;92-3.
|
| 7. | Sloth-Nielsen J, Jurik AG. Spontaneous intercostal pulmonary hernia with subsegmental incarceration. Eur J Cardiothorac Surg 1989;3:562-4.
|
[Figure 1], [Figure 2]
|















