|


 |
| SURGICAL TECHNIQUE |
|
| Year : 2014 | Volume
: 6
| Issue : 1 | Page : 12-14 |
|
|
Esthetic management of gingival lesions in anterior maxilla: The role of VIP-CT Flap, a technical note
Amin Rahpeyma1, Saeedeh Khajehahmadi2
1 Associate Professor of Oral and Maxillofacial Surgery, School of Dentistry, Oral and Maxillofacial Diseases Research Center, Mashhad, Iran
2 Assistant Professor of Oral and Maxillofacial Pathology, Dental Research Center, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran
| Date of Web Publication | 24-Jun-2014 |
Correspondence Address:
Saeedeh Khajehahmadi
Dental Research Center of Mashhad University of Medical Sciences, Vakilabad Blvd, Mashhad
Iran
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.135137

 Abstract Abstract | | |
Purpose: Anterior maxilla is a high esthetic demand region. Reconstruction of the soft tissue loss after pathologic resection needs special techniques. Materials and Methods: This article describes the novel use of vascularized interpositional periosteal connective tissue flap of palate (VIP-CT) for reconstruction after resection of long-lasting pyogenic granuloma in anterior maxilla with underlying bone resorption in interdental region. Results: Good esthetic results both in labial gingiva and interdental region were obtained. Conclusion: VIP-CT flap is an ideal option for reconstruction of the pathologic lesions that affect the anterior maxilla and create pathologic space in interdental region. Keywords: Anterior maxilla, Pyogenic granuloma, VIP-CT flap
How to cite this article:
Rahpeyma A, Khajehahmadi S. Esthetic management of gingival lesions in anterior maxilla: The role of VIP-CT Flap, a technical note. J Surg Tech Case Report 2014;6:12-4 |
How to cite this URL:
Rahpeyma A, Khajehahmadi S. Esthetic management of gingival lesions in anterior maxilla: The role of VIP-CT Flap, a technical note. J Surg Tech Case Report [serial online] 2014 [cited 2016 May 10];6:12-4. Available from: http://www.jstcr.org/text.asp?2014/6/1/12/135137 |
| Introduction | |  |
Treatment of soft tissue pathologic process that affects the gingiva, especially in anterior maxilla, is a challenge. There is need for resection of the lesion and simultaneous reconstruction. [1] In long-standing neglected lesions, underlying bone resorption and pathologic tooth flaring are the other complications. [2] Excisional biopsy of the pathology responsible for gingival overgrowth will lead to unsightly gingival defect. [3] Vascularized interpositional periosteal connective tissue flap (VIP-CT) is introduced for reconstruction of the lost tissues in such situations.
| Materials and methods | | |
This article describes the novel use of VIP-CT of palate for reconstruction after resection of long-lasting pyogenic granuloma in anterior maxilla with underlying bone resorption in interdental region.The patient was a 25-year-old female patient with an exophytic mass in anterior maxilla, palatal to the dental arch with extension to the labial gingiva. During the pregnancy, it appeared and after that, it does not resolve (6-month duration). The interdental bony septum was affected and the bone level in this region had been reduced. The maxillary left central incisor had been extruded one millimeter in labial and incisal direction [Figure 1]. | Figure 1: Exophytic mass in anterior maxilla, palatal to the dental arch with labial and interdental extension
Click here to view |
The lesion had stalk in interdental and palatal gingiva which excised down to the bone under local anesthesia [Figure 2]. The resulted gingival defect was reconstructed with VIP-CT flap [Figure 3]. The pathologist report was pyogenic granuloma [Figure 4]. Finally, the patient was referred to the orthodontist. | Figure 2: The raw bone in interdental space and residual soft tissue defect in palatal and labial aspects
Click here to view |
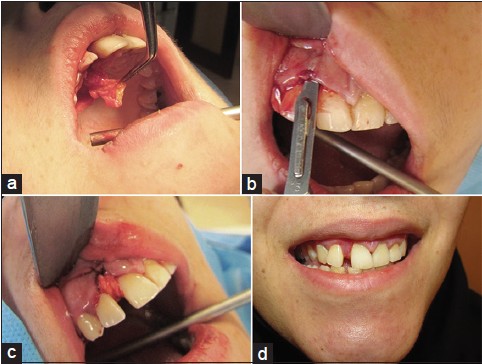 | Figure 3: (a) VIP-CT flap from the palate. (b) Supraperiosteal sharp dissection in labial region (pouch technique). (c) The flap was stabilized with 5-0 non resorbable sutures. (d) Healthy and esthetic gingiva four weeks after operation
Click here to view |
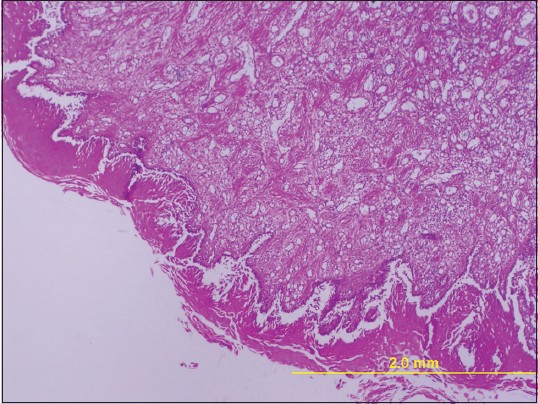 | Figure 4: Histopathologic feature showing a proliferation of fibroblast with numerous of capillary
Click here to view |
| Results | | |
Good esthetic results both in labial gingiva and interdental region were obtained.
| Discussion | | |
Palatal connective tissue as a free graft is a useful aid for soft tissue augmentation. It has applications in root coverage, filling small contour deformities of edentulous ridge, and as a biologic membrane in apical surgery. [4],[5],[6]
For esthetic treatment of gingival lesions in anterior maxilla, it is used successfully when the mucosal demand is small and limited to the gingival free margin. [7],[8] If free margin and attached gingiva are affected by the lesion, then lateral sliding flap is indicated. If the pathologic process involves the interdental papilla and effects on the underlying bone, then the adjacent teeth always move in labial and incisal direction and a considerable space occurs in the region occupied by the stalk of the lesion. Removing the exophytic mass without reconstruction had negative esthetic results such as black space, exposed root surface, and root hypersensitivity. [9]
VIP-CT flap is a well-nourished anteriorly pediculated connective tissue flap from palate. It is mainly used for coverage of small bone grafts in anterior maxilla. [10]
For esthetic management of gingival lesions when there is interdental space resulting from pathologic tooth migration and bone resorption, it is an ideal option [Figure 5].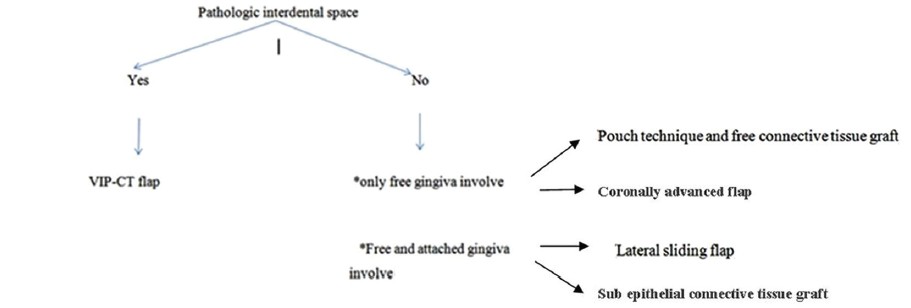 | Figure 5: Decision tree for esthetic management of gingival lesion in anterior maxilla
Click here to view |
This flap simultaneously corrects the labial soft tissue defect, covers the raw reduced interdental bone, and simultaneously augments the soft tissue. Its raw surface undergoes secondary epithelialization with the same color and consistency with adjacent mucosa after complete epithelialization.Vector of the VIP-CT flap contracture is favorable in this case and it is anticipated that creeping attachment happens.
Donor site morbidity is low and primary closure of palatal mucosa is possible.
Limitation of this technique is that because of pedicled nature of the flap, this technique is only applicable in anterior region of maxilla.
| Conclusion | | |
Reconstruction of the anterior maxillary gingival defects after pathologic resections that affect gingiva and interdental space is recommended with VIP-CT flap.
| Acknowledgements | | |
This study was supported by a grant from the Vice Chancellor of Research of Mashhad University of Medical Sciences.
| References | | |
| 1. | Walters JD, Will JK, Hatfield RD, Cacchillo DA, Raabe DA. Excision and repair of the peripheral ossifying fibroma: A report of 3 cases.J Periodontol 2001;72:939-44. 
|
| 2. | Corrente G, Abundo R, Re S, Cardaropoli D, Cardaropoli G. Orthodontic movement into infrabony defects in patients with advanced periodontal disease: A clinical and radiological study. J Periodontol 2003;74:1104-9.
|
| 3. | Anderegg CR, Metzler DG.Free gingival graft following biopsy: A case report of tissue management. J Periodontol 1996;67:532-5.
[PUBMED] |
| 4. | Zucchelli G, Mele M, Stefanini M, Mazzotti C, Marzadori M, Montebugnoli L, et al. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: A comparative randomized-controlled clinical trial. J Clin Periodontol 2010;37:728-38.
|
| 5. | Zucchelli G, Mazzotti C, Bentivogli V, Mounssif I, Marzadori M, Monaco C.The connective tissue platform technique for soft tissue augmentation.Int J Periodontics Restorative Dent 2012;32:665-75.
|
| 6. | Kahn S, Egreja AM, BarceleiroMde O. Subepithelial connective tissue graft associated with apicoectomy and root-end fillings in the treatment of deep localized gingival recession with apex root exposure: Case report. Int J Periodontics Restorative Dent 2009;29:445-9.
|
| 7. | Joda T. Esthetic management of mucogingival defects after total excision in a case of pyogenic granuloma. Eur J Esthet Dent 2012;7:110-9.
[PUBMED] |
| 8. | Sahingur SE, Cohen RE, Aguirre A. Esthetic management of peripheral giant cell granuloma. J Periodontol 2004;75:487-92.
|
| 9. | Bosco AF, Bonfante S, Luize DS, Bosco JM, Garcia VG. Periodontal plastic surgery associated with treatment for the removal of gingival overgrowth. J Periodontol 2006;77:922-8.
|
| 10. | Rahpeyma A, Khajehahmadi S. Modified VIP-CT flap in late maxillary alveolar cleft surgery. J Craniomaxillofac Surg 2013 [In press].
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|















