|


 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 6
| Issue : 1 | Page : 18-20 |
|
|
A case of esophagopericardial fistula as a complication of upper gastro-intestinal endoscopy
Chima K. P. Ofoegbu1, Neil Hendricks2, Lovendran Moodley3
1 Department of Surgery, Division of Cardiovascular and Thoracic Surgery, University of Ilorin, Ilorin, Nigeria,
2 Department of Medicine, The Cardiac Clinic, Groote Schuur Hospital, Cape Town, South Africa,
3 Chris Barnard Division of Cardiothoracic Surgery, Groote Schuur Hospital, Cape Town, South Africa,
| Date of Web Publication | 24-Jun-2014 |
Correspondence Address:
Chima K. P. Ofoegbu
University of Ilorin Teaching Hospital, PMB 1459, Ilorin 240 001, Nigeria
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.135142

 Abstract Abstract | | |
A case of suppurative pericarditis from an esophagopericardial fistula (EPF) following the upper gastrointestinal endoscopy (UGIE). A 38-year-old schizophrenic male patient with gastro-esophageal reflux disease (GORD) and previously dilated esophageal stricture was presented with acute retrosternal chest pain. The patient pulled out the endoscope during UGIE the previous day. A barium swallow (BS) post endoscopy was normal. The patient was initially hemodynamically stable and cardiac evaluation was normal. The patient subsequently developed features of cardiogenic shock. Echocardiography confirmed pericardial effusion and pericardial aspiration yielded pus. Surgical drainage with pericardial tube insertion was done. Pericardial biopsy revealed acute suppurative inflammation with food particles. The patient continued with antibiotics and pericardial drainage for 14 days and repeat BS and chest computerized tomography scan revealed no EPF. The patient was discharged 24 days after the presentation and remained well at follow-up. A rare, serious complication of UGIE which may be easily missed and is associated with a high mortality with delayed treatment. Keywords: Fistula, esophagus, pericardium, trauma
How to cite this article:
Ofoegbu CK, Hendricks N, Moodley L. A case of esophagopericardial fistula as a complication of upper gastro-intestinal endoscopy. J Surg Tech Case Report 2014;6:18-20 |
How to cite this URL:
Ofoegbu CK, Hendricks N, Moodley L. A case of esophagopericardial fistula as a complication of upper gastro-intestinal endoscopy. J Surg Tech Case Report [serial online] 2014 [cited 2016 May 10];6:18-20. Available from: http://www.jstcr.org/text.asp?2014/6/1/18/135142 |
| Introduction | |  |
An esophagopericardial fistula (EPF) is an uncommon condition seen in clinical practice and may be caused by trauma, benign or malignant pathology. The most common causes of OPF include; chronic esophagitis, esophageal ulcers, foreign body impaction and post-esophageal bouginage perforation. Malignant causes include esophageal cancer which may sometimes be associated with achalasia.
The common clinical presentation involves; pyrexia, retrosternal chest pain and breathlessness. Investigations that may confirm the diagnosis include; chest X-ray which commonest finding is pneumopericardium, contrast swallow which may show a fistulous tract connecting the esophagus to the pericardial sac and upper gastro-intestinal endoscopy which may show the fistula opening or the underlying disease.
We report a case of suppurative pericarditis as a result of an esophagopericardial fistula following a recent upper gastrointestinal endoscopy.
| Case report | | |
A 38-year-old male patient presented to our emergency unit with acute severe retrosternal chest pain of 2 h duration which was constant, non-radiating and associated with sweating and breathlessness.
The patient was an institutionalized schizophrenic with a history of gastro-esophageal reflux disease (GERD) with a previous esophageal stricture dilated 3 months earlier. On the day before the presentation he had undergone esophago-gastroscopy during which he forcefully pulled out the endoscope at mid esophageal level.
A barium swallow post endoscopy was normal [Figure 1]a and b].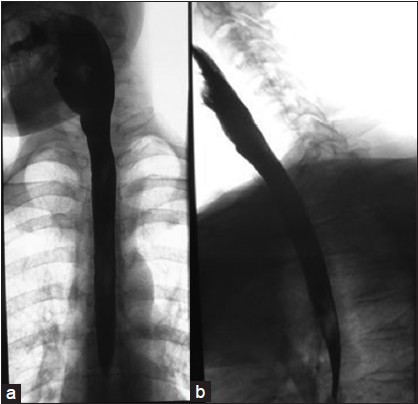 | Figure 1: (a) Barium swallow post endoscopy (b) Barium swallow post endoscopy
Click here to view |
He was afebrile, with a tachycardia of 109 beats per minute and a blood pressure of 108/89 mmHg. The rest of his examination including the cardiac evaluation was normal.
Initial electrocardiogram (ECG) revealed a sinus tachycardia and subtle saddle shaped ST elevation in V3 to V6. Chest radiograph (CXR) was unremarkable and a troponin level was <0.03 ng/ml.
Analgesia was given and he was observed overnight.
The following morning the patient developed severe pain and was found to be cold and clammy with a thready pulse, unrecordable blood pressure and distended neck veins. Widespread marked saddle shaped ST elevation was present on ECG and repeat CXR revealed an enlarged cardiac silhouette [Figure 2].
Echocardiography confirmed a pericardial effusion with echo bright densities within the pericardial space. Pericardial aspiration yielded 70 ml of frank pus.
Surgical drainage was performed and a pericardial drain was left in situ. Pericardial biopsy performed at surgery revealed acute suppurative inflammation with food particles.
Antibiotic therapy and pericardial drainage was continued for 14 days. A repeat barium swallow revealed no esophageal fistula [Figure 3].
The patient was finally discharged 24 days after initial presentation. He remained well at follow-up of 2 weeks post discharge.
| Discussion | | |
Esophagopericardial fistulae (EPF) are rare complications of esophageal pathology and are usually from benign pathology of the esophagus (Barrett's esophagus), esophageal surgery (esophagectomy, Nissen fundoplication), [1] endoscopy and fibrillation ablation procedures, [2] but are also caused by esophageal malignancy. [3],[4] Other benign esophageal conditions implicated include; esophageal ulcers, chronic esophagitis, tuberculosis, ingested foreign body, esophageal diverticula and very rarely achalasia. [2],[5],[6] Benign etiologies that are uncommon may be from increased intra-luminal esophageal pressure leading to esophageal perforations as seen in opening pressurized soft drink containers with the mouth, hyperemesis gravidarum and childbirth. [7] Conditions associated with an increased intra-abdominal pressure, for example, heavy weightlifting, exercises, laughing fits, seizures and blunt abdominal trauma can also cause esophageal perforations which may culminate into the development of an esophagopericardial fistula. [7] A rare case of barogenic esophageal perforation from riding a bicycle has previously been reported. [8] The clinical features that suggest EPF include retrosternal pain, dyspnoea, fever and if severe enough like in this patient, may present with hemodynamic collapse suggestive of a septic/cardiogenic shock.
The rarity of this condition allows for missed or late diagnosis which is also compounded by the non-specific nature of the clinical features and a high mortality rate may be the consequence of delayed treatment. [9] This case emphasizes the importance of being well acquainted with the potential complications of invasive procedures. A high index of suspicion is imperative and if a patient presents with symptoms after an invasive procedure, it should be assumed to be due to a complication of the procedure.
Pneumopericardium is the most frequent chest radiographic finding, present in about 50% of cases, but was absent in this extant case. [10] Other chest X-ray findings may include pleural effusions and lung infiltrates which are seen in 20% of cases. [10] The barium swallows done in this patient were normal and did not reveal the EPF (gross filling of the pericardial sac with contrast material) and is consistent with the reported barium swallow sensitivity of 69-80 [11] for the detection of esophagopericardial fistula. Upper gastro-intestinal endoscopy (UGIE) may show the fistula and any associated underlying pathology, but was not done in this case because it was thought UGIE was the culprit.
Most survivors of this condition are usually those whose surgical treatment are established early in the clinical course. [7],[8] The patient's survival in this case may be attributed to early diagnosis and treatment which include; surgical drainage of the pericardial effusion, antibiotic therapy and adequate supportive treatment which led to the closure of the fistula non-operatively.
| References | | |
| 1. | Farjah F, Komanapalli CB, Shen I, Sukumar MS. Gastropericardial fistula and candida kruzei pericarditis following Nissen fundoplication (gastropericardial fistula).Thorac Cardiovasc Surg2005;53:365-7. 
|
| 2. | Ali F, Mostafa A, Charachon A, Karoui M, Loisance D, Kirsch M. Multidisciplinary therapy of a large esophago-pericardial fistula arising from Barrett's esophagus. Ann Thorac Surg 2008;86:1690-3.
|
| 3. | Kaufman J, Thongsuwan N, Stern E, Karmy-Jones R. Esophageal-pericardial fistula with purulent pericarditis secondary to esophageal carcinoma presenting with tamponade. Ann Thorac Surg2003;75:288-9.
|
| 4. | Luthi F, Groebli Y, Newton A, Kaeser P. Cardiac and pericardial fistulae associated with esophageal or gastric neoplasms: A literature review. Int Surg 2003;88:188-93.
|
| 5. | Strong RW. Oesophago-cardiac fistula complicating achalasia. Postgrad Med J 1974;50:41-4.
|
| 6. | Miller WL, Osborn MJ, Sinak LJ, Westbrook BM. Pyopneumopericardium attributed to an esophagopericardial fistula: Report of a survivor and review of the literature. Mayo Clin Proc 1991;66:1041-5.
|
| 7. | Bjerke HS.Boerhaave's syndrome and barogenic injuries of the esophagus. Chest Surg Clin N Am 1994;4:819-25.
[PUBMED] |
| 8. | Gonzalez-Ojeda A, de LunaVargas MA, Nazara-Cazorla Z, Anaya-Prado R, Radillo LG. Esophagopericardialfistula attributed to a barogenic rupture of the esophagus. Report of a case and review of the literature.Hepatogastroenterology 2001;48:1375-8.
|
| 9. | Greven WL, Kooij N, Peters HM, Kardux J, Spronk PE. Cardiac tamponade, an unusual and fatal complication of esophagus dilatation for benign stenosis: A case report. Cases J 2008;1:419.
|
| 10. | Cyrlak D, Cohen AJ, Dana ER. Esophagopericardial fistula: Causes and radiographic features. AJR Am J Roentgenol 1983;141:177-9.
[PUBMED] |
| 11. | Dafnios N, Anastasopoulos G, Marinis A, Polydorou A, Gkiokas G, Fragulidis G, et al. Esophagopericardial fistula as a rare complication after total gastrectomy for cancer. World J Surg Oncol 2009;7:58.
|
[Figure 1], [Figure 2], [Figure 3]
|

















