|


 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 6
| Issue : 1 | Page : 26-28 |
|
|
Anterior roux-en-Y Pancreatico-jejunostomy for pancreatic trauma
PS Aravinda, Sudipta Saha, Manoj Andley, OP Pathania, Ajay Kumar
Department of Surgery, Lady Hardinge Medical College, New Delhi, India
| Date of Web Publication | 24-Jun-2014 |
Correspondence Address:
P S Aravinda
63, Defence Enclave, Vikas Marg, New Delhi 110 092
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.135147

 Abstract Abstract | | |
Isolated pancreatic laceration is a rare injury. The typical mechanism by which it occurs is overstretching of the pancreas across the vertebral column during blunt abdominal trauma. The management depends on the location and extent of the injury. Disruption of the pancreatic duct usually requires operative treatment. Operative options for pancreatic laceration at the neck include distal pancreatectomy or suturing of the cephalic remnant and Roux-en-Y pancreatico-jejunostomy on the left remnant. We are reporting two cases of isolated pancreatic injury with disruption of the pancreatic duct but preserved posterior surface of the pancreas. These patients were managed by performing anterior Roux-en-Y pancreatico-jejunostomy at the lacerated area. Both the patients had successful outcome with removal of drains by 6 th postoperative day. Anterior Roux-en-Y pancreatico-jejunostomy in this particular scenario is easy, less time consuming, and has the advantage of preserving the pancreas and the spleen. Keywords: Pancreatic trauma, Roux-en-Y pancreatico-jejunostomy, anterior pancreatico-jejunostomy
How to cite this article:
Aravinda P S, Saha S, Andley M, Pathania O P, Kumar A. Anterior roux-en-Y Pancreatico-jejunostomy for pancreatic trauma. J Surg Tech Case Report 2014;6:26-8 |
How to cite this URL:
Aravinda P S, Saha S, Andley M, Pathania O P, Kumar A. Anterior roux-en-Y Pancreatico-jejunostomy for pancreatic trauma. J Surg Tech Case Report [serial online] 2014 [cited 2016 May 10];6:26-8. Available from: http://www.jstcr.org/text.asp?2014/6/1/26/135147 |
| Introduction | |  |
Pancreatic injuries can be caused by penetrating or blunt trauma to the abdomen. They occur in approximately 5% of all abdominal injuries. [1] Pancreatic injuries are usually associated with injuries of other intra-abdominal organs, and isolated pancreatic rupture is quite rare. [2] Management may vary from non operative management, including image-guided drainage, to complex procedures like distal pancreatectomy and pancreatico-jejunostomy. [3] We are reporting two cases of isolated pancreatic injury with disruption of the pancreatic duct but preserved posterior surface at the site of laceration. These patients were managed by anastomosing Roux loop of jejunum with the lacerated site of the pancreas.
| Case Reports | | |
Case 1
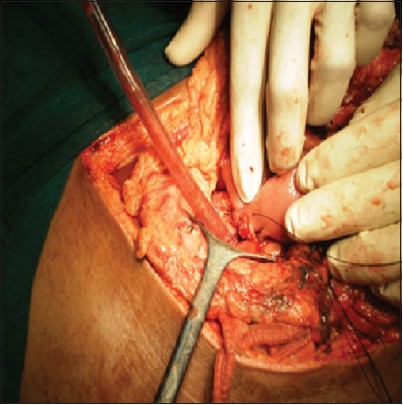
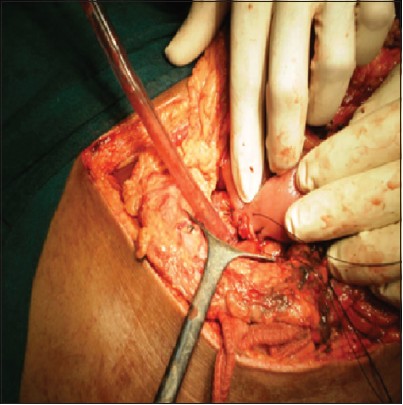
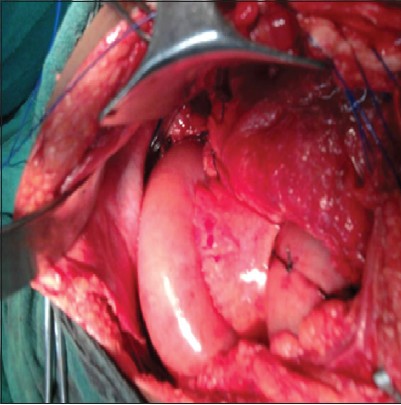
A 35-year-old male presented in the emergency department with the complaint of pain over epigastrium following direct compression injury of the upper abdomen with a concrete tile 5 days ago. Pain was continuous, severe, and radiating to back. On examination, the patient had tachycardia (pulse 102/min), along with tenderness and guarding over the epigastrium. Sonography of abdomen revealed free fluid in the peritoneal cavity. The body and tail of the pancreas had shaggy margins and there was peripancreatic collection. Contrast-enhanced computed tomography (CECT) scan of the abdomen showed laceration of pancreas at neck with injury of the pancreatic duct [Figure 1]. On exploratory laparotomy, the pancreas was found to be lacerated at the level of neck with disruption of the pancreatic duct. However, the posterior surface of the pancreas was preserved at the site of laceration [Figure 2]. An anterior Roux-en-Y pancreatico-jejunostomy was done at the lacerated site of the pancreas [Figure 3]. In this, the lacerated site of the pancreas was anastomosed to the lateral opening made in a Roux loop of the jejunum in two layers. Postoperatively, the drain output gradually reduced to minimum by day 4 and the patient was discharged on day 6. Patient is healthy at the last follow-up 10 months after the operation.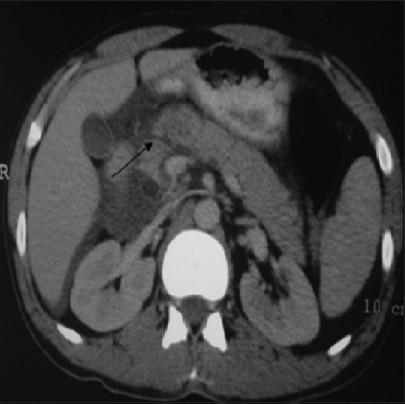 | Figure 1: CECT abdomen showing laceration at the neck of the pancreas (arrow)
Click here to view |
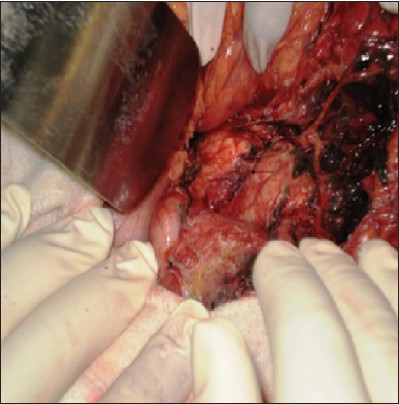 | Figure 2: Intraoperative photograph showing laceration of the pancreas (arrow)
Click here to view |
Case 2
A 35-year-old male presented with a history of fall from height of approximately 15 feet. At the time of presentation, the patient was having tachycardia (pulse rate 108/min) and his BP was 130/80 mm Hg. Abdomen was distended and there were signs of peritonitis. Ultrasound of the abdomen showed free fluid in the abdomen. CECT abdomen showed laceration at the neck of pancreas with surrounding hematoma and disruption of the pancreatic duct [Figure 4]. On exploratory laparotomy, laceration of 1.5 cm × 1 cm × 1.5 cm was found at the neck of the pancreas with disrupted pancreatic duct but intact posterior surface of the pancreas at the lacerated site [Figure 5]. Anterior Roux-en-Y pancreatico-jejunostomy was done with suturing of edges of the laceration of pancreas to the side of Roux-en-Y loop of the jejunum [Figure 6]. The postoperative course was uneventful. Drain output decreased to minimum 6 days after the operation and the patient was discharged on the 7 th day. The patient is normal at 1 year of follow-up.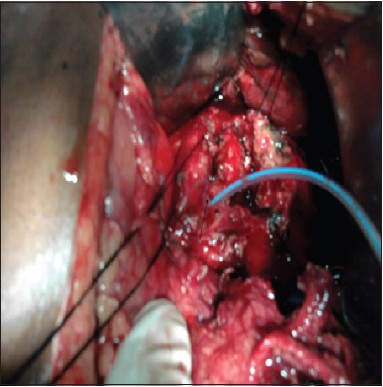 | Figure 5: Intraoperative photograph showing lacerated pancreas. Pancreatic duct is shown cannulated with feeding tube
Click here to view |
| Discussion | | |
Pancreatic injury most often results because of blunt trauma to the epigastrium causing the neck of the pancreas to be crushed against the vertebra. Pancreatic injury is usually associated with injuries to the other abdominal organs as well. [2] Integrity of the pancreatic duct is one of the main factors which decide the management option in pancreatic injury. Missed pancreatic duct injury may result in complications such as pseudocysts, fistulas, pancreatitis, sepsis, and secondary hemorrhage. Some of these complications can cause significant morbidity and can even be life threatening. [4] In the absence of injury to the pancreatic duct, simple debridement of devitalized pancreas and drainage is sufficient. However, injury of the pancreatic duct requires definite operative procedures depending upon the location of the injury. Distal pancreatectomy along with splenectomy is usually done for pancreatic duct injury at the body, neck, and tail of the pancreas. Spleen preserving distal pancreatectomy is also an option which has the advantage of preservation of spleen, but it increases the operation time. [4],[5]
Drawbacks of distal pancreatectomy at the neck include loss of splenic function if splenectomy is done along with distal pancreatectomy and the possibility of endocrine dysfunction. Endocrine dysfunction has been reported in 8-10% of patients after distal pancreatectomy done for a variety of indications. [6],[7] It has also been reported in a small series of patients in whom distal pancreatectomy was done for trauma. [8] For these reasons, distal pancreatico-jejunostomy is an option in pancreatic injuries at the neck with disruption of the duct, as it has the advantages of preserving the spleen and pancreas. [9]
We have reported here two cases of pancreatic laceration with pancreatic duct injury, where posterior surface of the pancreas was intact. We propose anterior pancreatico-jejunostomy as a management option in this type of pancreatic injuries. In this, the edges of the laceration are anastomosed to the opening made at the side of a Roux loop of jejunum. This repair has the advantage of preservation of pancreas and spleen, and further, the operative time is less as no mobilization of the pancreas is required. This procedure has been described previously in nine patients, and was found to be an appropriate procedure in patients in whom posterior pancreatic capsule was intact. [10]
| Conclusion | | |
Pancreatic laceration with disruption of the duct and preserved posterior surface is rare. Our experience of these two cases shows that anterior pancreatico-jejunostomy is a feasible option for the management of this type of injury. We propose that if the surgeons come across such a type of pancreatic injury, anterior pancreatico-jejunostomy should be considered.
| References | | |
| 1. | Subramanian A, Dente CJ, Feliciano DV. The management of pancreatic trauma in the modern era. Surg Clin N Am 2007;87:1515-32. 
|
| 2. | Levine RA, Bank MA. Traumatic transection of the pancreas. Case of delayed presentation. JOP 2011;12:47-9.
|
| 3. | Degiannis E, Glapa M, Loukogeorgakis SP, Smith MD. Management of pancreatic trauma. Injury 2008;39:21-9.
|
| 4. | Krige JE, Beningfield SJ, Nicol AJ, Navsaria P. The management of complex pancreatic injuries. S Afr J Surg 2005;43:92-102.
|
| 5. | El-Boghdadly S, Al-Yousef Z, Al Bedah K. Pancreatic injury: An audit and a practical approach. Ann R Coll Surg Engl 2000;82:258-62.
|
| 6. | Lillemoe KD, Kaushal S, Cameron JL, Sohn TA, Pitt HA, Yeo CJ. Distal pancreatectomy: Indications and outcomes in 235 patients. Ann Surg 1999;229:693-8.
|
| 7. | King J, Kazanjian K, Matsumoto J, Reber HA, Yeh MW, Hines OJ, et al. Distal pancreatecomy: Incidence of postoperative diabetes. J Gastrointest Surg 2008;12:1548-53.
|
| 8. | Al-Ahmadi K, Ahmed N. Outcomes after pancreatic trauma: Experience at a single institution. Can J Surg 2008;5:118-24.
|
| 9. | Bhat S, Azad TP, Kaur M. Pancreaticojejunostomy in proximal pancreatic transection: A viable option. N Am J Med Sci 2011;3:46-7.
|
| 10. | Jones RC. Management of pancreatic trauma. Ann Surg 1978;187:555-64.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]
|