|


 |
| SURGICAL TECHNIQUE |
|
| Year : 2014 | Volume
: 6
| Issue : 1 | Page : 5-8 |
|
|
Single stage reconstruction of type IIA defect of the ear lobule: The limberg flap technique revisited
Abdulrasheed Ibrahim
Department of Surgery, Ahmadu Bello University, Zaria, Nigeria
| Date of Web Publication | 24-Jun-2014 |
Correspondence Address:
Abdulrasheed Ibrahim
Department of Surgery, Ahmadu Bello University, Zaria
Nigeria
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.135133

 Abstract Abstract | | |
The ear lobule is an important reference point for symmetry of the face and its loss causes an obvious aesthetic abnormality. Type II A defects are characterized by loss of the ear lobule without presence of a nubbin of tissue attached to the cheek. Such defects are typically seen in individuals having an unattached ear lobule. The goal of surgery should be an aesthetically pleasing reconstruction that maintains symmetry with the opposite ear lobule. The Limberg-flap technique using a doubled-over skin flap allows a one stage reconstruction of the ear lobule. It is technically simple and may be performed under local anesthesia. The aesthetic results are generally well acceptable and there is a good color match between the neolobule and the surrounding skin.
Keywords: Ear lobule, Limberg flap, reconstruction, single stage, type IIA defect
How to cite this article:
Ibrahim A. Single stage reconstruction of type IIA defect of the ear lobule: The limberg flap technique revisited. J Surg Tech Case Report 2014;6:5-8 |
How to cite this URL:
Ibrahim A. Single stage reconstruction of type IIA defect of the ear lobule: The limberg flap technique revisited. J Surg Tech Case Report [serial online] 2014 [cited 2016 May 10];6:5-8. Available from: http://www.jstcr.org/text.asp?2014/6/1/5/135133 |
| Introduction | |  |
The auricle is a complex structure of intricate cartilage folds covered by skin. [1] It has an undulating topography and structural configuration ranging from a firm rigid cartilage to the soft, spongy and elastic ear lobule. [2] The ear lobule is a special subunit of the auricle and deformities are more commonly acquired following trauma. Complete agenesis of the lobule is documented but is very rare. The ear lobule is an important reference point for symmetry of the face and its loss causes an obvious aesthetic abnormality. [3],[4]
There are key anatomic features of the ear lobule that make reconstruction unique and profoundly affect the skill set required for success. These include: A robust vascular supply, a topography which is highly variable and a relatively inconspicuous lateral location with limited visibility on frontal view. These should be taken into consideration by the plastic surgeon to optimize outcome. [2],[5],[6]
The ear lobule lends itself readily to reconstruction with a variety of techniques. The ideal technique should be simple, expeditious, easily implemented and complication free. [7],[8] This article describes the technique of reconstruction of the type IIA defect of the ear lobule using a doubled-over Limberg flap.
| Surgical technique | | |
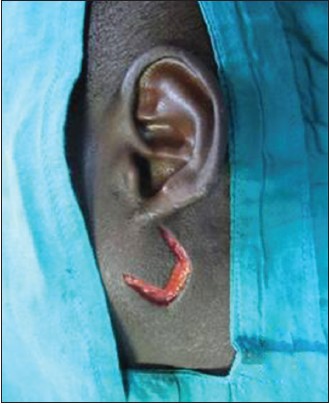
The opposite normal ear lobule is used as a model for the type IIA ear lobule defect being reconstructed [Figure 1]. [9] The limberg flap is outlined anteriorinferior to the ear lobule defect ensuring that the side of the defect and the flap are equal in length [Figure 2]. The operation may be performed under local anaesthesia using 1% lignocaine hydrochloride mixed with epinephrine. The flap is elevated at the level of subcutaneous tissue by sharp dissection [Figure 3]. The scar at the inferior edge of the ear is excised and the Limberg flap is transposed [Figure 4]. This once sutured, constitutes the curved free edge of the ear lobule. The edges of the secondary defect is appropriately undermined to facillitae direct closure [Figure 5]. The defect of the ear lobule is roughly a sector of a circle (abd) [Figure A], which would become a rhomboid (abcd) if its posterior-medial layer were unfolded. The edge ad' is sutured to the edge ab of the ear [Figure B]. Nonabsorbable sutures (nylon 5/0) are commonly used. The flap is folded along its short diagonal (d'f) so that the distal half (d'ef) [shaded in Figures B and C] comes to lie behind ad'f and point e comes to lie behind point a. The edge d'e is stitched to the posterior edge of ab, and edge ef is stitched to af [Figure C]. [9] | Figure 1: Pre-operative appearance of a type IIA defect of the ear lobule
Click here to view |
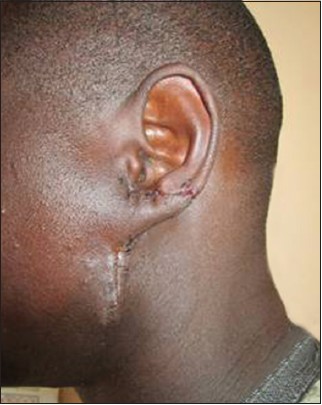
 | Figure 5: Flaps sutured and secondary defect is closed by direct approximation
Click here to view |

| Discussion | | |
Defects of the ear lobule are three dimensional requiring the plastic surgeon to seek creative reconstructive options. Type II A defects are characterized by loss of the ear lobule without presence of a nubbin of tissue attached to the cheek. Such defects are typically seen in individuals having an unattached ear lobule. [10] Reconstruction thus requires thoughtful planning. The goal should be an aesthetically pleasing reconstruction that maintains symmetry with the opposite earlobe. [11]
Several detailed reviews have described the full spectrum of reconstructive options. [3],[4],[6],[7],[8],[11],[12],[13] They broadly fall into five categories: (a) Preauricular flap reconstruction; (b) postauricular flap reconstruction; (c) superimposition of two opposing or paired flaps; and (d) tissue expansion using a tubed flap; (e) a combination of techniques. [4] Some of the drawbacks of these described methods include; burden on the patient from a two-stage procedure, an unnatural contour of the lobule, firmness due to placement of cartilage and flaps from the neck may bring abnormally hairy skin to the ear lobule. [11] Furthermore, some of the documented techniques have only reconstructed one surface of the ear lobule and have required a split skin graft for the opposite surface. This generally leads to poor cosmesis because the lobule is too thin and retracts secondarily. Grafted cartilage prevents scar contracture, but a deformity may result from secondary absorption of the cartilage. [3]
Limberg described the rhomboid skin flap in 1946. The underlying flap design is based on the transposition of a rhomboid or parallelogram with 120˚ angles located where there is lax skin (that will form the flap), whereas the other two angles are 60˚ each. [14] Some technical details need to be empasized. The Limberg flap is a durable flap that is based on a random pattern cutaenous and subcutaenous pedicle. The flap is elevated slightly beyond the base of the flap going from distal to proximal. There maybe a standing cone deformity, which is excised with a burow's triangle excision. This also facillitate transposition of the flap. It may, however, be a little bulky and need defatting after 3-4 months. The donor defect is also visible and needs careful suturing to give a fine scar. This method is not suitable if the loss is greater than an ear lobule. [9]
The Limberg-flap technique using a doubled-over skin flap encompasses several advantages. It allows an immediate, one stage reconstruction of both the anterior and the posterior surfaces of the ear lobule [Figure 6]. It is technically simple and may be performed under local anesthesia. Skin grafts are not required and the flap is very safe and predictable. The aesthetic results are generally well acceptable, [9] and it offers the great advantage of a good color match between the neolobule and the surrounding skin.
| Conclusions | | |
Full-thickness defects of the ear lobule remain an intruiging reconstructive challenge for the plastic surgeon. The Limberg-flap technique remains useful in the reconstruction of type IIA defects. It provides satisfactory results and alleviates the drawbacks of the numerous alternative techniques. It is recommended for immediate and delayed reconstruction of the ear lobule.
| References | | |
| 1. | Gault D. Post traumatic ear reconstruction. J Plast Reconstr Aesthet Surg 2008;61 Suppl 1:S5-12. 
[PUBMED] |
| 2. | Brodland DG. Auricular reconstruction. Dermatol Clin 2005;23:23-41, v.
[PUBMED] |
| 3. | Khemani S, Rannard F, Kenyon G. Bi-lobar post-auricular skin flap for reconstruction of the earlobe. J Laryngol Otol 2007;121:1094-5.
|
| 4. | Shen W, Cui J, Chen J, Chen H, Zou J, Ji Y. Inversion of the flap at the lower ear and restoration of the flap at postauricular skin for reconstruction of the earlobe. J Craniofac Surg 2012;23:560-2.
|
| 5. | Savaci N, Tosun Z, Hoşnuter M. Ear lobe reconstruction with a posterior ear flap. Case reports. Scand J Plast Reconstr Surg Hand Surg 2000;34:173-5.
|
| 6. | Alconchel MD, Rodrigo J, Cimorra GA. A combined flap technique for earlobe reconstruction in one stage. Br J Plast Surg 1996;49:242-4.
|
| 7. | Sleilati F. Immediate earlobe reconstruction with double-crossed skin flaps. J Plast Reconstr Aesthet Surg 2006;59:1003-5.
[PUBMED] |
| 8. | Fidalgo Rodriguez F, Navarro Cecilia J, Rioja Torrejón L. Earlobe reconstruction with a modified bilobed flap. Plast Reconstr Surg 2010;126:23e-24e.
|
| 9. | Singh A, Singh G. Earlobe reconstruction using a Limberg flap in six ears. Br J Plast Surg 2003;56:33-6.
|
| 10. | Mohapatra DP, Friji MT, Chittoria RK, Kumar SD. Algorithm based on eighteen patients with acquired traumatic earlobe defects not associated with jewellery. Clin Otolaryngol 2013;38:386-9.
|
| 11. | Samolitis NJ, Florell SR, Mobley SR, Bowen GM. Use of a conchal bowl flap for repair of the earlobe. Arch Dermatol 2005;141:947-9.
|
| 12. | Di Mascio D, Castagnetti F. Tubed flap interpolation in reconstruction of helical and ear lobe defects. Dermatol Surg 2004;30:572-8.
|
| 13. | Kumar P, Shah P. Preauricular flap for post burn ear lobe reconstruction-a case report. Burns 2000;26:571-4.
|
| 14. | Maciel-Miranda A, Morris SF, Hallock GG. Local flaps, including pedicled perforator flaps: Anatomy, technique, and applications. Plast Reconstr Surg 2013;131:896e-911e.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]
|