|


 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 7
| Issue : 1 | Page : 7-11 |
|
|
Single visit feeding appliance for 1-day-old neonate with cleft palate using safe dental putty-gauze hybrid impression technique for maxillary impression
Manu Rathee
Department of Prosthodontics, Post Graduate Institute of Dental Sciences, Pt. B.D. Sharma University of Health Sciences, Rohtak, Haryana, India
| Date of Web Publication | 29-Jun-2016 |
Correspondence Address:
Manu Rathee
Department of Prosthodontics, Post Graduate Institute of Dental Sciences, Pt. B.D. Sharma University of Health Sciences, Rohtak, Haryana
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2006-8808.184938

 Abstract Abstract | | |
Cleft lip and palate is one of the most common craniofacial anomalies of humans. Intraoral impression making is the first clinical step in the fabrication of feeding appliance for infants with oro-nasal communication. It is difficult to control the flow of the impression material in the cleft area and undercuts in a child patient. This clinical report presents a simple and safe impression technique for maxillary impression making in neonates and infants with cleft palate. A gauze piece was used to confine the impression material during functional movements of sucking while impression making in an awake child to avoid the risk of aspiration or swallowing. Keywords: Cleft palate, feeding plate, maxillary impression, obturator
How to cite this article:
Rathee M. Single visit feeding appliance for 1-day-old neonate with cleft palate using safe dental putty-gauze hybrid impression technique for maxillary impression. J Surg Tech Case Report 2015;7:7-11 |
How to cite this URL:
Rathee M. Single visit feeding appliance for 1-day-old neonate with cleft palate using safe dental putty-gauze hybrid impression technique for maxillary impression. J Surg Tech Case Report [serial online] 2015 [cited 2018 Jul 1];7:7-11. Available from: http://www.jstcr.org/text.asp?2015/7/1/7/184938 |
| Introduction | |  |
Cleft lip and palate (CLP) is one of the most common craniofacial anomalies of humans.[1] Varied incidence of CLP deformity caused due to unknown precise etiology is reported in the literature with severity ranging from minor notching of lip or bifid uvula to complete unilateral or bilateral cleft of the lip and palate. Newborns with abnormal oro-nasal communication face the threat to life due to difficulty in feeding.[2] Hence, there arises an acute demand of feeding appliance that serves as an obturator in the cleft area, in view of the complications of feeding tube. A feeding appliance or obturator is a prosthetic aid that is used to restore the separation between oral and nasal cavities.[3] It assists in suckling and hence feeding.
Intraoral impression making is the first clinical step in the fabrication of feeding appliance. In addition, it is also the primary step in the fabrication of different devices such as palatal obturator, articulation development prosthesis, palatopharyngeal obturator, palatal lift prosthesis, nasal conformer, and appliances for presurgical infant orthopedic or presurgical nasoalveolar molding, those that are introduced to enhance speech, esthetics, and function.
It has been emphasized in literature that every precaution must be taken while making impression for neonates and infants with cleft palate, and surgeons' presence is needed to manage airway emergency.[4],[5] Maneuvering the child's head position forward to avoid the aspiration of impression material has been the only suggested precaution. This does not ensure complete control over the impression material and avoidance of complication of impression material being pushed too deep into the nasal cavity or distally through the pharynx. This clinical report presents dental putty-gauge hybrid impression technique as a simple and safe method of maxillary impression making in neonates and infants with cleft palate, permitting complete control over impression material during functional movements.
| Case Report | | |
A 1-day-old male infant was referred for fabrication of feeding plate. The infant's parents presented with a chief complaint of difficulty in feeding. There was a history of defect in the lip and palate since birth. Family history was noncontributory. On extraoral examination, there was bilateral complete cleft lip with forward placed premaxilla [Figure 1]. Intraoral examination revealed a median cleft of the palate involving complete soft and hard palate [Figure 2]. After detailed history and examination, a diagnosis of nonsyndromic CLP was made. Parents' counseling was done to allay their anxiety. They were explained the treatment plan for fabrication of feeding plate and consent was obtained.
It was planned to make the maxillary impression when the infant was fully awake, without any premedication or anesthesia. The infant was seated upright in his mother's lap in dental chair with face forward. Small size of the mouth opening did not permit the use of impression tray or flat wooden stick as carrier for the material. Thus, it was planned to make impression with finger-loaded impression material. Fast setting elastomeric putty impression material (Express ™ STD, 3M ESPE, USA) was mixed and loaded on the index finger and an adequately large piece of gauze was wrapped all over the loaded impression material with loose ends wrapped toward the hand [Figure 3] and [Figure 4]. The gauze permitted control over the material and restricted the excessive displacement of impression material toward the nasal cavity and pharynx [Figure 5]. Thick consistency of the impression material did not permit leakage of material through the gauze and kept it within the flexible confines of the gauze. The child was encouraged to perform sucking during the impression making. The functional movements facilitated recording of tissue details and undercuts. The resultant sucking pressure embedded the gauze threads in the putty impression material as the easily moldable gauge did not offer any resistance. After the impression material was set, the impression was removed in toto from the patient's mouth [Figure 6] and [Figure 7]. Then, the impression was poured in dental stone (Kalstone, Kalabhai Karson Pvt Ltd)., Mumbai, Maharashtra, India) and the master cast was obtained [Figure 8]. Single visit feeding obturator was fabricated using clear, flexible thermal-forming material with a midline extraoral extension for a hole to tie a safety thread [Figure 9]. It was finished and polished for smooth surfaces. The neonate could comfortably perform sucking with the feeding obturator [Figure 10]. The mother could feed the child immediately after insertion without nasal regurgitation.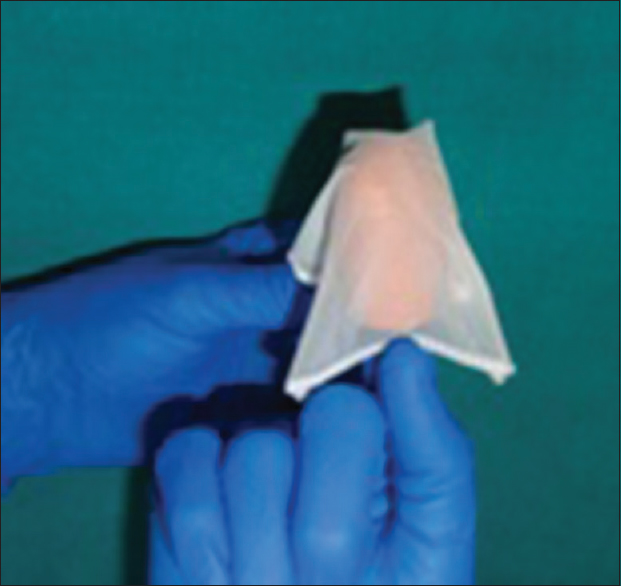 | Figure 4: Gauze wrapped around the putty impression material loaded on the finger
Click here to view |
 | Figure 5: Maxillary impression made with functional movements by neonate
Click here to view |
Parents were demonstrated about the use and hygiene maintenance of the feeding plate. A regular follow-up after 24 h and monthly follow-ups later were scheduled and the parents were advised to use the appliance till surgical intervention. No untoward effect was noticed during the follow-up.
| Discussion | | |
A cleft palate hampers intraoral pressure built-up required for suction and favors nasal reflex of food, thus posing challenge of middle ear infections. Feeding is an immediate concern for newborn with CLP where the role of dentist and the feeding plate is evident.[3] Various head and body positions and diverse impression materials have been used to make maxillary impression in neonates and infants with suggestions to take all precautions including the presence of surgeon to handle airway emergency. A feeding appliance bridges the gap between oral and nasal cavities. Feeding obturator becomes urgent in CLP infants considering the health of the infant as surgical treatment usually starts at 2–3 months of age.[4] Presurgical orthopedic appliance fabrication for children with cleft also begins with impression making. However, little is found in literature regarding the impression required to fabricate these maxillary appliances.[6]
Impression making is the initial, crucial, and clinical step in cleft palate of infants and poses a challenge because of lack of cooperation from patient, inadequate size of oral cavity, and nonavailability of suitable impression trays. There is a risk of breakage of some parts of impression material that may get lodged in the undercut in the defect or the child can swallow or aspirate the material. Difficulty in withdrawal of impression, cyanotic events, and asphyxiation has been encountered during impression making.[7] Displaced intranasal impression material may remain undetected for a very long period of time.[8] Patient positioning, tray, and impression material are the important factors for safety.
Impression compound softened and placed on finger is the commonly used method to make preliminary impression. Individualized impression trays for CLP have been designed and the tray handle has also been used to carry the material.[9] Impression making under general anesthesia has been adopted for infants. Adequate suctioning and resuscitation facilities should be available chairside. In case of airway emergency, the surgeon's presence is mandatory to help with the impression.[5] It is advised to maneuver the infant position and head position to keep the tongue forward to avoid posterior displacement of impression material. Making the child to cry throughout the impression procedure ensures that there is no aspiration. However, it does not prevent the thin consistency material passing down the pharynx. In this case, the child was not crying during the procedure, but performed the functional movements to mold the impression material to obtain accurate anatomic details. Cleft palate affects feeding, facial growth, dentition development, speech, and may cause psychological problems for the child and parents as acceptance of the parents for the dysmorphic child can be difficult. However, in the present case, parents were involved in the care from the start of therapy that provided assurance and motivation to them.
A variety of impression materials have been advocated; however, putty type vinyl polysiloxane has been used in this case because its high viscosity reduces the risk of aspiration and there is no risk of thermal injury to the delicate oral mucosa of the neonate unlike that with the use of wax or thermoplastic impression compound. The use of gauze wrapped around the impression material throughout the functional movements completely removed the chances of aspiration or swallowing of material making, it a risk-free procedure in an awake child as young as 1-day-old.
The commonly used material for feeding plate is acrylic resin that needs multiple visits. However, in this patient, soft, clear, and flexible thermoplastic material was used as it permitted a single-step appliance fabrication. The feeding plate was delivered without any delay, on the same day in view of the urgency for feeding the newborn. The prosthetic therapy delivered through feeding plate remains a suitable treatment modality until the time prenatal diagnosis and intrauterine fetal surgery through feto-endoscopic approach for human fetus with a CLP are well established.[10]
| Conclusion | | |
This article describes the successful immediate oral rehabilitation of CLP neonate achieved with simple feeding appliance and risk-free procedure that decreased the stress for the parents and the child and provided instant feeding ability. Maxillary impression procedure in infants with cleft palate poses a unique set of challenges and we should be well-equipped for every precaution while making impression.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Chandna P, Adlakha VK, Singh N. Feeding obturator appliance for an infant with cleft lip and palate. J Indian Soc Pedod Prev Dent 2011;29:71-3.  [ PUBMED]  |
| 2. | Goldberg WB, Ferguson FS, Miles RJ. Successful use of a feeding obturator for an infant with a cleft palate. Spec Care Dentist 1988;8:86-9. |
| 3. | Rathee M, Hooda A, Tamarkar AK, Yadav SP. Role of feeding plate in cleft palate: Case report and review of literature. Internet J Otorhinolaryngol 2010;12:1. |
| 4. | Gupta R, Singhal P, Mahajan K, Singhal A. Fabricating feeding plate in CLP infants with two different material: A series of case report. J Indian Soc Pedod Prev Dent 2012;30:352-5. [ PUBMED] |
| 5. | Grayson BH, Maull D. Naso alveolar moulding for infants born with clefts of the lip, alveolus and palate. Semin Plast Surg 2005;19:294-301. |
| 6. | Pani SC, Hedge AM. Impressions in cleft lip and palate – A novel two stage technique. J Clin Pediatr Dent 2008;33:93-6. |
| 7. | Chate RA. A report on the hazards encountered when taking neonatal cleft palate impressions (1983-1992). Br J Orthod 1995;22:299-307. |
| 8. | Jones SD, Drake DJ. Case series of undetected intranasal impression material in patients with clefts. Br J Oral Maxillofac Surg 2013;51:e34-6. |
| 9. | Ravichandra KS, Vijayaprasad KE, Vasa AA, Suzan S. A new technique of impression making for an obturator in cleft lip and palate patient. J Indian Soc Pedod Prev Dent 2010;28:311-4. [ PUBMED] |
| 10. | Goodacre T, Swan MC. Cleft lip and palate: Current management. Paediatr Child Health 2012;22:160-8. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10]
|























