|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 16
| Issue : 1 | Page : 20-22 |
|
Male infertility: diagnostic and epidemiological aspect concerning 96 cases in a teaching university hospital of cotonou, benin republic
Prince Pascal Hounnasso1, Josué Dedjinnin Georges Avakoudjo1, Abdoudjalilou Sanni Dankoro1, Fouad Kolawalé Yde Soumanou1, Gilles Natchagé1, Michel Michael Agounkpé1, Rafiou Sanni Toré2
1 Department of Urology, Teaching Univesity Hospital (CNHU-HKM), Cotonou, Benin
2 Department of Surgery, Savè Hospital, Benin
| Date of Web Publication | 8-Oct-2015 |
Correspondence Address:
Fouad Kolawalé Yde Soumanou
Teaching University Hospital (CNHU-HKM), Cotonou
Benin
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.166886

Objectives: The goal of this study is to describe the epidemiological and diagnostic aspect of male infertility in the Department of Urology and Andrology of the Hospital mentioned above.
Methods: This was a retrospective descriptive study of 6 months duration at the Academic Clinic of Urology and Andrology of a Teaching Hospital in Cotonou. A total of 96 medical records of patients were retrieved for the study.
Results: The average age of the patients was 37.2 ± 6.7 years old. About 59.4% of the cases were primary infertility. The average duration of the infertility was 51 months. From the patients past medical histories; 44.9% suffered from gonorrhea. On clinical examination, the findings were: Varicocele in 23% of the cases, testicular hypotrophy in 9.3% and epididymal cyst in 4.6%. The seminal fluid analysis revealed hypospermia in 30.1% of cases, azoospermia in 33.7%, asthenozoospermia in 75.5% and teratozoospermia in 61.5%. The pH was basic in 46.4% of the cases. Follicular stimulating hormone and testosterone levels were high in 48.1% and 12.5% of cases, respectively. About 31.6% of the cases had the positive chlamydial serological test. Semen culture was positive in 25% of the cases and the main organism isolated was Staphylococcus aureus in 66.6% of the cases.
Conclusion: Male infertility is the cause of couple infertility in around a third of the cases. In this study, we have found various etiologies of causes of male infertility. However, idiopathic causes could be found. Keywords: Cotonou, etiology, hormonal profile, male infertility, semen analysis
How to cite this article:
Hounnasso PP, Avakoudjo JG, Dankoro AS, Yde Soumanou FK, Natchagé G, Agounkpé MM, Toré RS. Male infertility: diagnostic and epidemiological aspect concerning 96 cases in a teaching university hospital of cotonou, benin republic. Niger J Surg Res 2015;16:20-2 |
How to cite this URL:
Hounnasso PP, Avakoudjo JG, Dankoro AS, Yde Soumanou FK, Natchagé G, Agounkpé MM, Toré RS. Male infertility: diagnostic and epidemiological aspect concerning 96 cases in a teaching university hospital of cotonou, benin republic. Niger J Surg Res [serial online] 2015 [cited 2018 Jul 23];16:20-2. Available from: http://www.njsrjournal.org/text.asp?2015/16/1/20/166886 |
| Introduction | |  |
Infertility is defined as inability of a sexually active couple without contraception to have pregnancy after a year.[1] If the woman considered the long time ago as only responsible of the infertility couple nowadays in fact male has found in 30–40%.[2] In Benin the frequent reason of andrology consultation is infertility couple.[3] The aim of this study is to describe the epidemiological and diagnostic aspect of male infertility in Urology and Andrology Department Hubert Koutoukou Maga National University Teaching Hospital.
| Methods | | |
This was a retrospective descriptive study conducted at the Academic Clinic of Urology and Andrology Department of Hubert Koutoukou Maga National University Teaching Hospital in Cotonou. The study period was over 6 months duration (January to July 2014). Inclusion criteria were all male patients who represented at the clinic for paternity desire. Data were retrieved from the medical records of the patients. Data retrieved include: The age, spouses's age, past medical history, type and duration of the infertility, clinical examination findings at presentation, testicular ultrasonography findings, semen analysis parameters, hormonal profile-luteinizing hormone, follicular stimulating hormone (FSH), testosterone and prolactin levels, chlamydia trachomatis serological test result, and semen culture.
| Results | | |
The average age of the patients was 37.2 &± 6.7 years with a range of 23 to 55 years.
Sixty-five (67.7%) of the patients were below the age of 40 years [Table 1].
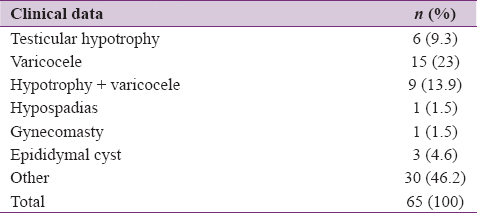
Two-third (66.7%) of the patients' spouses age were above the age of 30 years. Fifty-seven patients (59.4%) had primary infertility. The average duration of infertility was 51 months with a range of 12–180 months. The past medical history, 43 patients (44.9%) and 10 patients (10.3%) had gonorrhea infection and parotid orchitis, respectively. Clinical examination findings revealed 15 cases (23%) of varicoceles, 6 cases (9.3%) of testicular hypotrophy and 3 cases (4.6%) of the epididymal cyst as shown in [Table 2].
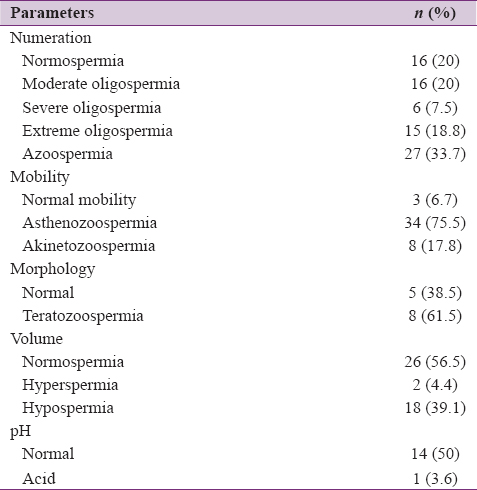
The semen anomalies were: Hypospermia in 18 cases (39.1%), azoospermia in 27 cases (33.7%), asthenozoospermia in 34 cases (75.5%), teratozoospermia in 8 cases (61.5%) and alkaline pH in 46.4% of the patients [Table 3].
Hormonal profile of the patients revealed high serum level of FSH and testosterone in 46 cases (48.1%) and 12 patients (12.5%) of the patients respectively. The chlamydia trachomatis serological test done in 19 of the patients was positive in 6 patients (31.6%). Twenty-four (24) patients' semen cultures were positive in 6 patients (25%) with Staphylococcus aureus isolated in 66.6% of semen cultured.
| Discussion | | |
In Sub-Saharan Africa, couple infertility treatment is a challenge for andrologist and gynecologist. The infertility couple is often young couples' problem within the 1st years of marital life. The average age of the patients is often between 36.4 years and 39 years.[4],[5] This result is near 37.2 years which have found in this study.
Primary infertility is predominant in 59.4% of cases in this study. This result is below to 66.5% noted by Niang et al. in Senegal.[5] This shows the frequency of this disease in both countries which are at Sub-Saharan Africa. Hargreave et al.[4] enumerated gonorrhea among the consulted pathologies which could lead to infertility. In this study, we have found out in the past medical history of patients a gonorrhea in 13 cases and a parotid orchitis in 3 cases. However, Schill et al.[6] talked that after parotid orchitis, fertility recuperation is variable; some men stay barren, and other could need 2 years for spermatozoon production. Thus, this disease may also explain infertility cases in this study.
According to Huyghe et al.,[1] every infertile man or suspected must be object to urology and andrological expertise for searching a potential urogenital anomalies. Therefore, clinical examination is very important before any therapeutic decision. Systematic physical examination of patients led to the findings of varicocele and testicular hypotrophy in some of the patients. Palpable varicoceles (from Grade 1) had been attributed to male infertility.[7] Twenty-three percent of varicocele cases that were reported in this study were higher than 18.5% observed in Germany by Behre et al.[8] This pathology has been shown to be responsible for spermogram anomalies in 35% of infertile men.[9]
The ejaculate volume reflects secretory capacity of accessory sex glands (seminal vesicle, prostate). In this study, hypospermia has been noted in 39.1% of the patients. This was higher than earlier reported value of 22.1% in a study by Hounnasso et al.[10] in the same department. The anomalies of volume ejaculate are many according to Robin et al.[11] Among spermatozoon numeration anomalies, azoospermia was the first position with 33.7%. But in Congo Brazzaville, Locko-Mafouta et al.[12] have found oligospermia in 56% in real sequence. This result would be linked in part to varicocele of which some patients were suffering.
Semen culture test was positive in 37.5%, attesting an evolutive urogenital infection. This result is close to 35% noted by Esfandiari et al.[13] However, it is inferior than that of 49% found by Mehta et al.[14] This difference could be explained by some patients did not do semen culture test.
| Conclusion | | |
Male infertility is responsible for couple infertility in about thirty percent of cases. In this study, we have found various etiologies of causes of male infertility. However, idiopathic causes could be found.
| References | | |
| 1. | Huyghe E, Izard V, Rigot JM, Pariente JL, Tostain J, CCAFU. Evaluation of infertility man: Recommendations of urologist association of france (AFU) 2007. Urol Prog 2008;18:95-101.  |
| 2. | Thonneau P, Marchand S, Tallec A, Ferial ML, Ducot B, Lansac J, et al. Incidence and main causes of infertility in a resident population (1,850,000) of three French regions (1988-1989). Hum Reprod 1991;6:811-6. |
| 3. | Gainsi E, Fourn L, Akpo C. Male infertility and urethral infection in CNHU of cotonou. Medecine d'Afrique Noire 1990;37:472-80. |
| 4. | Hargreave T, editor. Varicocèle. In: Male Infertility. Berlin: Springer Verlag; 2000. p. 83-7. |
| 5. | Niang L, Ndoye M, Labou I, Jalloh M, Kane R, Diaw JJ, et al. Epidemiologic and clinically profil of male infertility at general great yoff hospital of Dakar. Concerning in 492 cases. J Androl 2009;19:103-7. |
| 6. | Schill WB, Comhaire FH, Hargreave TB. CausesSystematic etiologies of male sterility. In: Mahmoud A, Comhaire F, editors. Treaty of Urology for use by clinicians. Paris: Springer-Verlag; 2008. p. 57-61. |
| 7. | Marmar JL, Benoff S. Varicoceles. J Urol 2006;175(3 Pt 1):818-9. |
| 8. | Behre HM, Kliesch S, Schädel F, Nieschlag E. Clinical relevance of scrotal and transrectal ultrasonography in andrological patients. Int J Androl 1995;18 Suppl 2:27-31. |
| 9. | Cho KS, Seo JT. Effect of varicocelectomy on male infertility. Korean J Urol 2014;55:703-9. |
| 10. | Hounnasso PP, Sikpa KH, Avakoudjo JDG, Gandaho I, Yevi M, Ouattara A, et al. Spermiologic profil of men who consult for infertility at cotonou. URO' ANDRO 2013;1:52-9. |
| 11. | Robin G, Marcelli F, Mitchell V, Marchetti C, Lemaitre L, Dewailly D, et al. Why and how to assess hypospermia? Gynecol Obstet Fertil 2008;36:1035-42. |
| 12. | Locko-Mafouta C, Malonga G, Assounga AG, Riviere-Gazeaux H, Silou JM. Male infertility at Brazaville. Médecine d'Afrique Noire 1989;36:325-30. |
| 13. | Esfandiari N, Saleh RA, Abdoos M, Rouzrokh A, Nazemian Z. Positive bacterial culture of semen from infertile men with asymptomatic leukocytospermia. Int J Fertil Womens Med 2002;47:265-70. |
| 14. | Mehta RH, Sridhar H, Vijay Kumar BR, Anand Kumar TC. High incidence of oligozoospermia and teratozoospermia in human semen infected with the aerobic bacterium Streptococcus faecalis. Reprod Biomed Online 2002;5:17-21. |
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for